

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Xenotransplantation refers to transplantation of tissues or organs between different species.1) On January 7th, 2022, a historical event of pig-to-human cardiac xenotransplantation was performed using genetically engineered porcine xenograft and co-stimulation blockade-based immunosuppression.2) Though the patient developed xenograft failure and succumbed to death on post-operative day 60,2) this event shed light on the cumulative effect of scientists and physicians who worked hard to unveil the underlying immunobiology of cross-species organ transplantation.
In this review, we aimed to summarize the historical landmarks of cardiac transplantation (Figure 1, Table 1), to discuss current understandings on the immunobiology of xenotransplantation, and to assess the current limitations to clinical translation.
Figure 1
Historical landmarks of cardiac xenotransplantation.
History of cardiac xenotransplantation rooted from the 1960s, and cumulating advances on immunosuppressive strategies, cross-species rejection biology, and genetic engineering provided solid grounds for the modern history of heart xenotransplantation.
DAF = decay accelerating factor; Gal = α1,3-galactose; HLA = human leukocyte antigen.
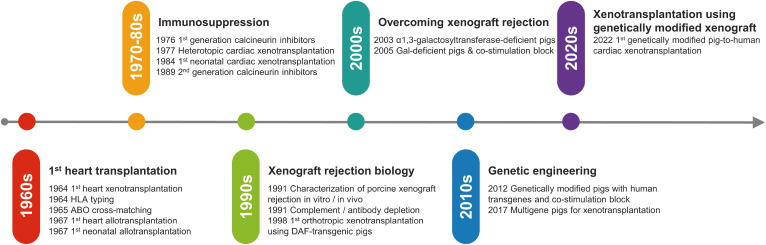
Table 1
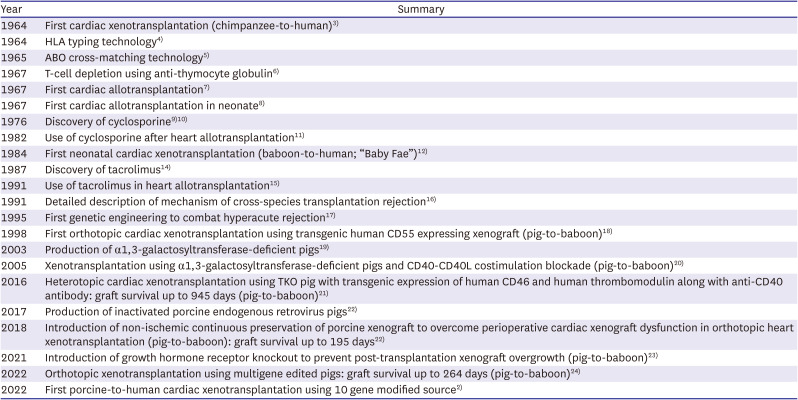
Key events throughout the history of cardiac xenotransplantation
| Year | Summary |
|---|---|
| 1964 | First cardiac xenotransplantation (chimpanzee-to-human)3) |
| 1964 | HLA typing technology4) |
| 1965 | ABO cross-matching technology5) |
| 1967 | T-cell depletion using anti-thymocyte globulin6) |
| 1967 | First cardiac allotransplantation7) |
| 1967 | First cardiac allotransplantation in neonate8) |
| 1976 | Discovery of cyclosporine9)10) |
| 1982 | Use of cyclosporine after heart allotransplantation11) |
| 1984 | First neonatal cardiac xenotransplantation (baboon-to-human; “Baby Fae”)12) |
| 1987 | Discovery of tacrolimus14) |
| 1991 | Use of tacrolimus in heart allotransplantation15) |
| 1991 | Detailed description of mechanism of cross-species transplantation rejection16) |
| 1995 | First genetic engineering to combat hyperacute rejection17) |
| 1998 | First orthotopic cardiac xenotransplantation using transgenic human CD55 expressing xenograft (pig-to-baboon)18) |
| 2003 | Production of α1,3-galactosyltransferase-deficient pigs19) |
| 2005 | Xenotransplantation using α1,3-galactosyltransferase-deficient pigs and CD40-CD40L costimulation blockade (pig-to-baboon)20) |
| 2016 | Heterotopic cardiac xenotransplantation using TKO pig with transgenic expression of human CD46 and human thrombomodulin along with anti-CD40 antibody: graft survival up to 945 days (pig-to-baboon)21) |
| 2017 | Production of inactivated porcine endogenous retrovirus pigs22) |
| 2018 | Introduction of non-ischemic continuous preservation of porcine xenograft to overcome perioperative cardiac xenograft dysfunction in orthotopic heart xenotransplantation (pig-to-baboon): graft survival up to 195 days22) |
| 2021 | Introduction of growth hormone receptor knockout to prevent post-transplantation xenograft overgrowth (pig-to-baboon)23) |
| 2022 | Orthotopic xenotransplantation using multigene edited pigs: graft survival up to 264 days (pig-to-baboon)24) |
| 2022 | First porcine-to-human cardiac xenotransplantation using 10 gene modified source2) |
HISTORY OF CARDIAC TRANSPLANTATION
Early days before modern understanding of transplantation
The first cardiac transplantation was a xenotransplantation using chimpanzee heart into a 68-year-old male with a long history of hypertensive cardiovascular disease, which took place on January 23, 1964 by Dr. Hardy.3) The chimpanzee heart was too small to handle the large venous return and support the circulation, therefore, this innovative movement lasted for 90 minutes. The first heart allotransplantation was performed three years later in Cape Town, South Africa. On December 3, 1967, historical surgery was performed by Dr. Barnard,7) and the 54-year-old male patient survived for 18 days. However, lack of immunosuppression and knowledge on allograft immunology resulted in rapid deterioration, and the patient was succumb to death. Another cardiac allotransplantation took place in Brooklyn, New York, 3 days after Dr. Barnard’s adventure; this was the 1st allotransplantation performed in a cyanotic infant, and the patient died 6 and a half hours postoperatively in severe metabolic and respiratory acidosis.8)
Along with endeavors of cardiac surgeons of the 1960s, the period of time was also noted for milestone discoveries on ABO compatibility, human leukocyte antigen (HLA) typing,4) and immunosuppressive agents. Especially, understanding of ABO compatibility and cross-matching resulted in an improved early clinical outcome of renal transplantation.5) Moreover, after the clinical introduction of 6-mercaptopurine,25) azathioprine was developed and was proved to have a superior impact on the survival of organ graft in animal models.26) Introduction of lymphodepletion using antilymphoid products (nowadays antithymocyte globulin; ATG) further aided in prolongation of canine renal allograft survival.6)
The remarkable discovery of the first generation calcineurin inhibitor (cyclosporine) was a game changer9)10) in the history of cardiac transplantation. By the year of 1982, it was proved that the use of cyclosporine with low-dose steroid is superior to azathioprine and high-dose steroid, in the means of not only early morbid rejection of allotransplanted heart but also infectious complications.11)
The legendary challenge – “Baby Fae” and the first success
On the grounds of medical achievements in 1960s and 1970s, the first cardiac xenotransplantation of baboon heart in a neonate born with hypoplastic left heart syndrome (HLHS) took place on October 26, 1984.12) The infant’s blood type was O, Rh+, which is a very rare phenotype among baboons.27) Pretransplant immunologic testing including lymphocytotoxic crossmatching and mixed lymphocyte cultures showed that the infant’s serum was compatible and was predicted to be a weak responder to xenogeneic lymphocytes. The infant survived for 20 days, becoming the icon of organ xenotransplantation, named as “Baby Fae”. However, the patient ultimately succumbed to humoral factors refractory to cyclosporine-based immunosuppression. Postmortem examination of xenograft showed microvascular occlusions and interstitial hemorrhage, supporting the contribution of humoral rejection.13)
Meanwhile, another historic heart allotransplantation took place a year after “Baby Fae”. The recipient was a male infant born with HLHS, and orthotropic heart allotransplantation was performed using the heart from a brain-dead, ABO compatible infant on November 20, 1985.28) Histocompatibility testing demonstrated compatible lymphocytotoxic crossmatching, and immunosuppression using cyclosporine, azathioprine and prednisone followed. The patient – also known as “Baby Moses” – grew up to be a healthy adult and is still living today.
MODERN-DAY UNDERSTANDING OF XENOTRANSPLANT REJECTION AND OVERCOMING STRATEGIES
Critical breakthrough on cardiac xenotransplantation was achieved by enhanced understanding on the immunobiology of xenograft rejection, novel immunosuppressive drugs, and utilization of advanced genetic engineering (Figure 2). In this section, we will discuss the key obstacles and means to overcome them (Table 2).
Figure 2
Schematic illustration of the genetically engineered cardiac xenograft.
Four genes were knocked out and six human genes were knocked in to produce the genetically engineered cardiac xenograft. This model has overcome major obstacles including hyperacute xenograft rejection and xenograft overgrowth, and proper regulation of complement pathway, coagulation cascade, and inflammatory further aided in the prolonged xenograft survival.
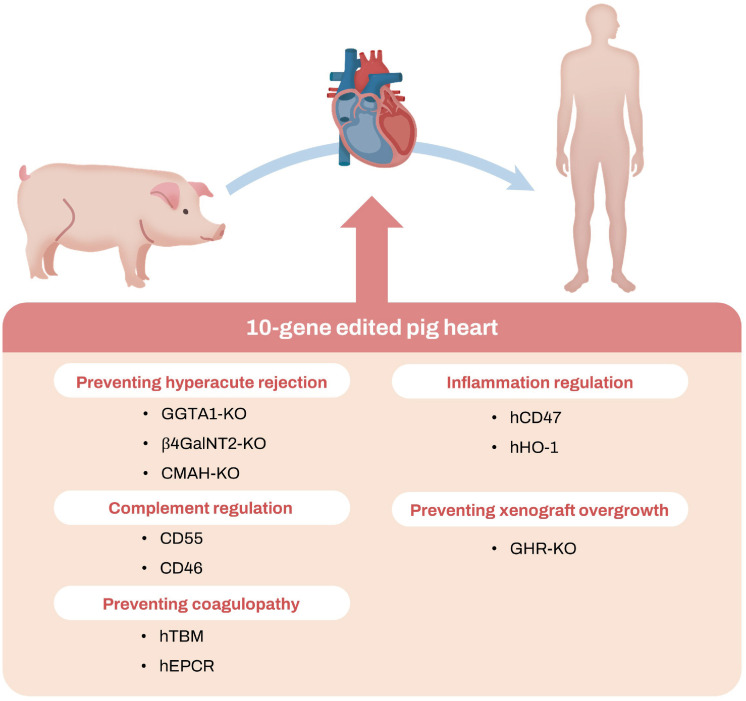
Table 2
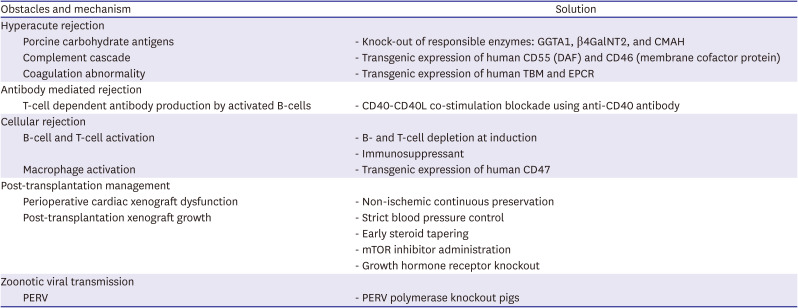
Key obstacles of cross-species heart transplantation and solutions
Overcoming hyperacute rejection
Hyperacute rejection occurs immediately after transplantation, and the culprit factor of this rejection is the natural, preformed antibody in human serum against carbohydrate antigens on xenogeneic endothelial cells.29) The major carbohydrates of porcine endothelial cells are three xenoantigens: α1,3-galactose (Gal),30) SDa blood group antigen (SDa), and N-glycolylneuraminic acid (Neu5Gc).31)32) Following the binding of natural antibodies into these xenoantigens, human complement activation ensues,16) resulting in endothelial cell activation, intravascular thrombosis, and eventually leading to xenograft injury. Histopathologic features of hyperacute rejection includes intravascular thrombosis, interstitial hemorrhage and myocyte death.33)
This antibody-mediated rejection represents inherent immunologic barriers of cross-species transplantation. Endeavors to overcome this obstacle had started as early as 1990s and accelerated by rapid development of novel gene editing technologies including zinc finger nuclease,34) transcription activator-like effector nucleases,35) and clustered regularly interspaced short palindromic repeats (CRISPR).36)37)
Considering the 3 predominant porcine xenoantigens (Gal, SDa, and Neu5Gc) are produced by α1,3-galactosyltransferase (GGTA1), β1,4-N-acetylgalactosyltransferase (β4GalNT2), and N-acetylneuraminic acid hydroxylase (CMAH) respectively, efforts were taken to eliminate these enzymes from the potential xenograft animal models using gene editing technologies. First effort was taken in 2003, producing GGAT1 deficient pigs,19)20) and subsequent pig-to-baboon renal xenograft experiments using GGAT1-knock out donors resulted in prolonged survival of up to 83 days.38) Additional knock out of other major porcine carbohydrate ensued, producing triple knock out (TKO) pig models which lacks GGTA1/β4GalNT2/CMAH genes.39)
Meanwhile, different approaches were also taken by scientists to tackle the step after antibody binding to xenoantigens—the complement cascade. Complement activation and endothelial cell activation still occurred, even in the setting of TKO xenograft model, presumably due to residual antibody binding to minor xenoantigens or as a result of ischemic/reperfusion injury.40) Classical pathway of complement activation starts with antibody binding to xenograft’s endothelial cells and activation of C1 esterase by antibody’s Fc portion; subsequent activation of C3 convertase results in the production of C3b which in turn activates C5 convertase, finally forming the membrane attack complex, which destroys endothelial cells.41) Physiologically, human CD55 (decay accelerating factor; DAF) and CD46 (membrane cofactor protein) cleaves C3 and C5 convertase, thereby maintaining homeostasis. Therefore, to reduce complement-mediated xenograft injury, efforts were taken for transgenic expression of human CD55 and CD46 in pigs, which resulted in improved xenograft rejection-free survival in animal models.18)42)43)44)
Beyond complement cascade, additional genetic engineering technologies were implemented to inhibit porcine endothelial cell activation itself. Under physiologic circumstances, whenever endothelial cell injury happens, heparin sulfate is released from the endothelial cells and human thrombomodulin (TBM) prevent thrombus formation in vivo by activating anticoagulant protein C.45) Endothelial protein C receptor (EPCR) on endothelial cells also augment activation of protein C. To mimic this physiological counterbalance system in the porcine xenograft,46) transgenic expression of human TBM and EPCR was tried, which resulted in significant augmentation of protein C, reduction of graft thrombosis, and prolongation of xenograft survival.47)48)
Overcoming antibody-mediated rejection
After abrogation of risk for hyperacute rejection, major obstacle against successful xenotransplantation lies within the possibility of antibody-mediate rejection49) which occurs within days to weeks after transplantation. This type of rejection is mediated by sensitized antibody-producing cells; antibody production occurs through recognition, processing and presentation of xenoantigens by antigen presenting cells (APCs) by means of major histocompatibility complex (MHC)-peptide complexes. Production of xenoantigen specific antibodies is done by interaction between B cells and CD4+ helper T cells. Throughout this T-cell dependent antibody production by activated B-cells, CD40-CD40L signaling plays the most critical role;50)51) CD40 is expressed on B cells and CD4+ helper T cells express CD40L, and this interaction results in activation of B-cells and production of humoral antibody against the processed antigen.52)
The importance of CD40-CD40L in xenotransplant immunobiology was highlighted by the experiences suggesting the immunosuppressive strategies used in allotransplantation (maintenance therapy using mycophenolate mofetil [MMF], tacrolimus,14) and corticosteroid) were not enough to avoid xenograft.49)53) Instead, xenotransplantation requires blockade of CD40-CD40L pathway; preclinically, this blockade resulted in impaired B-cell activation by xenoantigens, immunoglobulin class switching and germinal center reaction.54) Accordingly, blockade of CD40-CD40L co-stimulation using chimeric 2C10R4 anti-CD40 monoclonal antibody,21) along with MMF, B- and T-cell depletion, and complement depletion has resulted in a marked prolongation of xenograft survival, up to 945 days in a heterotopic xenograft model.55)
Overcoming cellular rejection
Cellular rejection is a T-cell mediated mechanism which occurs when processed xenoantigens by APCs are recognized by cognate receptors, followed by T-cell activation and tissue injury. Swine leukocyte antigen (SLA) is swine counterpart of MHC, and it is known that SLA can provoke and induce human T-cell proliferation, for there exists 70% sequence homology between SLA and HLA.39)56)57)
In addition to T-cells, macrophages also contribute to xenogenic graft rejection. Macrophage activation is physiologically controlled by the inhibitory interaction between signal-regulatory protein alpha (SIRPα) and CD4758) (also known as ‘do not eat me signal’); lack of CD47 on porcine endothelial cells can induce macrophage activation. To ameliorate the actions of macrophages, transgenic expression human CD47 xenografts is implemented in multigene animal models.24)
RECENT SUCCESS AND REMAINING CHALLENGES
Porcine to baboon heterotopic cardiac xenotransplantation
In 2016, a significant improvement was reported in the history of cardiac xenotransplantation. Mohiuddin et al.55) reported that they heterotopically xenotransplanted the hearts from TKO pigs with transgenic expression of human CD46 and human TBM into baboons. Regarding immunosuppressive regimen, they used ATG and anti-CD20 before transplantation to deplete T- and B-cells, and anti-CD40 monoclonal antibody (clone 2C10R4) was also administered for co-stimulation blockade at induction phase. During the maintenance, anti-CD40 antibody, MMF, and corticosteroid administered.
A total of 5 baboons received porcine hearts and marked prolonged graft survivals (median 298 days and longest 945 days) were noted.55) Specifically, humoral rejection and systemic coagulopathy were significantly reduced, which was confirmed by graft biopsy. This success highlighted the key importance of TKO approach, transgenic complement regulation protein expression, and CD40-CD40L blockade in the prevention of xenorejection, paving the way for additional trials including life-supporting, orthotopic cardiac xenotransplantation.
Porcine to baboon orthotopic cardiac xenotransplantation
Subsequent success in orthotopic cardiac xenotransplantation from porcine to baboon followed.22)24) Längin et al.22) used TKO pig model with human CD46 and TBM expression and preserved the graft into non-ischemic preservation with continuous perfusion (NICP) before implantation surgery. NICP was introduced to reduce a complication called perioperative cardiac xenograft dysfunction (PCXD), which will be described in detail later in this review. This approach using NICP resulted in consistent life-supporting function of orthotopic xenograft up to 195 days.22)
Another milestone success used a novel multigene modified pig. TKO model was used as backbone, and additional strategies were implemented24)59): transgenic expression of human CD46 and DAF for complement regulation, human TBM and EPCR for coagulation regulation, and human CD47, and hemeoxygenase 1 (HO-1) for inflammatory modulation. Moreover, knock out of growth hormone receptor (GHR) was also performed to control post-transplantation xenograft growth, which will be discussed later in this review. Immunosuppression was largely similar to the regimen previously used in heterotopic model55): B-, T-cell and complement depletion along with CD40-CD40L signaling blockade during the induction phase, and maintenance using anti-CD40 antibody, MMF, corticosteroids, and anti-inflammatory agents (interleukin-6 inhibitor and tumor necrosis factor α inhibitor). This orthotopic multi-gene xenografts remained highly functional up to 264 days; however, post-transplantation xenograft growth was inevitable despite GHR knockout, still leaving additional challenges behind.24)
Porcine to non-human primate heterotopic cardiac xenotransplantation in Korea
The current research on the cardiac xenotransplantation in Korea will be summarized in 3 aspects. The first is the status of production and breeding of transgenic pigs to be used as donors of the xenotransplantation. The second will be in-vivo testing of the immunocompatibility of pig hearts and the final step would be orthotopic cardiac graft to check the physiologic and functional aspect of the graft heart.
The first part of the research was performed by the National Institute of Animal Science of Rural Development Administration and 2 companies, Optipharm Inc and Mgenplus. They produced various kinds of transgenic pigs for xenotransplantation and the current available transgenic pigs are listed in the review paper.60) Park and associates in 201960) reviewed the history of the research on xenotransplantation in Korea and summarized the contribution of Xenotransplantation Research Center at the Seoul National University Hospital.
The second part of the research was on the heterotopic cardiac graft using porcine hearts to non-human primates. Lee et al.61) started xenotransplantation in 2012 to place the pig heart to Cynomolgus monkey, heterotopically. The aorta of the pig heart was anastomosed to abdominal aorta and the pulmonary trunk of pig heart was connected to the inferior vena cava of the recipients such that the bold perfused coronary arteries through aorta drained to the coronary sinus, right atrial and ventricular chambers to the pulmonary trunk to drain back to the venous system of the monkey. The left ventricular chamber therefore was not used as a pump but the porcine myocardium was perfused by the monkey’s blood. In their experiment 22 monkeys received genetically manipulated pigs’ hearts. The genetic status of pigs was GGTA1 knockout (GalT KO) pigs and 6 of those pigs were additionally expressed with human CD46 or CD39 or CD73. The pigs weighed from 3 to 10 kg, with the hearts weighing 23 to 71 g. Recipients were Cynomolgus monkey, and their body weights were 3 to 7 kg. For transplantation, ABO blood types were matched. For the induction of immune suppression, ATG and rituximab were given preoperatively, followed by maintenance therapy with tacrolimus, mycophenolate mofetil and methylprednisone. Anti-CD154 monoclonal antibody as costimulation blockade and cobra venom factor to inhibit the complement activation were also used postoperatively. The mean graft survival has been 16±16.27 days and the longest survival was 60 days. The mean graft survival was significantly longer in cases since 2014. Double or triple genetic manipulated hearts exhibited significantly better survival (11.63±11.29 days in GalT KO pig; 30.83±20.34 days in double or triple genetic edited pigs; p=0.03). For example, the GalT KO pig with human CD46 expression resulted in the longest survival up to 60 days. Investigation of effective and optimal target genes is important for further progression toward better results is important.
The third part is planned as the orthotopic cardiac xenotransplanation experiments, for which large size non-human primates, such as baboon or chimpanzee, should be available in Korea. Because the body size of Cynomolgus monkeys is small compared to baboon, their chest cage is not enough for the rapid growing pig’s heart. Multiple transgenic pigs especially expressing human thrombomodulin are another obstacle.
The first porcine to human orthotopic cardiac xenotransplantation
On January 7, 2022, a historical first porcine to human orthotopic cardiac xenotransplantation took place.2) A 57-year-old man with a history of hypertension and nonischemic cardiomyopathy developed severe heart failure. Left ventricular ejection fraction was only 10% at presentation, and despite multiple measures including inotropic and intraaortic balloon pump, the patient was subject to venoarterial extracorporeal membrane oxygenation (ECMO). After the approval from the United States Food and Drug Administration, hospital ethics committee, and institutional review board, the patient provided the written informed consent for receiving the first genetically engineered pig heart.
The porcine heart was harvested from the 10-gene edited pig. Four pig genes were knocked out including GGTA1, β4GalNT2, and CMAH to eliminate major pig xenoantigens, and GHR to prevent xenograft overgrowth. Six human genes (CD55, CD46, CD47, HO1, EPCR, and TBM) were knocked-in to control complement cascade, inflammatory reaction, and abnormal coagulation. Immunosuppression regimen included rituximab and ATG for B- and T-cell depletion, and C1 esterase inhibitor to control complement pathway. Anti-CD40 monoclonal antibody (KPL-404) was administered as the mainstay regimen to block CD40-CD40L co-stimulation pathway, accompanied by methylprednisolone pulse. Maintenance by MMT, KPL-404 and tapered methylprednisolone ensued.
Hospital course after xenotransplantation is summarized in Table 3. The first endomyocardial biopsy performed at postoperative day (POD) 34 showed normal histologic characteristics with no evidence of rejection. Starting from POD 43, the patient became more somnolent, and weekly plasma microbial cell-free DNA (mcfDNA) monitoring gradually revealed rising titer of porcine cytomegalovirus (pCMV), suggestive of infection. Diffuse airway ulcerations were noted on bronchoscopy, however, bronchoscopic biopsy did not reveal and viropathic effect with negative staining for Grocott methenamine silver. Intense treatments including antiviral agents ensued, resulting in clinical improvement by POD 47.
Table 3
Clinical course of the first porcine-to-human cardiac xenotransplantation
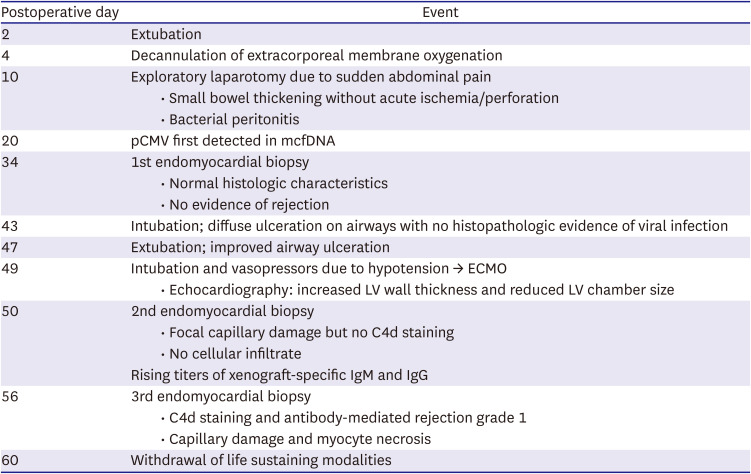
However, by POD 49, sudden deterioration of cardiac function became apparent; left ventricle (LV) thickness was markedly increased leaving reduced LV chamber size. Venoarterial ECMO was initiated, and second endomyocardial biopsy was performed the day after, which showed no evidence of antibody mediated rejection (AMR)62) or acute cellular rejection.63) Instead, focal capillary damage with extravasated red blood cells (RBCs) and interstitial edema were noted, raising concern for the atypical manifestation of AMR, therefore, plasmapheresis was performed along with intravenous immune globulin and rituximab administration.
The third biopsy was performed at day 56, which showed AMR of International Society for Heart and Lung Transplantation grade 162) and myocyte necrosis. Despite the support from ECMO, there was no evidence of change in the graft status by echocardiography, suggesting the irreversibly injury to the xenograft. At POD 60, life sustaining modalities were withdrawn. Postmortem examination of the xenograft was noted by markedly increased heart weight, scattered myocyte necrosis, thin fibrosis, and endothelial cell damage with RBC extravasation.
Though immunologic rejection still remains as the major culprit causing the graft failure, the postmortem findings were inconsistent with traditional knowledge of AMR, in that capillary injury occurred without concomitant complement (C4d) deposition and that no evidence of activated CD68+ mononuclear cells were seen. Moreover, a sudden increase in LV thickness with diastolic dysfunction without systolic failure remains unexplained.2)64) Zoonotic infection by pCMV may have contributed to the failure; though no evidence of viral infection was found at bronchoscopic biopsy, postmortem in situ hybridization revealed the evidence of pCMV infection in the xenograft.64) Though there remain unresolved problems, this historical event illustrates the power of genetic engineering and provides the hope for clinical application of xenotransplantation.
LIMITATIONS TO CLINICAL TRANSLATION
Perioperative cardiac xenograft dysfunction
Apart from immunologic rejections, previous work on xenotransplantation also addressed some important pitfalls and limitations that hinder clinical application of xenotransplantation. One of the limitations include PCXD. PCXD refers to a phenomenon of rapidly developing loss of cardiac function within the first 48 hours of implantation.22) The reported incidence of PCXD ranges from 40% to 60%. PCXD occurs independently of hyperacute of acute rejection, and inflammatory insult from cardiopulmonary bypass system and ischemic-reperfusion injury are regarded as the potential cause of PCXD.22)65)66)
Exciting breakthrough of PCXD emerged by applying NICP when preserving the harvested xenograft until implantation. Xenografts are preserved with hyperoncotic cardioplegic solution which contains packed RBCs, human serum albumin, dextran 40, inotropes, and hormones.22)65)66) The NICP method was the key technique which enabled up to 195 days of orthotopic porcine to baboon graft survival,22) and clinical superiority of this method over crystalloid mediated preservation was further supported by the recent clinical trial of NICP during heart allotransplantation process.67)
Post-transplantation xenograft growth
One of the important reasons why pigs have become the ideal donors for cardiac xenotransplantation is that pigs have similar heart size and anatomy. In the first porcine-to-human heart xenotransplantation, the donor pig weighed 110 kg, and it was assumed that the pig’s heart would be suitable for the 85 kg weighing recipient.2)
However, it is reported that the porcine xenograft continues to grow in the recipient’s body after implantation due to both intrinsic and extrinsic factors.22)68) Variable measures were introduced to reduce this detrimental overgrowth: stringent control of blood pressure, early tapering of corticosteroids to reduce cardiac hypertrophy, and administration of mTOR inhibitor to minimize myocardial hypertrophy.22)
More recently, GHR-knock out strategies were developed, and was proved to be effective even without concurrent administration of additional medications.68) On the grounds of these experiences, the GHR was knocked out in the xenograft in the first porcine-to-human heart xenotransplantation.2) Since the long term data on the growth of this xenograft is lacking, the post-transplantation xenograft growth in human recipients remains to be elucidated.
Zoonotic viral transmission
Zoonotic viral transmission is another obstacle of clinical translation of xenotransplantation,69) for this is closely related with social barriers and major public health concerns. Specific pathogens of concern include porcine endogenous retroviruses (PERVs), pCMV, porcine lymphotropic herpesvirus, and porcine circoviruses. PERVs are most studied microorganism and they are endemic to pigs, thus cannot be eliminated. There are 3 types of PERVs – PERV-A, PERV-B, and PERV-C. Until now, there is no evidence of harmful risk of PERVs to humans, and PERV transmission from porcine to baboon has never been documented.70)71)72)73) However, PERV-A and PERV-B can infect human cells, therefore, concern for zoonotic transmission cannot be underestimated.
Evidence of pCMV in xenografts is associated with reduced xenograft survival according to studies on non-human primates.74)75) pCMV was also detected in the first porcine-to-human heart xenotransplantation by weekly mcfDNA monitoring during the hospital course2) and postmortem in situ hybridization assay,64) however, the contribution of this virus on the clinical deterioration of the patient still remains to be elucidated.
Social and ethical barriers
Major ethical concern regarding xenotransplantation is about animal rights.76) Specifically, putting the rights of human beings above all the rights of the other species could be viewed as too anthropocentric, and growing concern lies on the magnitude and extent of genetic modification. Porcine organs are the most well studied xenograft models, however, handling pigs is forbidden in certain cultural and religious background, therefore fair and proper allocation of porcine xenografts would be very challenging.
Though overall disease burden of heart failure is significant, clinical implementation of xenotransplantation would require markedly higher amount of medical expenditure, for it is based on the combined efforts of complex genetic engineering, donor animal care, costly immunosuppressive medications, and post-operative monitoring and care. In depth cost-effectiveness and cost-benefit analyses should be addressed.
CONCLUSIONS
History of cardiac xenotransplantation rooted from the 1960s. Major advances on xenotransplantation were achieved by understanding the immunobiology of xenograft rejection, the development of immunosuppressive drugs, and the utilization of advanced genetic engineering. Multigene xenograft preparation along with CD40-CD40L blockade successfully resulted in the 60 days of survival in the first pig-to-human cardiac xenotransplantation. The cause of graft failure in this historical challenge is to be elucidated. Although there are several remaining obstacles to overcome, xenotransplantation would become the novel option for millions of patients with end-stage heart failure who have limited options to traditional therapeutics.
 XML Download
XML Download