

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sarcopenia is defined as a decrease in the strength, function, and mass of the skeletal muscle, and this decline has been associated with adverse outcomes such as falls, physical disability, and death.12 Many non-imaging and imaging methods are used to diagnose sarcopenia, with whole-body dual X-ray absorptiometry (DXA), magnetic resonance imaging (MRI), computed tomography (CT), and ultrasonography being the main imaging modalities used for assessment.3 In particular, the cross-sectional area of the psoas muscle at the L3 level can be measured on CT, as it is known to be represent total muscle mass.4 Imaging findings obtained with these methods can demonstrate the severity of sarcopenia.
Sarcopenia is a form of degenerative disease, so the severity of the disease may be related to aging. However, it is also affected by other disease etiologies and the clinical manifestation of sarcopenia may differ according to the severity of each disease. A study of adult patients with cerebral palsy found significant correlation between sarcopenia measured using DXA and a higher Gross Motor Function Classification System (GMFCS) grade.5 Even children with cerebral palsy had muscles that were much smaller than the muscles of typically developing peers according to motor function.67 Besides the decrease in walking speed or grip strength due to sarcopenia, aging can disrupt the balance between the extensor and flexor muscles of the spine, consequently result in scoliosis or kyphosis.89 Several adult studies have reported on an association between sarcopenia and scoliosis, and the degree of sarcopenia evaluated by DXA or multi-frequency bioelectrical impedance analyzer has been positively correlated with the degree of scoliosis.1011 Another previous study revealed a correlation between the sagittal vertical axis and muscle mass measured by MRI and the bioelectrical impedance analyzer.12
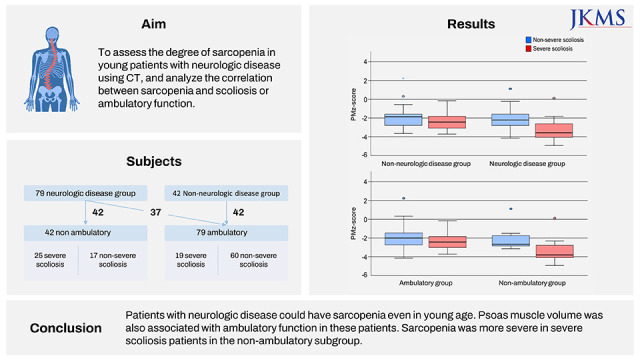
Scoliosis and walking disability are the typical symptoms of patients with neurologic diseases. Scoliosis in patients with cerebral palsy, uncertain brain disorders, myelomeningoceles, or Duchenne muscular dystrophy defined as neuromuscular (NM) scoliosis, because scoliosis related to the neurologic disease is very severe and rapidly progressive in younger children compared with idiopathic scoliosis. Patients with leg length discrepancy or lower leg deformities may have gait deterioration; however gait disability in patients with neurologic disease is different because these disorders causes muscle decrease and imbalance, and change the normal musculoskeletal development.13 No study has yet to examine the relation that sarcopenia has with neurologic disease, scoliosis and gait function in young patients, nor has there been particular research on the degree of sarcopenia measured by the cross-sectional area of the psoas muscle. Therefore, this study aimed to assess the degree of sarcopenia in pediatric patients using CT, and correlate any existing associations between sarcopenia and neurologic disease, severity of scoliosis and gait function.
METHODS
Subjects
From January 2019 to December 2020, pediatric and young adult patients between the age of 4 and 25 years old who underwent non-enhanced whole-spine or lower-extremity CT covering the L3 level were included. The minimum age was 4 years for considering gait maturation and the maximum age as 25 years for excluding degenerative process. Non-enhanced whole-spine or lower-extremity CT was performed to evaluate scoliosis or other lower extremity disorders such as torsional deformity, patellar dislocation, and genu valgum. For patients who underwent multiple CT scans, only the initial examination before surgery was included in the analysis. Demographic and clinical data including age, sex, weight, height, and presence of underlying neurologic disease at the time of the CT examination were assessed. Body mass index (BMI) was calculated using the following formula: weight (kg)/height2 (m2). Patients were divided into either the ambulatory or non-ambulatory group. The ambulatory group consisted patients who could walk with or without assistive devices. The non-ambulatory group consisted of patients who could not walk functionally even with an assistive device, such as a crutch or walker.
CT image analysis
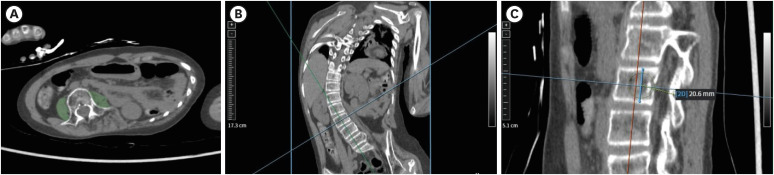
Bilateral psoas muscle area (PMA), a representative value of the degree of sarcopenia, was measured on an angle-corrected axial CT image perpendicular to the L3 vertebral body at the mid L3 level (Fig. 1).314 Skeletal muscle area was additionally measured in patients with images that included full sections of mid L3 level trunk. L3 vertebral height was also measured on an angle-corrected sagittal CT image. To normalize data, the psoas muscle z-score (PMz) was calculated by age and sex.15 As the maximum analytical age of the reference program was 16, data from patients 17 years and older were calculated based on the age of 16. Additionally, the psoas muscle index (PMI) was calculated by dividing the PMA by the square of the L3 height [PMI = PMA/(L3 height)2]. The Cobb angle was measured on the spine radiograph of the shortest interval with the evaluated CT to quantify the magnitude of scoliosis. The Cobb angle of 40 degrees was used to define severe scoliosis.
Fig. 1
Representative images for the measurement of psoas muscle area and vertebral height on CT. (A) Psoas muscle area (green color) measured on an angle-corrected axial CT image (B) perpendicular to the L3 vertebral body at the mid L3 level. (C) L3 vertebral height was also measured on an angle-corrected sagittal CT image.
CT = computed tomography.
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means ± standard deviations and categorical variables were summarized as frequencies and percentages. To compare variables, the independent t-test or Fisher’s exact test were performed. Pearson correlation coefficients were calculated to evaluate the correlation between PMA and skeletal muscle area. And logistic regression analyses were performed to assess the association between sarcopenia and neurologic disease, severe scoliosis and/or ambulatory function. P values less than 0.05 were considered statistically significant.
RESULTS
Subjects
A total of 128 pediatric and young adult (≤ 25 years old) patients underwent non-enhanced whole-spine or lower-extremity CT during the study period. Seven of these patients were excluded because the L3 level psoas muscle was not completely covered on CT images. Therefore, 121 patients were finally included in this study. There were 56 males and the mean age was 12.2 ± 3.7 years (range, 4–24 years).
Patients were divided into two groups according to the presence of neurologic disease. Of the 79 patients with neurologic diseases, 72 had cerebral palsy and 7 had quadriplegia with uncertain brain disorders such as Lennox-Gastaut syndrome. Of the 42 typically developing patients without neurologic disease, 21 had lower extremity torsional deformity, 11 had adolescent idiopathic scoliosis, 9 had recurrent/habitual patella dislocation and one had congenital scoliosis.
There was a significant correlation between skeletal muscle area and PMA in patients with images that included full sections of the L3 level trunk (n = 73, r = 0.928, P < 0.001).
Group comparisons
When patients with and without neurologic disease were compared, height, weight, and BMI were all significantly smaller in patients with neurologic disease (n = 79) than patients without neurologic disease (n = 42) (P ≤ 0.001 for all, Table 1). The PMA was significantly smaller in the neurologic disease group compared with the non-neurologic disease group (890.2 ± 481.5 vs. 1,246.5 ± 754.0 mm2, P = 0.002). The neurologic disease group also showed lower PMz (−2.6 ± 1.1 vs. −2.0 ± 1.2, P = 0.013) and PMI (1.8 ± 0.9 vs. 223 ± 1.0, P = 0.026) compared with the non-neurologic disease group (Fig. 2). When compared between only cerebral palsy patients in neurologic disease and non-neurologic disease group, the results showed similar difference (Supplementary Table 1).
Table 1
Characteristics of patients with/without neurologic diseases or ambulatory function
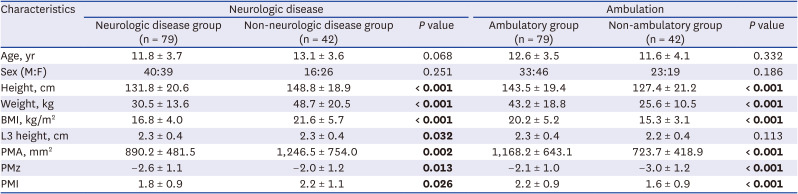
Fig. 2
Box plots that compare psoas muscle parameters such as the (A) PMz and (B) PMI according to neurologic disease and severe scoliosis. Sarcopenia was more severe in patients with severe scoliosis in the neurologic disease group with lower PMz (P < 0.001) and PMI (P = 0.001) being observed compared to patients with non-severe scoliosis.
PMz = psoas muscle z-score, PMI = psoas muscle index.
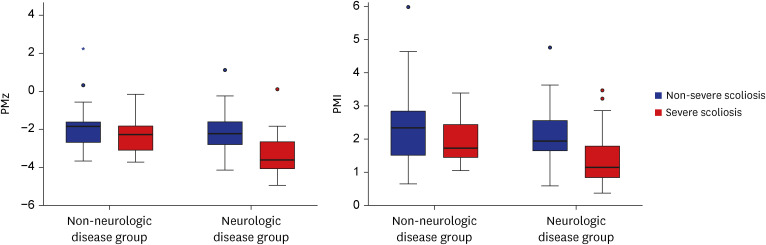
In a subgroup analysis of only neurologic disease patients (n = 79), patients with severe scoliosis (n = 29) were older in age (13.8 ± 3.6 vs. 10.6 ± 3.3 years, P < 0.001), and showed lower BMI (15.1 ± 4.3 vs. 17.9 ± 3.4 kg/m2, P = 0.003), PMz (−3.3 ± 1.1 vs. −2.2 ± 0.9, P < 0.001), and PMI (1.4 ± 0.9 vs. 2.1 ± 0.8, P = 0.001) compared to patients with non-severe scoliosis (n = 50) (Fig. 2). However, in the non-neurologic disease subgroup (n = 42), patients did not show differences in age, BMI, PMA, PMz, and PMI (all, P > 0.05) according to the severity of scoliosis, even though patients with severe scoliosis had lower BMI (19.5 ± 2.8 vs. 23.2 ± 6.7 kg/m2, P = 0.035).
Associations between ambulatory function and psoas muscle parameters
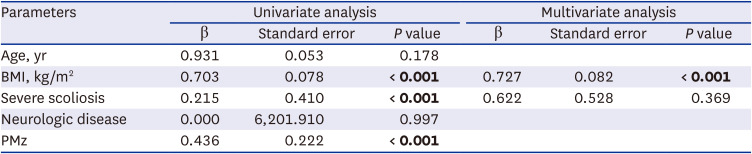
Among all 121 patients, 79 were in the ambulatory group and 42 were in the non-ambulatory group. The ambulatory and non-ambulatory group are compared in Table 1. In the logistic regression analysis comparing the two groups, univariate analysis showed associations between non-ambulatory function with BMI (β = 0.703, P < 0.001), PMz (β = 0.436, P < 0.001), and severe scoliosis (β = 0.215, P < 0.001), but not with age or neurologic disease (Table 2). Multivariate analysis also revealed associations between non-ambulatory function and BMI (β = 0.727, P < 0.001) and between non-ambulatory function and PMz (β = 0.547, P = 0.025). The analysis including only cerebral palsy among neurologic diseases, the results showed similar findings (Supplementary Table 2).
Table 2
Results from logistic regression analysis for non-ambulatory patients
When considering patients only with neurologic disease (n = 79), 37 were in the ambulatory group and 42 were in the non-ambulatory group. The non-ambulatory group also showed lower BMI (15.3 ± 3.1 vs. 18.8 ± 4.2 kg/m2, P < 0.001), PMz (−3.0 ± 1.2 vs. −2.2 ± 0.9, P = 0.001), and PMI (1.6 ± 0.9 vs. 2.1 ± 0.8, P = 0.003) compared with the ambulatory group, even though the age was not different (P > 0.05).
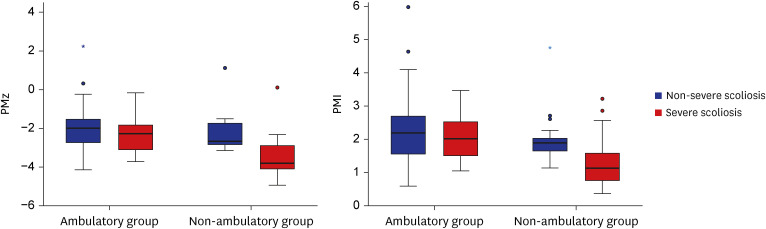
In a subgroup analysis of only non-ambulatory patients (n = 42), who all had neurologic disease, patients with severe scoliosis (n = 25) were older (13.3 ± 3.6 vs. 9.1 ± 3.5 years, P < 0.001) and taller (133.3 ± 18.4 vs. 118.6 ± 22.5 cm, P = 0.025) than those with non-severe scoliosis. However, psoas muscle parameters had lower values in patients with severe scoliosis (PMz: −3.5 ± 1.0 vs. −2.2 ± 1.0; P < 0.001, and PMI: 1.3 ± 0.7 vs. 2.0 ± 0.8; P = 0.004) (Fig. 3).
Fig. 3
Box plots that compare (A) PMz and (B) PMI between the ambulatory function groups. In the non-ambulatory group, psoas muscle parameters were lower in patients with severe scoliosis (P < 0.001 for PMz and P = 0.004 for PMI).
PMz = psoas muscle z-score, PMI = psoas muscle index.
In the ambulatory subgroup (n = 79), patients with severe scoliosis (n = 19) were older (14.5 ± 3.2 vs 11.9 ± 3.4 years, P = 0.004) than those without. However, BMI, PMA, PMz, and PMI did not differ between patients with and without severe scoliosis (all, P > 0.05).
DISCUSSION
There have been many studies about disease status or outcomes associated with sarcopenia in adults, especially in elderly patients.1617 However, sarcopenia is also related to the diverse disease etiology and could be noted even in young individuals. Sarcopenia has been associated with liver disease severity in pediatric non-alcoholic fatty liver disease,18 negative outcomes in children with high-risk hepatoblastoma,19 and higher mortality or postoperative complications after pediatric liver transplantation.202122 However, studies about sarcopenia in children and young adults have been fairly limited. Furthermore, there have been no studies on the relationship between sarcopenia and neurologic disease, scoliosis or gait function in young individuals.
In this study, patients with neurologic disease showed significantly worse sarcopenia, measured by PMz and PMI, than those without neurologic disease. When only patients with neurologic disease were analyzed, both PMz and PMI were significantly lower in those with severe scoliosis than those without severe scoliosis. A decline in ambulatory function was also associated with sarcopenia. Moreover, in non-ambulatory patients with neurologic disease, patients with severe scoliosis showed more severe sarcopenia compared to patients without severe scoliosis. This is the first study to determine the relationship between sarcopenia and ambulatory function or scoliosis in pediatric patients with neurologic disease. Even there have been reports of changes in the psoas muscle imbalance in patients with scoliosis,23 changes due to scoliosis could be excluded by analyzing sarcopenia by the sum of both sides in this study. Also, a strong positive correlation was shown between the skeletal muscle area and the PMA.
A significant decrease in muscle mass and strength is known to occur in patients with cerebral palsy, even in children, which may contribute to the early loss of physical activity and increased chronic health conditions with aging.242526 Patients with other neurologic diseases may also have sarcopenia considering decreased gross motor function. In this study, patients with neurologic disease showed significantly more severe sarcopenia compared to patients without neurologic disease. That is, sarcopenia significantly occurred in children with neurologic diseases, which can cause a rapid decrease in physical activity that presents as gait disability at a young age, and this finding is as significant as sarcopenia observed in the elderly. Research needs to be done to see how the severity of sarcopenia can vary according to different disease etiology. However, the severity of sarcopenia may be related to musculoskeletal symptoms, such as scoliosis or gait disability beyond neurologic etiology.
Pediatric scoliosis can be divided as idiopathic, congenital and NM.27 Congenital scoliosis is caused by a deformed vertebra. The cause of idiopathic scoliosis is not certain, whereas NM scoliosis occurs due to an underlying disease such as cerebral palsy and Duchenne muscular dystrophy that causes muscle decrease and imbalance.13 NM scoliosis differs from other scoliosis in terms of severity, rapid progression, and more perioperative complications.28 In neurologic disease patients, patients with severe scoliosis showed sarcopenia compared with patients without scoliosis, but there was no difference according to severe scoliosis in the non-neurologic group. NM scoliosis may be associated with sarcopenia in young patients because it is related to muscle function.
In adults, a few studies have evaluated the association between sarcopenia and scoliosis.1011 Other spine alignment disorders such as dropped head syndrome, kyphosis, and postoperative proximal junctional disease have been associated with sarcopenia.12293031 Any reduction of muscle mass can disrupt the balance of paraspinal muscles responsible for maintaining spine alignment and cause kyphoscoliosis.832 Although other methods to measure muscle mass such as DXA or bioelectric impedance were not utilized in this study, our results are consistent with these previous studies associating sarcopenia and degenerative scoliosis, considering that scoliosis in patients with neurologic disease can also be due to the imbalance of the antagonist muscles around the spine from sarcopenia. We may similarly apply the association between sarcopenia and degenerative spine disease to the relationship between sarcopenia and NM scoliosis in young patients.
When considering gross motor function, in a past study of 80 adults with cerebral palsy, sarcopenia as measured by DXA was significantly correlated with poor GMFCS, although there was no difference in the prevalence of scoliosis when patients were grouped by sarcopenia.5 This report is consistent with our findings that showed a significant association between non-ambulatory function and PMz, even in young patients. Ambulatory function may be predicted with psoas muscle parameters. Another interesting finding of our study was that sarcopenia was severe in patients with NM scoliosis in the non-ambulatory subgroup. We could not determine whether the severe sarcopenia in non-ambulatory patients with scoliosis was the cause or result of NM scoliosis. However, there was small difference in motor function within non-ambulatory patients in terms of rolling, crawling or head control. The maintenance of motor function is the principle of treatment for neurologic disease and disability. Therefore, sarcopenia may be a red flag for the development of severe scoliosis.
Our study has several limitations. First, the PMz used in this study was calculated using a reference based on data collected from Canadian children, who are reported to be of higher weight and height than our study population, so it is possible that the degree of sarcopenia was overestimated. However, since we normalized the PMI to each patient's lumbar vertebral height for analysis, and the PMI showed the same trends as PMz, we can assume that this did not affect the correlation analysis between sarcopenia and other factors. Second, all children without neurologic disease included in this study had scoliosis or torsional deformity in the lower extremities, so there were no normal controls. Further studies including children with normal muscle mass may be needed for reference. Third, NM scoliosis can be classified into the spastic and flaccid type according to the neurologic disease, and the correlation between sarcopenia, scoliosis and motor function may depend on the type of scoliosis, but this study did not analyze the conditions separately. In addition, patients with a diverse neurologic disease were analyzed as one group, although we included only neurologic disease related to the central nervous system. However, in the subgroup analysis of patients with only cerebral palsy, PMz was still lower than the non-neurologic group. Further studies with larger study populations are needed to further validate our findings for each specific disease. Finally, because this was a cross-sectional study, a causal relationship cannot be determined although we can illustrate the associations between sarcopenia and neurologic disease, scoliosis, or ambulatory function. Further research is needed to confirm whether scoliosis or motor function can be improved through the treatment of sarcopenia.
In conclusion, pediatric and young adult patients with neurologic disease could have sarcopenia. A decline in ambulatory function is associated with BMI and sarcopenia in these patients. In non-ambulatory patients with neurologic disease, patients with significant scoliosis have severe sarcopenia. Further research is needed on the causal relationship of these changes.
 XML Download
XML Download