

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Spontaneous subarachnoid hemorrhage (SAH) accounts for 2–7% of all strokes that result in high mortality and morbidity.1 The yearly incidence rate of SAH is approximately 6/100,000 people in developed countries.2 Among the various causes of this devastating disease, ruptured intracranial aneurysm is the most serious cause that accounts for 85% of the cases.1 Over the past few decades, great advancements was achieved in diagnostic methodology, perioperative management, and treatment modality including endovascular techniques like pipeline devices in SAH patients. In spite of these improvements, the clinical outcome for aneurysmal SAH (aSAH) patients remains poor; approximately 40% of SAH patients die within 4 weeks of admission to the hospital,3 30% of survivors have severe morbidity requiring them to depend on others for daily living,4 and 50% of survivors develop cognitive dysfunction.5
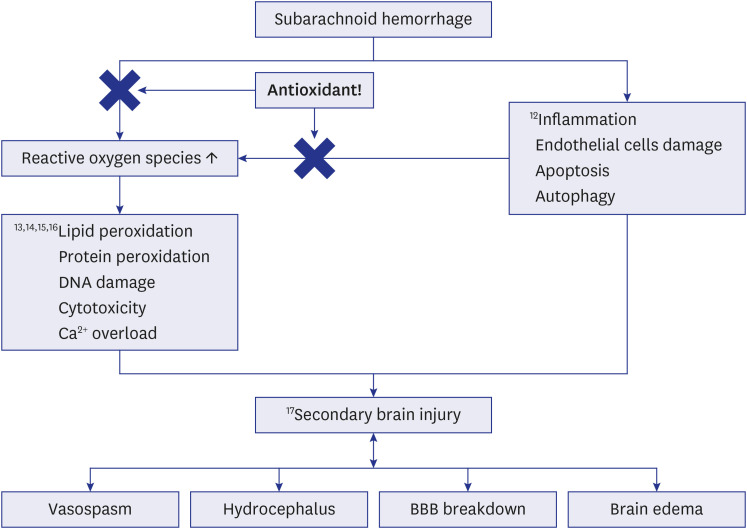
SAH patients have oxidative stress (OS). Increasing evidence supports the role for systemic OS in SAH patients.67 When a brain hemorrhage begins, edema develops and surrounds the hematoma.8 During this process, hemorrhagic clots releases toxic substances like thrombin and iron causing the development of perihematomal edema (PHE) via the oxidation process.9 Hence, antioxidants may reduce the PHE by blocking various cascades in the oxidation process. OS even affects the post-rupture state of an aneurysm in the process of vasospasm, delayed ischemic neurological deficits, and even hydrocephalus (Fig. 1).61011121314151617 Given the supporting data regarding OS biomarkers in SAH, numerous preclinical and clinical studies evaluated its pathophysiology in SAH and assessed the efficacy of targeted antioxidant treatment. Nevertheless, conflicting results were obtained as some studies yielded beneficial effects of antioxidants,1118 whereas other studies failed to confirm such an effect.19
Mounting evidence supports the impact of systemic OS in the development and manifestation of critical illness. Initially, the concept of OS was adopted in critical conditions like acute respiratory distress syndrome (ARDS), systemic inflammatory response syndrome (SIRS), sepsis and shock.202122 In these trials, acetylcysteine and selenium are the most studied antioxidants.23 However, in neurocritical situations, like aSAH, most trials have focusing on antioxidants like edaravone,24 tirilazad mesylate,2526 nicaraven,19 or ebselen.11 Therefore, we postulated that the administration of acetylcysteine and selenium may diminish free radicals, thereby providing a neuroprotective effect that can improve clinical outcomes in aSAH patients. Our a priori hypothesis is that our antioxidants will play a crucial role in the acute period of aSAH by affecting the complex OS system in the human body.
METHODS
Study design and participants
Patients were enrolled from January 2017 to October 2019. The selection of participating hospitals was initiated within the neuro-intensive care unit (ICU) section of the Korean Society of Intensive Care Medicine, with the identification of investigators which have thereafter selected any potential ICUs with neurosurgical facilities and an adequate number of patients with aSAH admitted per year.
The inclusion criteria to be enrolled in the present study were as follows: 1) diagnosis of aneurysm rupture SAH based on computed tomography (CT) and CT angiography (CTA); 2) age ≥ 18 or ≤ 80 years; and 3) expectation to stay in the ICU for > 48 hours. The exclusion criteria were as follows: 1) trauma related hemorrhage; 2) patients on medication of antiplatelets (aspirin, clopidogrel, or cilostazol) or anticoagulation (heparin or low-molecular weight heparin, vitamin K antagonist (warfarin) or direct oral anticoagulants); 3) pregnancy; 4) seizure or status epilepticus disorder requiring anticonvulsant medication; and 5) medically ill conditions that may affect the clinical outcome (i.e., liver cirrhosis, post-cardiac arrest, imminent death or do not resuscitate ordered patients and so on).
The primary outcome was a neurological outcome assessed at 30-days using a modified Rankin scale (mRS).27 Secondary outcomes were divided into clinical and radiological values. The clinical outcomes were the time to reach target sedation level (using the Richmond agitation sedation scale [RASS], target of −2 to 0), need to perform tracheostomy, and total duration of hospital and ICU stay. The radiologic outcomes were serial changes in mid-line shifting due to PHE on CT and the incidence of vasospasms.
Study intervention
Eligible patients were randomly assigned to receive either antioxidants or matching placebo solutions. Randomization was performed in a 1:1 ratio, without stratification and using a block size of 4, by means of a computerized central internet-based allocation service based on computer-generated random numbers. Study investigators were aware of the randomization results whereas enrolled patients were blinded to the result of study drug randomization. The antioxidants used were acetylcysteine (2,000 mg [1,000 mg twice daily {BID}] intravenously [IV] per day) and selenium (1,600 µg [800 µg BID] IV per day). The control group received IV placebo. Antioxidants were given as soon as possible on the day of admission (within 24 hours of admission) for 14 days. These intravenous antioxidants were administered in addition to standard nutrition. Serum selenium level (normal range: 5.8–23.4 µg/dL) was checked twice weekly for 14 days. If the selenium level was higher than the upper limit, administration was discontinued and the level was assessed on the next day to determine the administration. There is no available test to check serum acetylcysteine levels.
Data collection and definition
Relevant data were obtained from the medical records by a neurosurgeon and trained research nurse. The following factors were analyzed: 1) age; 2) sex; 3) comorbidities: hypertension (previous hypertension diagnosis or taking related medication), diabetes mellitus (previous diabetes mellitus diagnosis or taking related medication), hyperlipidemia (total cholesterol ≥ 240 mg/dL, triglyceride ≥ 200 mg/dL, high-density lipoprotein cholesterol ≤ 40 mg/dL, low-density lipoprotein cholesterol ≥ 150 mg/dL, or lipid-lowering medication use), ischemic heart disease (previous diagnosis of angina or myocardial infarction or related medication in use), chronic kidney injury; 4) Hunt and Hess grade28 on admission; 5) treatment modality: microsurgery or endovascular; 6) admission scores (the worst of the first 24 hours) including Glasgow coma scale (GCS), mRS and RASS; 7) time interval between last normal time to hospital admission (hours); 8) baseline blood test results (blood pressure, glucose, total cholesterol, platelets, activated partial thromboplastin time, prothrombin time, and international normalized ratio); 9) use of osmotic agents (mannitol or hypertonic saline); 10) angioplasty for vasospasm; and 11) hydrocephalus on admission. Agitation and sedation levels were examined using the RASS. Our target RASS score was between −2 and 0.
All patients underwent CT and CTA upon admission followed by a transfemoral catheter angiography for treatment decisions (microsurgery vs. endovascular). The collection of radiologic data included: 1) location of ruptured aneurysm (internal carotid artery, anterior cerebral artery, middle cerebral artery, posterior cerebral artery, anterior inferior cerebellar artery, posterior inferior cerebellar artery, and basilar artery); and 2) modified Fisher grade29 for distribution and pattern of SAH.
Serious adverse events (SAEs) were prespecified and had to be reported within 48 hours of identification; 1) pneumonia or ARDS; 2) gastrointestinal bleeding; 3) acute myocardial ischemia or heart failure; 4) cardiac arrest 5) acute renal injury; 6) venous thrombotic events (deep vein thrombosis or pulmonary thromboembolism); 7) sepsis (evidence of an infection and organ failure attributed to it) or septic shock (mean arterial pressure < 65 mmHg despite fluid resuscitation requiring inotropics or vasopressors); and 8) disseminated intravascular coagulation.
Radiologic evaluation
To evaluate the radiological impact of antioxidants in aSAH patients, we selected patients according to their hemorrhage distributions (i.e., modified Fisher grade). Since modified Fisher grade 4 patients have localized intracerebral hemorrhage (ICH) or intraventricular hemorrhage with diffuse SAH, we measured the volume of hematoma, PHE and PHE ratio on post-operative day 0, 7 and 14 for these patients. PHE ratio was defined as the differential value between hemorrhage and PHE volume. The diagnosis of vasospasm was dependent on both clinical and radiological basis.3031 CTA, magnetic resonance angiography (MRA) or transcranial doppler (TCD) ultrasonography were adopted for the radiological diagnosis of vasospasm. The definition of vasospasm in the present study were as follow32; 1) symptomatic vasospasm, defined as clinical deterioration deemed secondary to vasospasm after other causes were eliminated; 2) delayed cerebral ischemia, defined as symptomatic vasospasm, or infarction on CT attributable to vasospasm; 3) angiographic spasm, as seen on digital subtraction angiography; and 4) TCD spasm, defined as any mean flow velocity > 120 cm/sec. The diagnosis of increased intracranial pressure (ICP) includes non-invasive methods like neurologic examination, CT or magnetic resonance (MR). Invasive methods include external ventricular drainage with measurement of ICP greater than 20 mmHg for more than 5 to 10 minutes.33 We also measured the midline shift measurement by drawing a vertical line from anterior of the falx cerebri to posterior insertion. A perpendicular line was drawn to the vertical line and measured from the line to the septum pellucidum, at the level of the foramen of Monro. To minimize measurement errors, the measurements were performed by two board-certified neurosurgeons who were blinded to treatment assignment and the mean value was documented. Hemorrhage and PHE were volumetrically measured with CT using 1.5 to 5 mm-thick slices; the slices were processed using software developed in-house (AsanJ, based on a plug-in package for ImageJ [https://rsbweb.nih.gov/ij]).
SAH management and follow-up
The fundamental management of SAH was performed according to standard guidelines.31 Surgical decisions including treatment modality and techniques were at the discretion of the attending neurosurgeons or neurointerventionists. Microsurgery or endovascular treatments were performed within 24 hours of admission. Fentanyl (0.5–5 µg/kg/hour) or remifentanil (0.025–0.2 µg/kg/min) IV was administered in cases where continuous analgesics were needed. CTA or MRA was performed whenever vasospasm was suspected. The medical treatment of vasospasm was in accordance with SAH guidelines.31 Patients with vasospasm refractory to medical management were treated with angioplasty using infusion of intra-arterial vasodilating agents like nicardipine. The prophylactic anticoagulants were not administered in the study enrolled patients. Instead, intermittent pneumatic compression and bedside physical therapy were applied to all patients with risk of thrombosis. Discharge from ICU and transfer to general ward is indicated if the patient’s vital functions are stable without the intensive care support and no longer require monitoring or treatment.
Statistical analysis
Among various antioxidants, the effect of acetylcysteine and selenium in aSAH patients has not been well studied. Also there were no studies focusing on the same endpoints as the current study to date. Accordingly, we estimated the sample size from past studies which have included other antioxidants targeting ICH patients. Based on an expected effect size of antioxidants in aSAH patients (0.6), assuming 5% lost to follow-up, 106 subjects need to be randomized 1:1 antioxidants vs. placebo afford 85% power to demonstrate with a 2-sided α of 0.05. The expected effect size of 0.6 was derived from the study results administrating statin (antioxidant) to ICH patients. Cohen’s D effect size calculation was used to calculate the expected effect size.
Categorical data were analyzed using the Pearson χ2 test or Fisher’s exact test whereas Student’s t-test was used to compare quantitative data. All values are presented as mean with standard deviation or median (interquartile range 25th to 75th percentile). Univariate analysis was performed with clinical factors of interest. Subsequent stepwise multivariate logistic regression analysis was performed to assess the association between the antioxidant and these factors. Backward elimination (95% confidence interval, CI) method was used to determine the final model, in which all remaining factors had a P < 0.15. All statistical analyses were performed with the use of SPSS (version 21; SPSS Inc., Chicago, IL, USA) and SAS 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was considered when P value < 0.05.
Ethics statement
This prospective, multi-center, singled-blind, randomized study was developed by Korean neuro-ICUs with approval from the Institutional Review Board (Asan Medical Center, 2019-1337). Written informed consent was obtained from all participants, families, or their legal representatives before enrollment in this study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. We confirm that our clinical trial was registered and approved according to the clinical research information service. This is a randomized clinical trial, registered at the Clinical Research Information Service (CRIS, http://cris.nih.go.kr, unique identifier: KCT0004628).
RESULTS
Characteristics of study groups
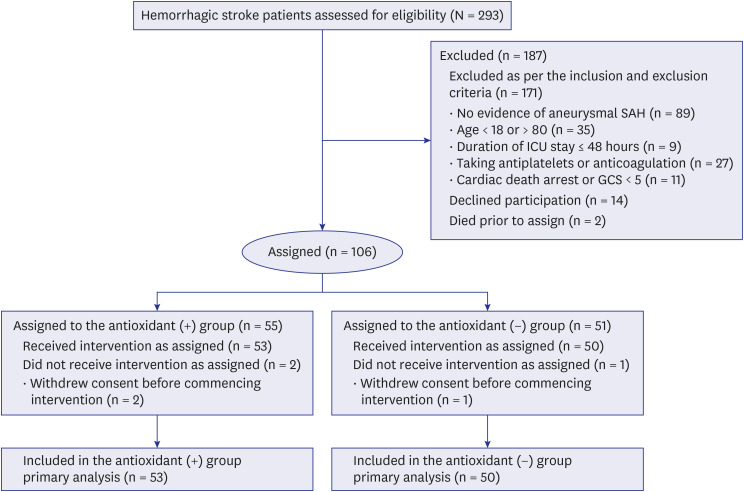
We prospectively screened 293 SAH patients between January 2017 and October 2019 from three different tertiary medical centers. Among these patients, 187 were excluded as per the inclusion and exclusion criteria (n = 171), declining to participate in the study (n = 14) or death prior to assignment (n = 2). Accordingly, 106 patients were included in the assignment of antioxidants, but 3 patients withdrew consent before commencing intervention. Finally, 103 aSAH patients were included in the present study. Among these patients, 53 were assigned to the antioxidant group and 50 to the non-antioxidant (placebo) group (Fig. 2).
There were no significant differences in admission factors between the antioxidant and non-antioxidant groups; age (57.20 ± 16.22 vs. 59.01 ± 13.22 years, P = 0.511), male sex (21 vs. 24, P = 0.843) and Hunt & Hess grade (grade 1, 26% vs. 18.9%; grade 2, 30% vs. 34%; grade 3, 26% vs. 24.5%; grade 4, 14% vs. 22.6%; and grade 5, 4% vs. 0%, P = 0.476). Radiologic assessments of ruptured aneurysm locations (internal carotid artery, 36% vs. 32.1%; anterior cerebral artery, 24% vs. 28.3%; middle cerebral artery, 18% vs. 22.6%; posterior cerebral artery, 16% vs. 9.4%; anterior inferior cerebellar artery, posterior inferior cerebellar artery and basilar artery, 6% vs. 7.5%, P = 0.149) and modified Fisher grade (grade 1, 2, and 3, 66% vs. 64.23%; grade 4, 34% vs. 35.8%; P = 0.846) showed no differences. There was also no significant difference in the type of operations performed between the groups (clipping, 52% vs. 52.8%; bypass and clipping, 4% vs. 5.7%; bypass and trapping, 6% vs. 3.8%; decompressive craniectomy, 12% vs. 15.1; coil embolization, 33% vs. 30.2%; bypass and coil embolization, 2% vs. 3.8%; and trapping 4% vs. 3.8%, P = 0.132). No significant differences were observed in admission neurologic score (GCS 11 [7–14] vs. 10 [7.5–14], P = 0.194 and mRS 4 [3–5] vs. 5 [3–5], P = 0.237), agitation (RASS −1 [−3–0] vs. −2 [−4–0], P = 0.382). The comparison of SAH managements during ICU admission, such as continuous analgesics (72% vs. 69.8%, P = 0.984) and osmotic agents (mannitol, 38% vs. 39.6%; hypertonic saline, 0% vs. 1.9%; and both 2% vs. 1.9%, P = 0.779) showed no differences. The results are summarized in Table 1.
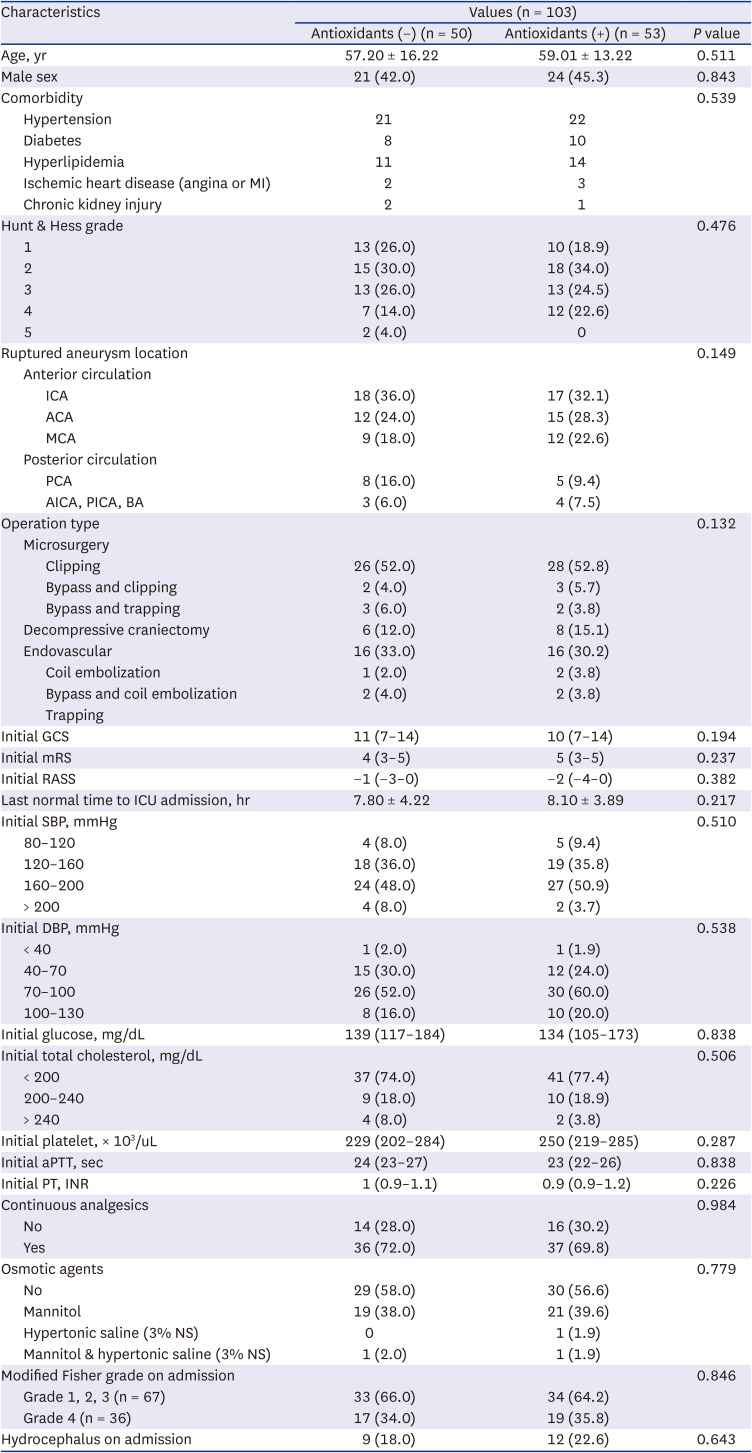
Table 1
Characteristics of subarachnoid hemorrhage patients according to antioxidant administration
Values are presented as number (%), mean ± standard deviation, or median (interquartile range).
ACA = anterior cerebral artery, AICA = anterior inferior cerebellar artery, aPTT = activated partial thromboplastin time, BA = basilar artery, DBP = diastolic blood pressure, GCS = Glasgow coma scale, ICA = internal carotid artery, ICU = intensive care unit, INR = international normalized ratio, MCA = middle cerebral artery, MI = myocardial infarction, mRS = modified Rankin scale, NS = normal saline, PCA = posterior cerebral artery, PICA = posterior inferior cerebellar artery, PT = prothrombin time, RASS = Richmond agitation sedation scale, SBP = systolic blood pressure.
![]()
Radiologic outcome
The radiological impact of antioxidants in reducing PHE were only focused on modified Fisher grade 4 aSAH patients as these patients have localized ICH. CT and CTA scans upon admission showed no differences in the volume of hematoma and PHE causing mid-line shifting and vasospasm. Administration of antioxidants showed no beneficial effects of PHE reduction and midline shifting (Fig. 3). No significant differences in incidence of radiological vasospasm were observed between the two groups at the 1-week (11 patients [22%] vs. 9 patients [17%], P = 0.525) or 2-week (15 patients [30%] vs. 14 patients [26.4%], P = 0.690) radiologic evaluation. The incidence of angioplasty for vasospasm (12% vs. 11.3%, P = 0.916) and diagnosis of hydrocephalus on 2-week CT or MR (26% vs. 28.3%, P = 0.829) showed no differences too. The results are summarized in Table 2.
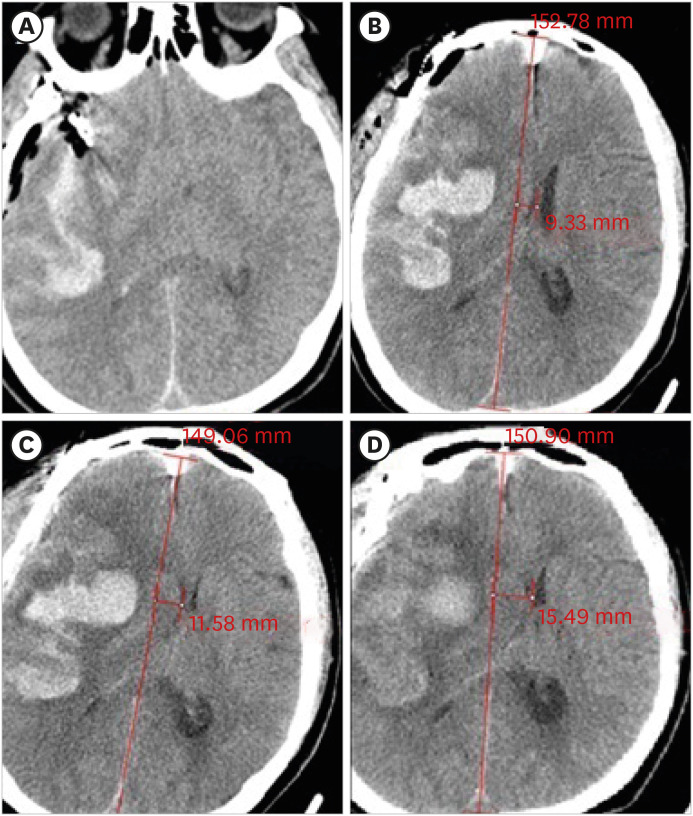
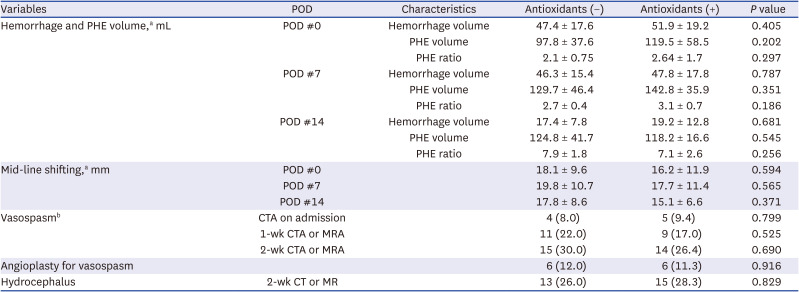
Fig. 3
Non-enhanced brain CT images showing SAH patients with administration of antioxidants. (A) A 74-year-old female patient with aneurysmal SAH due to right middle cerebral artery aneurysm rupture. The patient was treated with craniotomy and clipping of ruptured aneurysm. (B) Post-operative CT on the day of operation showing massive hemorrhage and PHE causing midline shifting (9.33 mm) is observed. Antioxidants were given within 24 hours of admission. (C) One-week follow-up CT shows PHE causing midline shifting (11.58 mm). (D) Two-week follow-up CT showed aggravated PHE causing persistent midline shifting (15.49 mm). The patient underwent decompressive craniectomy for perihematomal edema management.
SAH = subarachnoid hemorrhage, CT = computed tomography, PHE = perihematomal edema.
![]()
Table 2
Radiological outcomes of subarachnoid hemorrhage patients according to antioxidant administration
PHE ratio = PHE volume/Hemorrhage volume.
CTA = computed tomography angiography, PHE = perihematomal edema, POD = post-operative day, MRA = magnetic resonance angiography, CT = computed tomography, MR = magnetic resonance.
aMeasured only for Fisher grade 4 patients (n = 36).
bFor assessment of vasospasm, CTA was performed in surgical clipping cases whereas MRA for coil endovascular treated cases due to coil artifact.
![]()
Clinical outcome
There were no significant differences between the antioxidant and non-antioxidant groups on time to reach target RASS (5.4 ± 3.8 vs. 5.9 ± 4.1 hours, P = 0.122) and the need for tracheostomy (5 [10%] vs. 7 [13.2%], P = 0.284). However, significant differences were observed in total ICU stay (11.6, 95% CI, 9.7–13.4 vs. 8.9, 95% CI, 7.9–10.7 days, P = 0.044) despite no differences being observed in the total hospital stay (24.2, 95% CI, 21.3–27 vs. 22.4, 95% CI, 19.6–26.1 days, P = 0.107). The 30-day neurologic outcomes using mRS were not different between these 2 groups (2.8, 95% CI, 2.1–3.4 vs. 2.4, 95% CI, 1.9–3.1, P = 0.088) (Fig. 4). We further analyzed these factors using multivariate analysis to show the clinical impact of antioxidants. The significant improvements were observed in total ICU stays (11.2, 95% CI, 9.7–14.5 vs. 8.3, 95% CI, 6.2–10.2 days, P = 0.008) but fail to show in total hospital stay (23.2, 95% CI, 20.9–26.5 vs. 21.9, 95% CI, 18.9–24.2 days, P = 0.123) or 30-day mRS (2.6, 95% CI, 1.9–3.3 vs. 2.2, 95% CI, 1.5–2.9, P = 0.105). The results are summarized in Table 3.
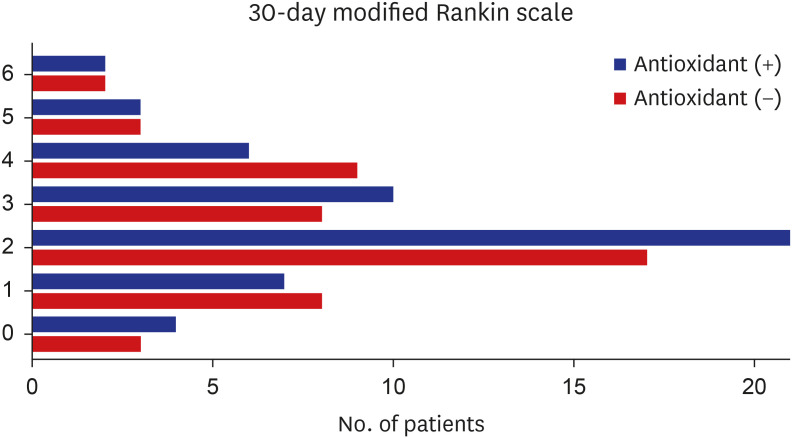
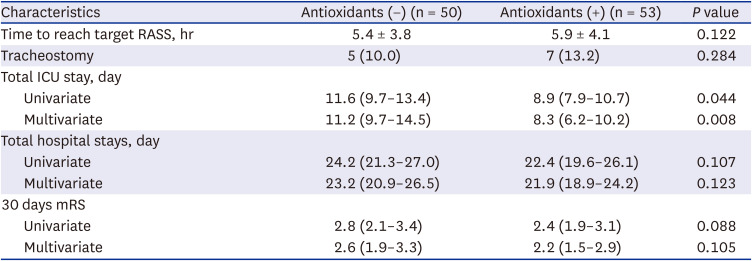
Fig. 4
The 30-day neurologic outcomes using modified Rankin scale between with and without antioxidant treated groups.
![]()
Table 3
Clinical outcomes of subarachnoid hemorrhage patients according to antioxidant administration
Values are presented as mean (95% confidence interval) or mean ± standard deviation.
ICU = intensive care unit, mRS = modified Rankin scale, RASS = Richmond agitation sedation scale.
![]()
SAEs
A total of 19 SAEs were reported in 17 patients and none of them were potentially associated to our antioxidant drugs. The most common SAEs were pneumonia or ARDS (non-antioxidants, n = 6 vs. antioxidants, n = 4, P = 0.450) followed by acute kidney injury (non-antioxidants, n = 1 vs. antioxidants, n = 3, P = 0.341), venous thrombosis events (non-antioxidants, n = 2 vs. antioxidants, n = 1, P = 0.529), heart injury (non-antioxidants, n = 1 vs. antioxidants, n = 1, P = 0.967) and sepsis or septic shock (non-antioxidants, n = 1 vs. antioxidants, n = 0, P = 0.306). No significant differences in the incidence of SAE were observed between the two groups. The results are summarized in Table 4.
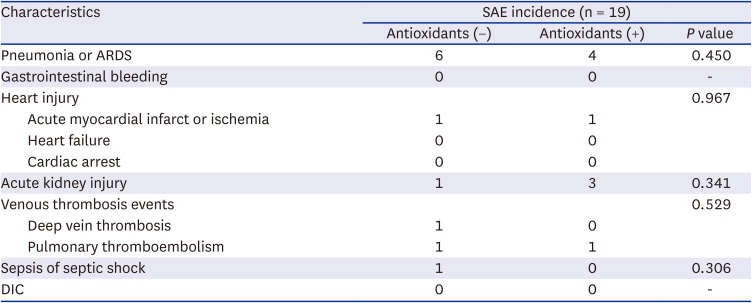
Table 4
Incidence of SAEs in relation to antioxidants administration
ARDS = acute respiratory distress syndrome, DIC = disseminated intravascular coagulation, SAE = serious adverse event.
![]()
Laboratory outcome
The serum selenium levels on admission were within normal limits for both groups (non-antioxidant, 8.4 ± 3.4 vs. antioxidant, 7.9 ± 2.9 µg/dL, P = 0.258). However, the antioxidant group showed a significant increase in serum selenium levels on day 7 (9.2 ± 4.5 vs. 13.5 ± 4.2 µg/dL, P < 0.01) and day 14 (8.7 ± 4.5 vs. 19.6 ± 3.8 µg/dL, P < 0.01) after selenium administration. There were 9 patients whom exceeded the upper limit of serum selenium level after the drug administration (non-antioxidant [n = 5, 10%] vs. antioxidant [n = 7, 13.2%], P = 0.743). The administration was paused for 1 time in all these patients and resumed in the next schedule. The results are summarized in Table 5.

Table 5
Comparison of serum selenium level after selenium administration between antioxidant (−) and antioxidants (+) groups
| Characteristics | Serum selenium level, µg/dL | ||
|---|---|---|---|
| Antioxidants (−) | Antioxidants (+) | P value | |
| Admission | 8.4 ± 3.4 | 7.9 ± 2.9 | 0.258 |
| 7 days | 9.2 ± 4.5 | 13.5 ± 4.2 | < 0.010 |
| 14 days | 8.7 ± 4.5 | 19.6 ± 3.8 | < 0.010 |
![]()
DISCUSSION
In this prospective, multicenter, and randomized trial focusing on the effect of antioxidants (acetylcysteine and selenium) in aSAH patients, we found no significant difference between groups in the primary outcome of neurological scale assessed at the 30-day follow-up using mRS. However, significantly shortened ICU stays was observed in the antioxidants group. No other favorable effect of antioxidants was observed on any other outcome. Importantly, there was no significant harmful effect of antioxidants in our study. The evidence is less clear regarding the significantly shortened length of ICU stay in the antioxidant group. One possible hypothesis is the protective potential of antioxidants improved the functional outcome in acute SAH patients. We failed to show the beneficial effect of antioxidants in the reduction of hemorrhage, mid-line shifting, vasospasm and hydrocephalus. However, antioxidants may have played other roles in cellular level, like relieving mitochondrial dysfunction and SIRS, which can lead to organ dysfunction and hence the longer duration of ICU stay.34 Throughout our study, we determined the merits of acetylcysteine and selenium showing antioxidant neuroprotective properties that mitigate functional outcomes in aSAH patients. To our knowledge, this is the first study focused on the therapeutic effects of combined antioxidants (acetylcysteine and selenium) in aSAH patients that assessed its subsequent clinical and radiological outcomes.
Administration of antioxidants may be effective in aSAH patients for following reasons: 1) vasospasm after aneurysm rupture involves both enzyme and non-enzymatic lipid peroxidation35; 2) elevated levels of superoxide anion and nicotinamide adenine dinucleotide phosphate were observed in preclinical trial of SAH,36 which are the both dominant oxidative stressors; and 3) antioxidants play a crucial role in cerebral ischemia.37 Accordingly, various antioxidants have been evaluated in previous preclinical and clinical studies to examine their potential beneficial effects.1119242526 However, we decided to focus on N-acetylcysteine and selenium for the following reasons. First, these are the most studied antioxidants in experimental and clinical models,23 hence much information is available regarding their safeties and side effects. Second, these antioxidants are inexpensive, simple to deliver, and readily available in most hospitals. In contrast, antioxidants like edaravone24 and tirilazad mesylate2526 have shown beneficial effects in aSAH but are not readily available in all hospitals. Finally, these drugs are commonly used in ICUs for various purposes. For example, the mucolytic effect of acetylcysteine is well-known and generally administered to ICU patients who need lung care for respiratory diseases like pneumonia or ARDS. In fact, SAH patients frequently need mechanical ventilation for lung care due to a high incidence of pneumonia and infection.38 Selenium also ameliorates systemic infection via improvement in immunoglobulin development and phagocytosis.39
Unfortunately, few studies have investigated the benefits of antioxidants in stroke patient showing inconsistent results.1119242526 The present study’s results stand apart from the negative findings of other trials for following reasons: first, previous studies focusing on the effect of antioxidants have developed from smaller and less systematic trials that were limited to experimental studies4041; second, compared to other studies,4243 a much higher dose of antioxidant (1,600 µg per day of selenium) was administered; third, we delivered a combination regimen of antioxidants, unlike the monotherapy used in previous studies1119242526; and last, the antioxidants in our study were administered within 24 hours of admission. Our drug administration time is much earlier comparing to former studies, which were given usually later in the course of admission.4445 Hence, the favorable effects observed in this study may be attributed to the dosing schedule used, suggesting that a high dose in a combination regimen administered shortly after admission may provide superior outcomes.
The optimal dosing schedule of antioxidants in critical patients is unknown. Unlike normal physiologic conditions where the balance between reactive oxygen species (ROS) and antioxidants is maintained, endogenous antioxidants are rapidly reduced after an acute brain hemorrhage resulting in increased OS.46 The majority of antioxidants are greatly reduced shortly after an acute stroke, mainly due to increased OS in the early period.46 A prospective study targeting SIRS patients also showed significant reduction in serum selenium levels soon after the inflammatory cascade initiated.47 Additionally, in a previous meta-analysis comparing administration of high doses of selenium to low doses, a significant reduction in mortality rate was observed.48 Therefore, it is likely that critically ill conditions like SAH are clinically similar to SIRS or sepsis, where there is a great reduction in the serum selenium levels in the acute period. It is possible that the conflicting results of antioxidants from previous trials were likely due to inappropriate timing and suboptimal dosing schedules of the antioxidants. In fact, to achieve pro-oxidant, cytotoxic, and anti-inflammatory effects of supplement drugs, the American Society of Parenteral and Enteral Nutrition recommended high doses of selenium (1,000–16,000 µg per day up to 14 days) to critically ill patients in the acute period.49 Accordingly, we decided to administer a much higher dose of selenium (1,600 µg per day for up to 14 days) compared to former studies.4243 Importantly, the administration of selenium is safe and toxicity is rare,50 and the common side effects of high dose selenium such as vomiting, diarrhea, nail discoloration, and hair loss were not observed in our study.
The combination regimen of antioxidants may represent a valid strategy as they work in synergy and act as basic components of the complicated antioxidant system. For instance, combining two different types of antioxidants, such as lipid-soluble and water-soluble agents may provide synergistic effects.51 For example, the multicenter Scottish Intensive Care Glutamine or Selenium Evaluation Trial, one of the largest and highest quality trials to date using selenium, investigated the effect of combination regimen of antioxidants in critically ill patients.52 In this study, a cocktail method of administrating multiple drugs showed significantly better functional outcome compared to the single drug group. No adverse effect of selenium was observed in this study either. In a prospective randomized study, early multiple antioxidants (selenium, zinc, vitamin C and vitamin B1) were administered to critically ill patients including cardiac surgery, major trauma, and SAH patients.53 Although the beneficial effects of combination regimen of antioxidants were not observed in the SAH patients group, significantly reduced inflammatory response was observed in all other patients.
Recently, some clinical and experimental results of antioxidants including resveratrol, apigenin and paeoniflorin showed favorable results in SAH patients or models.54555657 On the other hand, review and meta-analysis focusing on the antioxidant (selenium) failed to show improved clinical outcomes in the critically ill patients.58 Consequently, as the outcome in SAH patient is heterogeneous and is influenced by a plethora of variable factors, it is difficult to determine the pure effect of antioxidant in SAH patients. Numerous studies implicating OS in the pathophysiology of SAH support to role of antioxidants in these patients.67 ‘A multicenter prospective study involving traumatic brain injury showed that the low serum vitamin E level was associated with unfavorable outcome at 1 and 6 months after the injury.59 They emphasized that vitamin E is a potent antioxidant that administration of this drug resulted in a significant reduction in mortality and improved function outcome. A recent experimental study showed rapid delivery of a potent antioxidant that could decrease neuronal cell death, minimize the levels of ROS, and improve neurologic sequelae following SAH.60 The authors adopted cerium oxide nanoparticles to enhance the antioxidant system and showed significantly improved survival rate and neurological outcomes in the antioxidants group.
In our study, no favorable effects of antioxidants were observed except for the shortened ICU stay. Improved neurological outcome was not observed in our study due to possible causes like suboptimal timing, dosage and combination regimen of antioxidants. Hence, an optimal dose regimen of antioxidants remains challenging to pinpoint as large-scale clinical trials are lacking. In light of this, further research, including larger prospective clinical trials, is warranted.
Some limitations need to be acknowledged in the present study. Given the fact that the centers involved in the present study are all tertiary medical centers, referral biases need to be considered when interpreting our results. Although all of the centers have very similar up-to-date protocols for aSAH management, neurosurgeons or neurointerventionists from different centers may provide different treatments according to their level of expertise. Single blinded study is another limitation. Additionally, trace elements like selenium, zinc or copper that have antioxidant properties and are sometimes given as total parenteral nutrition or enteral feeding were not considered in our analysis. It is important to note that simultaneous multiple drug administration is very common in acute critically ill conditions. Hence, drug interactions may have affected the clinical outcome too. Also, developing study inclusion and exclusion criteria with serum selenium level on admission may help to clarify the role of antioxidants more precisely. Nevertheless, we exclusively focused on acetylcysteine and selenium in aSAH patients that were prospectively designed with a relatively large sample size compared to previous studies.1119242526 The concept of an early and high dose of antioxidants in a combination regimen was already introduced in other critically ill conditions like ARDS, SIRS, sepsis and shock patients.202122 However, to our knowledge, this is the first study to employ this unique concept of administrating antioxidants in neurocritical illness.
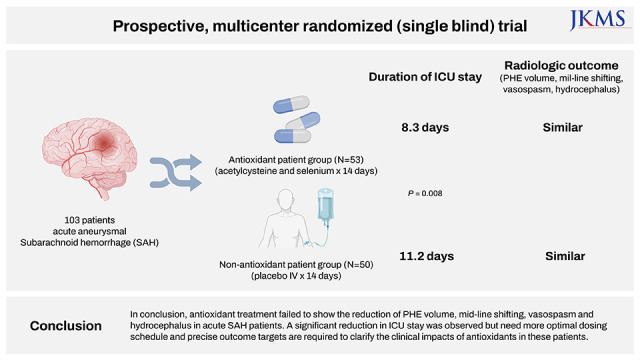
In conclusion, antioxidant treatment failed to show the reduction of PHE volume, mid-line shifting, vasospasm and hydrocephalus in acute SAH patients. A significant reduction in ICU stay was observed but need more optimal dosing schedule and precise outcome targets are required to clarify the clinical impacts of antioxidants in these patients. Our study motivates future research in this area, including a randomized controlled trial of participants with SAH to assess the clinical outcomes with antioxidants administration.
 XML Download
XML Download