

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Most tobacco cigarette smokers continue to smoke because of the addictive nature of nicotine.1 Tobacco cigarette is a harmful nicotine delivery product that exposes smokers to more than 6,000 chemicals, many of which are hazardous to human health.1 Complete cessation is necessary to reduce health risks associated with smoking. However, questions remain about the potential risk of alternative tobacco products such as electronic cigarettes (e-cigars) among continuing smokers who are unable or unwilling to quit smoking.2 In United State, 84% of e-cigar users are current or past tobacco cigarette smokers.3 Approximately 23% of smokers are “Dual Users” who use both tobacco and e-cigars.4
Switching from tobacco cigarettes to e-cigars as a strategy for harm reduction is controversial. E-cigars are electronic nicotine delivery systems (ENDS) that contain many trace elements due to thermal degradation of nicotine derived from tobacco.5 The United States Food and Drug Administration (FDA) recommends reporting harmful and potentially harmful constituent levels in e-cigar liquids and aerosols.5 Although most public health experts agree that e-cigars are less harmful than tobacco cigarette, the number of dual users who have switched to e-cigars and continue to use combustible tobacco cigarettes is not small.6 Several studies789 have shown that e-cigar aerosols typically contain fewer toxic substances in laboratory yields than tobacco cigarettes smoke. However, laboratory results do not necessarily reflect clinically actual individual smokers’ exposure to toxic substances.
The chemical, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK), has been reported by the International Agency for Research on Cancer (IARC) as a group 1 human carcinogen.10 NNK and its metabolite 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) are carcinogenic and contribute to the development of lung cancer in tobacco cigarette smokers.1112 NNAL is a reliable marker for detecting exposure to tobacco smoke and estimating the amount of NNK in the body.131415
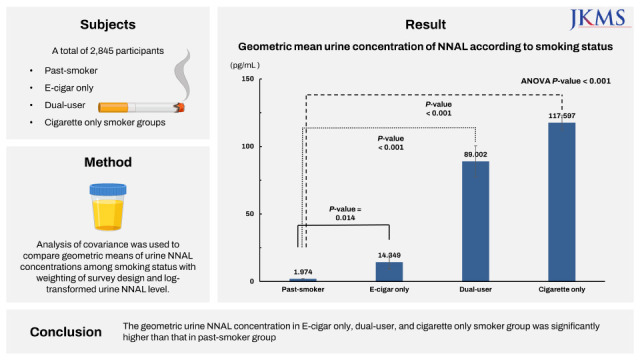
The purpose of this study was to understand the risk of tobacco cigarette, electronic cigarette, and dual users by comparing urine NNAL levels according to smoking status using data of the Korea National Health and Nutritional Survey (KNHANES).
METHODS
Data source
The KNHANES is a representative cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention (KCDC). Twenty-three households from each of 192 districts are sampled every year. A total of about 10,000 household members aged 1 year or older were surveyed. The KNHANES used a complex multi-step probability sample design consisting of stratification, clustering, and systematic sampling based on sex, age, and geographic area to achieve a representativeness of the Korean population using household registries. The KNHANES contains a Health Interview Survey, a Health Examination Survey, a Health Behavior Survey, and a Nutrition Survey known to provide a variety of information about health status, health-related lifestyle information, socioeconomic status, and laboratory results. Trained interviewers conducted face-to-face interviews with the participants. Participants are allowed to refuse to participate in this survey. A written agreement was obtained from the participant upon consent.16 The Disease Control and Prevention Agency of Korea provided detailed information about KNHANES in previous studies.1617
Study population and smoking status
Since urine NNAL concentration in KNHANES has been investigated since 2016, we selected those who had urine NNAL concentration examined in KNHANES from 2016 to 2018. Of a total of 24,269 participants, individuals younger than 19 years of age (n = 4,883), individuals who did not respond to the smoking-related questionnaire (n = 836), individuals who responded that they had never smoked cigarettes in lifetime (n = 11,263), individuals with missing urine NNAL concentration values (n = 4,439), and individuals with urine NNAL concentrations below the detection limit (n = 6) were excluded. Finally, 2,845 participants were included for analysis in this study (Fig. 1).
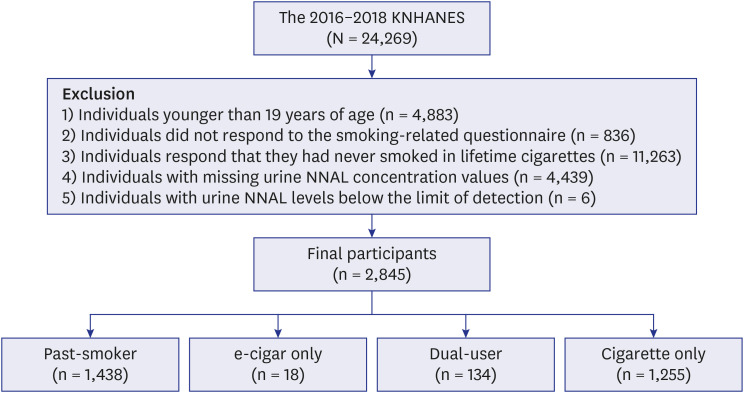
Participants were categorized into the following groups: past-smoker, e-cigar only, dual-user, and cigarette only smoker groups. Those who responded that they ‘do not currently smoke or have not smoked e-cigars’ were classified as past-smoker group. Those ‘who currently smoke and have not smoked e-cigars’ were classified as cigarette only smoker group. Those ‘who currently smoke and have smoked an electronic cigarette in the recent one month’ were classified as dual user group. Those who answered that they were not currently smoking but had smoked e-cigars in the recent one month were classified as e-cigar only group. The pack-years (PYRS) were calculated for each group by multiplying the amount of cigarette smoking (number of cigarette packs smoked per day) by the number of years. Subjects with urine NNAL concentrations more than the median value (21.520105 pg/mL) were defined as the high NNAL group.
Anthropometric measurements
Well-trained staff followed standard procedures to obtain anthropometric measurements. Trained staff measured the participants’ weight and height to the nearest 0.1 kg and 0.1 cm, respectively, while wearing light clothing but no shoes. Body mass index (BMI, kg/m2) was calculated as weight (kg) divided by squared height (m2). Blood pressure was obtained using a standard mercury sphygmomanometer with participants in a seated position and measured by a specialized investigator. Participants' blood samples were obtained from the antecubital vein in the morning after an overnight fast. Serum cholesterol and fasting plasma glucose (FPG) levels were measured enzymatically using a Hitachi Automatic Analyzer 7600-210 (Hitachi, Tokyo, Japan). Urine NNAL concentrations were measured by the HPLC-MS/MS method using an Agilent 1200 Series and Triple Quadrupole 5500 (AB Sciex, Framingham, MA, USA).
Definition of variables
Health-related lifestyle information was obtained from data collected using a self-reported questionnaire. Average monthly household income was calculated by dividing gross monthly house income by the square root of the family size. Sufficient physical activity was defined as individuals who engaged in moderate-intensity activity for ≥ 150 minutes per week or vigorous-intensity activity for ≥ 75 minutes per week. Drinking more than seven cups for men and five or more for women twice a week or more was classified as heavy alcohol intake. Occupational categories include: 1) manual workers, clerk, service and sales worker, person who works for skilled agricultural, forestry, and fishery field, person who operates or assembles craft, equipment, and machine, and elementary worker; 2) office workers, manager, professional, administrator; and 3) others, unemployed persons including housekeepers and students. Education was classified into less than 6 years, 6 to < 9 years, 9 to < 12 years and ≥ 12 years according to educational duration. Marital status was categorized into “married and not separated” and “single”, which included not married, separated, divorced, and widowed individuals. Chronic diseases were consisted of hypertension, diabetes mellitus, dyslipidemia, cardiovascular, and cerebrovascular disease based on the self-reported questionnaire.
Statistical analysis
Continuous and categorical variables are expressed as percentages and mean ± standard error (SE), respectively. All sampling and weight variables were stratified. Statistical analysis is performed using survey analysis of SAS to account for complex sample designs and maintain national representativeness. Analysis of covariance (ANCOVA) was used to compare geometric mean concentrations of urine NNAL and log-transformed urine NNAL level among smoking status with weighted survey design (adjusted for age, sex, pack-years, BMI, cholesterol, FPG, systolic blood pressure [SBP], household income, marital status, education duration, occupation, sufficient physical activity, heavy alcohol-drinking, and chronic disease). Post hoc paired comparison with Bonferroni adjustment was performed using log-transformed NNAL levels according to smoking status. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Two-tailed P value less than 0.05 were considered statistically significant.
Ethics statements
This study was approved by the Institutional Review Board of Chungbuk National University Hospital (CBNUH-2022-03-016). It was conducted following guidelines of the Declaration of Helsinki (1975). The Ethics Committee waived the requirement for informed consent because data were anonymized at all stages, including data clearing and statistical analysis.
RESULTS
Table 1 shows the characteristics of the participants according to smoking status. Unweighted numbers of past-smoker, e-cigar only, dual-user, and cigarette only smoker groups were 1,438, 18, 134 and 1,255, respectively. These groups had mean ± standard deviation ages of 51.7 ± 0.5, 36.9 ± 2.0, 35.7 ± 1.1, and 44.0 ± 0.5 years, respectively. All variables except for cholesterol and physical activity showed significant differences between groups.
Table 1
Participants’ characteristics according to smoking status
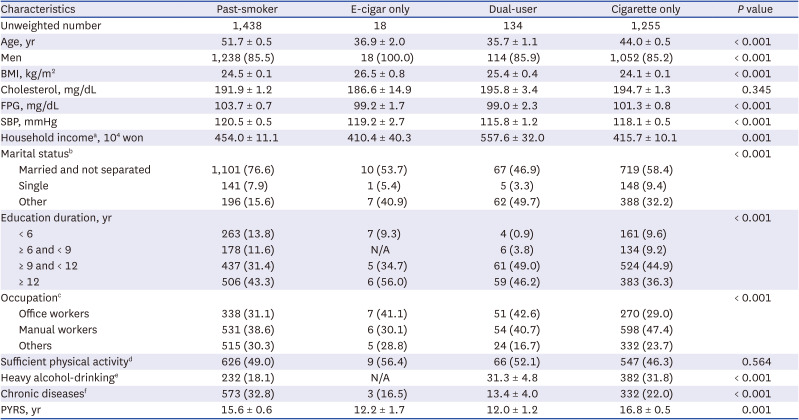
All data are presented as mean ± standard errors or unweighted number (%). SAS survey was adopted for statistical analysis to account for the complex sampling design and to maintain national representativeness. P values were determined by analysis of variance for continuous variables or χ2 test for categorical variables with weighting of survey design.
BMI = body mass index, FPG = fasting plasma glucose, SBP = systolic blood pressure, N/A = not applicable, PYRS = pack-years.
aHousehold income: total monthly house income/square root of number of family members.
bMarital status: married and not separated or single (not married, separated, divorced, or widowed).
cOccupation: office workers (general managers, government administrators, professionals, and office workers), manual workers (clerks; service and sales workers; skilled agricultural, forestry, and fishery workers; persons who operate or assemble crafts, equipment, or machines; and elementary workers), and Others (unemployed persons, housekeepers, and students).
dSufficient physical activity: moderate-intensity activity ≥ 150 minutes /week or vigorous activity ≥ 75 minutes/week.
eHeavy alcohol-drinking: more than 7 cups for men and 5 cups for women more than twice a week.
fChronic diseases: self-reported hypertension, diabetes, dyslipidemia, cardiovascular, or cerebrovascular disease.
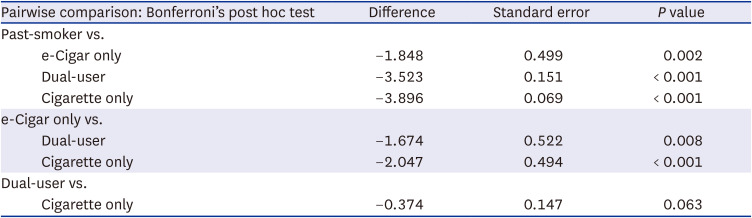
Tables 2 and 3 shows estimated geometric mean concentrations of urine NNAL according to smoking status. Geometric mean concentrations of urine NNAL in past-smoker, e-cigar only, dual-user, and cigarette only smoker groups were 1.974 ± 0.091, 14.349 ± 5.218, 89.002 ± 11.444, and 117.597 ± 5.459 pg/mL, respectively. Even after adjusting for various variables (age, sex, BMI, cholesterol, FPG, SBP, household income, marital status, education duration, occupation, sufficient physical activity, heavy alcohol-drinking, and chronic disease), log-transformed urine NNAL levels showed significant differences among groups (ANCOVA P value < 0.001). Compared with the past-smoker group, log-transformed urine concentrations of NNAL in e-cigar only, dual-user, and cigarette only smoker groups were significantly higher in post hoc test with Bonferroni adjustment (All P values < 0.05).
Table 2
Estimated geometric mean urine concentration of NNAL according to smoking status

Data are presented as mean ± standard errors. ANCOVA was used to compare geometric means of urine NNAL concentration among smoking status with weighting of survey design and log-transformed urine NNAL level adjusted for age, sex, pack-years, BMI, cholesterol, FPG, SBP, household income, marital status, education duration, occupation, sufficient physical activity, heavy alcohol-drinking, and chronic disease.
NNAL = 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol, ANCOVA = analysis of covariance, BMI = body mass index, FPG = fasting plasma glucose, SBP = systolic blood pressure.
Table 3
Pairwise comparison with past-smoker, e-Cigar only, dual-user, and cigarette only by Bonferroni’s post hoc test.
DISCUSSION
This study showed that geometric mean urine concentrations of NNAL varied according to smoking status using nationally representative data. Past-smoker had lower geometric mean levels of urine NNAL than all other group. Dual-user and cigarette only smoker groups showed significantly higher geometric mean levels of urine NNAL in past-smoker and e-cigar only group.
In Korea, the male tobacco smoking rate decreased from 71.7% in 1992 to 39.7% in 2016 and the female smoking rate decreased from 6.5% in 1992 to 3.3% in 2016.18 Although the smoking rate is decreasing, crude incidence rate of lung cancer has steadily increased in both women and men.19 In 2017, the crude lung cancer incidence rate was 52.7 per 100,000 population and age-standardized incidence rate of lung cancer was 27.5 per 100,000 population.19 The lung cancer incidence rate increased with age in both men and women, especially in those over 65 years of age.19 According to the Central Cancer Registry in Korea, lung cancer was the leading cause of cancer death in both men and women (crude rate: 53.5 per 100,000 in men and 19.0 per 100,000 in women) in 2019.20
Carcinogens in tobacco smoke include polycyclic aromatic hydrocarbons (PAH), heterocyclic amines, tobacco-specific N-nitrosamines, aldehydes, cadmium, and many other organic compounds.212223 Among these carcinogens in tobacco smoke, tobacco specific N-nitrosamines and PAH are known to be most closely related to the risk of lung cancer.24 Tobacco-specific N-nitrosamines include N-nitrosodimethylamine (NDMA) and N-nitrosopyrrolidine as well as tobacco specific nitrosamines such as N′-nitrosonornicotine (NNN) and NNK.25 NNK is present in all tobacco products and is considered as a strong lung carcinogen.14 Because NNK is converted to urinary metabolite NNAL, NNAL is considered as a specific biomarker of tobacco exposure.222627 Detection of urine NNAL indicates that the individual has been exposed to certain lung carcinogens with a potential of developing lung cancer in the future.222627
After adjusting for several variables, e-cigar, dual-user, and cigarette only smokers had higher urine NNAL concentrations than past-smokers in this study. E-cigars are often considered a less harmful alternative to conventional cigarettes because e-cigar aerosols contain fewer toxic substances than conventional cigarettes. But, some studies282930 have reported that some trace metallic substances in e-cigar aerosols are higher than those in conventional cigarettes. The e-cigar device consists of a battery and an atomizer containing a chamber and head, which structure has the potential for some trace metallic components to be delivered into the aerosol.31 The E-cigarette or Vaping Use-Associated Lung Injury (EVALI), which can be said to be a representative harmful case of e-cigars, was prevalent from August 2019 to 2020. According to the United States Centers for Disease Control and Prevention (CDC) report, 2,807 hospitalized cases and 68 deaths were reported to be related to EVALI during the period.32 EVALI has been particularly problematic among individuals who use e-cigars that contain tetrahydrocannabinol (THC), the psychoactive component of cannabis.32 Vitamin E acetate additives were detected in the bronchoalveolar lavage fluid in most EVALI patients. However, according to a 2019 report on harmful components suspected to be present in liquid e-cigars in Korea,33 THC was not detected in the liquid e-cigars distributed in Korea; only very trace amounts of vitamin E acetate were detected. Additionally, according to a previous study in 2021 in Korea,34 there may have been no EVALI patients in Korea during 2013–2019. During the period considered in our study (2016–2018), THC was not detected in any e-cigars investigated by the Ministry of Food and Drug Safety in Korea. The toxic effects of e-cigars are still controversial due to the lack of long-term clinical evidence of whether e-cigars are harmful.28 More studies are needed to investigate the harmful effect of e-cigars on human health.
There are several potential limitations to the interpretation of the results of this study. First of all, it was difficult to conclude a causal relationship in this study due to the cross-sectional design. Second, since the data in this study were based on self-reported questionnaires, the possibility of false reporting or recall bias could not be ruled out. Third, since KNHANES is a secondary data, other factors that may affect the concentration of urine NNAL could not be considered. The NNAL levels can also be affected by exposure to environmental tobacco smoke. Workers who harvest tobacco and produce tobacco products may also be exposed through the skin and lungs. These environmental factors could not be considered as data limitations. Additionally, a previous study35 reported that secondhand smoke may increase NNAL concentrations, but secondhand smoke was not considered in this study. Fourth, the operational definition of e-cigar users may be inaccurate. Fifth, because the number of female smokers was too small to be analyzed statistically, sex could not be investigated separately. Instead, we tried to adjust for the effect of gender by analyzing sex as a confounding variable. In addition, although e-cigars vary in shapes, sizes, and type of device, it was not possible to distinguish between various types of e-cigar devices. We could not further stratify for e-cigar types such as heat-not-burn (HNB) tobacco due to data limitations. Finally, since the number of e-cigar users was relatively small, there may be a possibility of selection bias.
Despite these limitations, our study used a population-based sample to generate estimates representative of Korean population. In addition, this is the first study in Korea to investigate urinary NNAL concentration according to smoking status using national representative data. Measuring the actual concentration of NNAL is also a strength of this study.
In conclusion, estimated geometric urine concentrations of NNAL were significantly different according to smoking status. E-cigar only, dual-user, and cigarette only smoker groups showed significantly higher urine NNAL concentrations than the past-smoker group after adjusting for several variables using national representative data. Conventional cigarette users, dual users, and e-cigar users can potentially suffer from harmful health effects of NNAL. Thus, preventive management might be needed for conventional cigarette smokers and e-cigar users through NNAL monitoring.
 XML Download
XML Download