

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sedation is an important procedure of intensive care practice at the time of intubation to minimize oxygen consumption and facilitate mechanical ventilation comfortably.12 Over the past two decades, deep sedation has been reported to be associated with adverse outcomes, such as delayed weaning, increased lengths of intensive care unit (ICU) stay, and increased hospital mortality.34 Especially, early deep sedation during the initial mechanical ventilation period worsens the outcomes.5 Escalating sedation intensity within the first 48 hours of ventilation was independently associated with delayed time to extubation and increased mortality.6 Furthermore, early deep sedation affected the long-term outcomes.7
Recently, an attempt at daily sedation interruption has been conducted in several studies. These trials that compared daily and no sedation interruption reported that patients had a shorter ICU stay in the latter group.89 However, a meta-analysis did not support this approach’s daily interruption of sedation.10 Moreover, the current trial that compared the strategy of no sedation and light sedation and daily interruption showed that none of the outcomes significantly differ between the trial groups.11 As a result, omitting sedation practice in mechanically ventilated patients is incompletely characterized, and the current guidelines for sedation in the ICU recommend monitoring of sedation clinically aiming to achieve light levels of sedation depth.12
Sedation practices in the ICU have drastically shifted as a mounting body of evidence supports the use of light sedation.13 Previously, a frequent over-sedation has been reported in ICUs, and the implementation rate of adequate assessment tools for sedated patients was low.1415 In a recent national survey of Spanish ICUs, most patients underwent a standardized sedation practice and were regularly monitored.16 However, in Korea, the real practice of sedation in ICUs and the impact of deep sedation on clinical outcomes remain unclear.17 Therefore, this study aimed to evaluate the association between early deep sedation within the first 48 hours of mechanical ventilation and clinical outcomes, including the duration of mechanical ventilation, length of ICU stays, and in-hospital mortality in the Korean population.
METHODS
Study design
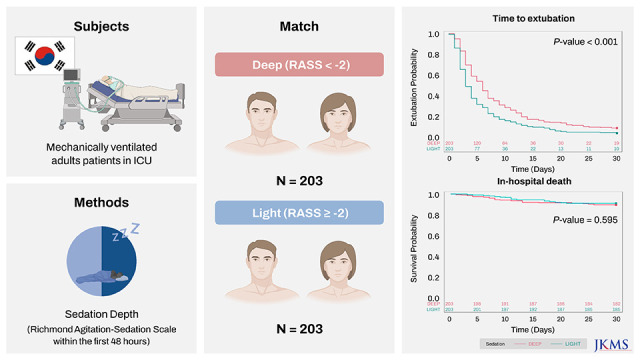
This is a multicenter, prospective, longitudinal, noninterventional cohort study conducted in 20 ICUs in Korea between April 2020 and July 2021. The participating ICUs are presented in detail in the Acknowledgments. During the study period, patients were recruited based on the number of available patients at each ICU. Patients were assessed for inclusion if they underwent mechanical ventilation and sedation practice in ICUs within 48 hours. The inclusion criteria included age of ≥ 19 years and expected sedation and mechanical ventilation for > 48 hours. The exclusion criteria were as follows: patients with a disease that likely leads to death within 90 days, with discontinuation of active treatment due to imminent death or no effective therapy, or with the need for nonselective deep sedation due to medical conditions such as brain damage, brain hemorrhage, spinal cord injury, drug overdose, burns, and nerve root block.
Sedation monitoring
We monitored sedation depth using Richmond Agitation–Sedation Scale (RASS), ranging from −5 to +4, every 8 hours until ICU discharge or day 30.18 The primary variable of interest was sedation intensity within the first 48 hours of mechanical ventilation. The sedation intensity within the first 48 hours was measured as a mean RASS value calculated as the sum of measured RASS values divided by the total number of RASS measurements performed in the first 48 hours. The depth of sedation was divided into light (mean RASS score ≥ −2) and deep sedation (mean RASS scores < −2) based on previous studies.1920
Measurements
During enrollment, baseline demographics, the reason for ICU admission, type of ICU admission, comorbid conditions, illness severity at enrollment (acute physiology and chronic health evaluation [APACHE] II score), and ICU support were collected to characterize the study population. Among the comorbid conditions, we defined severe to moderate liver disease as cirrhosis and portal hypertension with or without variceal bleeding history and severe to moderate chronic kidney disease as serum creatinine of > 3 mg/dL, on dialysis, post-kidney transplant status, or uremia status. The ICU support included vasopressor infusions, renal replacement therapy, and neuromuscular blockade. Clinical outcomes, including ICU discharge, ventilator days, and survival status, were also recorded. To determine the impact of sedation depth, the cohort was divided into two groups (the light and deep sedation). The primary outcome of this study was time to extubation, ICU length of stay, and in-hospital mortality. Time to extubation was defined as the number of days from initiation of mechanical ventilation to extubation. In addition, ICU length of stay was calculated as the number of days from the day of admission to the ICU to the day of discharge from the ICU. Outcomes were compared between the light and deep sedation groups, with the priori hypothesis of deep sedation associated with increased mortality, longer ICU lengths of stay, and greater ventilator duration.
Sample size
For sample size calculation, data reported in previous studies were used.21 Given a maximum risk of type I error of 5%, a sample size of 631 patients (213 and 418 in light and deep sedation groups, respectively) was estimated to provide the study with 90% power to show that the deep sedation group would result in a 50% higher hazard ratio (HR) of the length of days or to reject the hypothesis. A two-sided P value was used for the between-group difference based on the outcome.
Propensity score matching
Propensity score matching was used to reduce the potential confounding in comparing outcomes between the two groups by accounting for differences in covariables. In all patients, the propensity score was calculated for each patient using a multivariable logistic regression model with covariates that may affect the likelihood of sedation depth and outcome of interest, including age, gender, type of ICU, type of admission, APACHE II score, vasopressor infusions, and neuromuscular blockade. Light and deep sedation groups were then paired 1:1 on these propensity scores by the nearest-neighbor matching within an optimal caliper width of 0.1 standard deviations (SDs) of the propensity score. The standardized mean differences were estimated before and after matching to evaluate the balance of covariables, with values of < 10% used to indicate no significant imbalance.
Statistical analysis
Data were presented as numbers and proportions for categorical variables and means ± SDs or medians (interquartile range) for continuous variables. Between-group differences were analyzed using the χ2 test or Fisher’s exact test for categorical variables and independent two-sample t-test or Mann-Whitney U test with normal or nonnormal distribution as appropriate. Data normality was assessed by inspecting histograms. For the time-to-event analysis, the Kaplan-Meier method was used to estimate survival curves, whereas a log-rank test was used to determine significant differences. Uni- and multivariable Cox proportional hazards regression models were used to identify the association between the sedation depth and clinical outcomes. To adjust the observed effects, a list of a priori covariables with known prognostic significance for outcomes was selected for model inclusion: age, vasopressor, and illness severity. These results are presented as HR with a 95% confidence interval (CI). Two-sided P values of < 0.05 indicated significance. All analyses were performed using the SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board of all participating centers (Supplementary Table 1). Although all patients were initially designed to provide their written informed consent, some participating centers’ local review boards waived the need for informed consent when considering the observational nature of this study. This study was performed per the amended Declaration of Helsinki.
RESULTS
Patient selection
From April 2020 to July 2021, 676 patients were enrolled in the study; however, 45 patients were excluded (reasons for exclusion are provided in Supplementary Fig. 1). The final analysis included 631 patients, consisting of 213 (33.8%) and 418 (66.2%) in the light and deep sedation groups, respectively.
Patient characteristics
Table 1 shows the patient characteristics in the two groups. The incidence of deep sedation within the first 48 hours of mechanical ventilation was 66.2%. The baseline patient demographics, including age, gender, and body weight, were similar in the two groups. Among the entire cohort, 29.0% of patients had comorbidity. No differences were observed between the two groups in the type of comorbidity (P = 0.549), except for dementia (1.6% in light sedation vs. 6.7% in deep sedation, P = 0.004). The main source of admission was from medical conditions (48.6%) and emergency surgery (30.5%), with only 20.7% of patients admitted after elective surgery. The type of ICU significantly differs between the two groups. The light sedation group showed a higher percentage of surgical ICU (65.7%) than the deep sedation group (55.2%, P = 0.040). Approximately 50% of patients were admitted with respiratory reasons (56.8%), followed by cardiovascular (23.3%), other (16.6%), and digestive (13.1%) reasons. No differences of reasons for ICU admission were observed between the two groups. The mean APACHE II score was 23.4 (± SD 10.0) in all patients, without differences between the two groups (23.1 ± 9.8 in the light sedation group vs. 23.6 ± 10.1 in the deep sedation group, P = 0.632). The mean RASS score in the light sedation group was −1.1 (± SD 0.7), whereas that in the deep sedation group was −3.4 (± SD 0.8), indicating a more sedated state (P < 0.001). Supplementary Table 2 presents the comparison of the profile of sedative and analgesic agents within the first 48 hours between the two groups. The use of vasopressors was common (77.0%), whereas only one-third of patients received renal replacement therapy (16.9%) or neuromuscular blockade (27.1%). Among the ICU support within the first 48 hours, patients in the deep sedation group were more likely to undergo vasopressor infusions (80.3% vs. 70.4% in the light sedation group, P = 0.004) and neuromuscular blockade (31.5% vs. 18.3% in the light sedation group, P < 0.001).
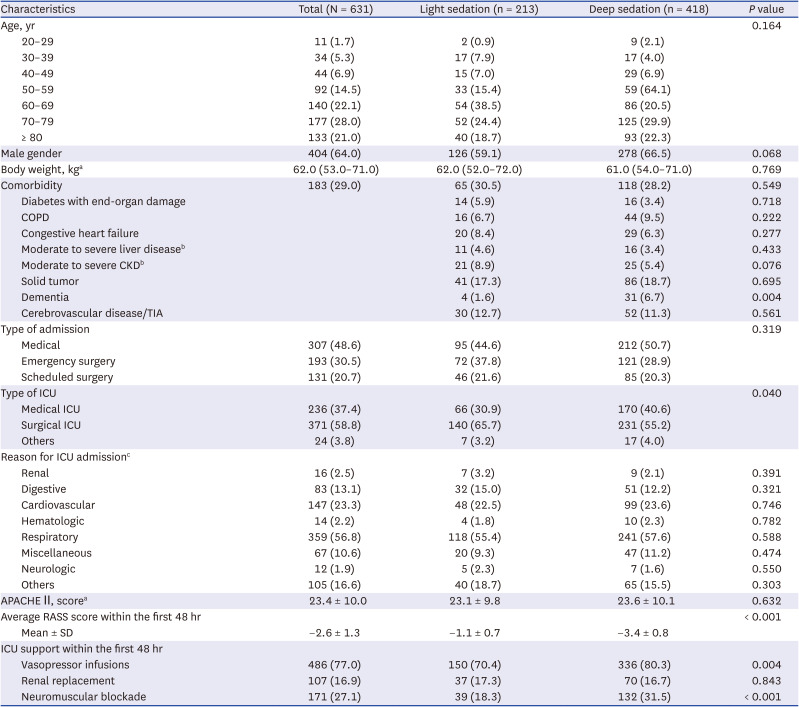
Table 1
Baseline characteristics of patients at ICU admission
Data are reported as mean ± standard deviation or median (interquartile range) for continuous variables and number (percentage) for categorical variables.
ICU = intensive care unit, COPD = chronic obstructive pulmonary disease, CKD = chronic kidney disease, TIA = transient ischemic attack, APACHE II = acute physiology and chronic health evaluation II, RASS = Richmond Agitation–Sedation Scale, SD = standard deviation.
aData on body weight are presented for all 605 patients, excluding 26 with missing data (4 in the light sedation group and 22 in the deep sedation group). Data on APACHE II are presented for all 577 patients, excluding 54 patients with missing data (15 in the light sedation group and 39 in the deep sedation group).
bSevere to moderate liver disease is defined as cirrhosis and portal hypertension with or without variceal bleeding history. Severe to moderate CKD is defined as serum creatinine of > 3 mg/dL or on dialysis or post-kidney transplant status or uremia status.
cOne hundred seventy-two patients had multiple reasons for ICU admission.
![]()
Outcomes
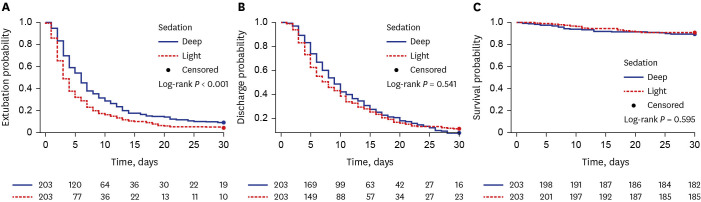
In the entire cohort, in-hospital mortality was observed in 77 patients (12.2%) (Table 2). Mortality rates were 14.1% and 8.4% in the deep and light sedation groups (P = 0.039), respectively. There were no differences on days until death after ICU admission (P = 0.896), ventilator (P = 0.822), or extubation (P = 0.692). The proportion of extubation significantly differs between the two groups (95.3% in the light sedation group vs. 88.0% in the deep sedation group, P = 0.003). Moreover, a longer duration of ventilator support was observed in the deep sedation group (6 days) than in the light sedation group (3 days, P < 0.001). Similar results based on the sedation depth existed for ICU discharge (89.2% in the light sedation group vs. 87.3% in the deep sedation group, P = 0.492) although the median days to ICU discharge were longer in the deep sedation group (10 days) than in the light sedation group (8 days, P = 0.005). The Kaplan-Meier estimates showed that patients who were deeply sedated within the first 48 hours had a significantly longer time to extubation (P < 0.001) (Fig. 1). Furthermore, differences in ICU length of stay (P = 0.005) and death (P = 0.041) were observed between the two groups.
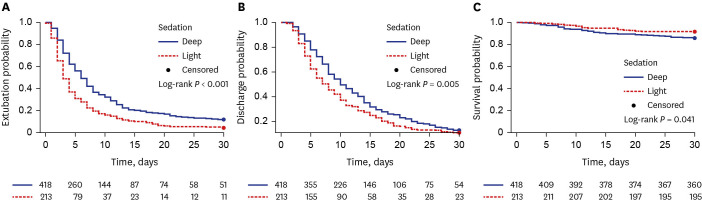
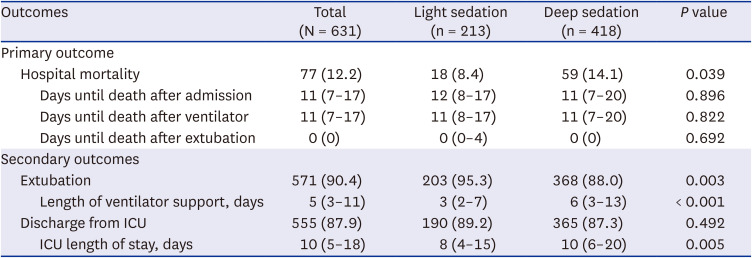
Fig. 1
Kaplan-Meier curves for time to event. Red line, patients with light sedation during first 48 hours from admission; Blue line, patients with deep sedation during first 48 hours from admission. (A) Time to extubation. (B) Time to intensive care unit discharge. (C) In-hospital survival.
![]()
Table 2
Clinical outcomes
Data are reported as median (interquartile range) for continuous variables and number (percentage) for categorical variables.
ICU = intensive care unit.
![]()
After adjusting for confounders comprising age, gender, type of admission, type of ICU, vasopressor infusions, and neuromuscular blockade, multivariable Cox proportional hazard regression analysis demonstrated that deep sedation was independently associated with reduced chances of shorter time to extubation than light sedation (adjusted HR, 0.66; 95% CI, 0.55–0.80; P < 0.001) (Table 3). Conversely, deep sedation was not associated with ICU length of stay (adjusted HR, 0.89; 95% CI, 0.74–1.06; P = 0.213) or in-hospital death (adjusted HR, 1.37; 95% CI, 0.79–2.36; P = 0.252).
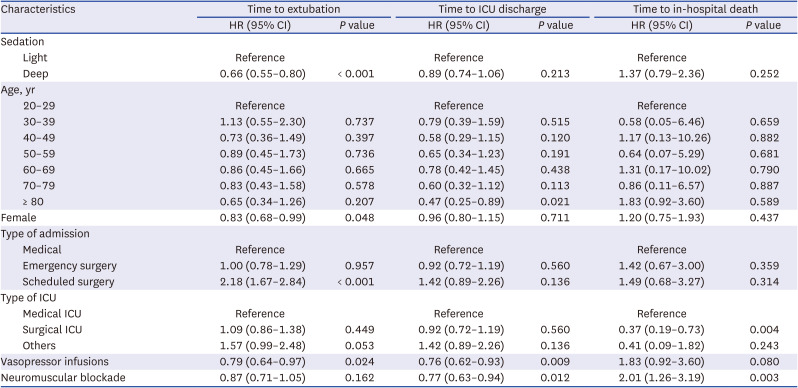
Table 3
Multivariable Cox proportional hazard regression models of time to event
HR > 1 indicates a higher probability of event than reference.
ICU = intensive care unit, HR = hazard ratio, CI = confidence interval.
![]()
Outcomes among propensity-matched patients
After propensity score matching in a 1:1 ratio, 203 matched pairs of patients were identified (Supplementary Table 3). In-hospital mortality was statistically similar between the two groups: 8.9% in the light sedation group (18 of 203 patients) versus 10.3% in the deep sedation group (21 of 203 patients) (Supplementary Table 4). The length of days until death postadmission, ventilator, and extubation did not significantly differ between the two groups. The HR for in-hospital mortality in the light sedation group compared with the deep sedation group was 1.19 (95% CI, 0.65–2.17; P = 0.582) (Fig. 2). No statistically significant difference was observed in ICU discharge between the light (88.6%) and deep sedation groups (92.1%) (HR, 0.94; 95% CI, 0.79–1.13; P = 0.500). The deep sedation group remained significantly associated with a longer time to extubation than the light sedation group (HR, 0.68; 95% CI, 0.56–0.83; P < 0.001).
DISCUSSION
To the best of our knowledge, this is the first Korean study to demonstrate these associations between early deep sedation and clinically important outcomes. A multicenter, prospective cohort study was conducted to assess independent associations between the depth of early sedation after initiating mechanical ventilation and clinical outcomes in the Korean population. Deep sedation was delivered to approximately two-thirds of mechanically ventilated patients within the first 48 hours in Korea. We found that patients in deep sedation have worse outcomes of time to extubation, ICU discharge, and in-hospital mortality than those in light sedation. However, after adjusting for multiple covariates, including age, gender, type of admission, type of ICU, vasopressors, and neuromuscular blockade, early deep sedation was only associated with delayed time to extubation. Similarly, the benefits of time to extubation were observed in the light sedation group of the matched cohort.
Previous studies have shown that the presence of early deep sedation in mechanically ventilated patients substantially increased the probability of worse outcomes, including death. The first prospective multicenter longitudinal study of the clinical practice of early sedation in critically ill patients was conducted by the Sedation Practice in Intensive Care Evaluation (SPICE) study investigators.5 This study included 25 ICUs in Australia and New Zealand and reported that the depth of early sedation independently predicted delayed extubation and increased mortality. These results were replicated in another prospective study in 11 Malaysian ICUs using the SPICE protocol.22 This group also performed multicenter international longitudinal observational studies in 42 ICUs in Australia and New Zealand, Malaysia, and Singapore.6 This study revealed that the escalating sedation intensity during the first 48 hours following mechanical ventilation was associated with increased 180-day mortality and time to extubation. Similar findings are shown in Brazilian ICUs although the study used the Glasgow Coma Scale as the assessment tool for sedation depth.23 Moreover, in a retrospective cohort study of a single center in Germany, early deep sedation in ICU induced decreased 2-year follow-up survival and in-hospital survival.7 Recently, early deep sedation during the first 48 hours of mechanical ventilation and its impact on outcome was demonstrated in a meta-analysis.3 These data suggest that early sedation could be a modifiable treatment variable to improve outcomes.
Our findings are inconsistent with recently published studies in other healthcare systems. Patients enrolled in this study have similar characteristics to those recruited in other studies conducted in Australia and New Zealand with > 20 APACHE II scores and > 70% of vasopressor infusions.5 However, a gap in in-hospital mortality was observed between the two studies (12.2% in our study vs. 21.1% in Australia and New Zealand). Similar differences existed in the Malaysian study (hospital mortality, 31.7%).22 In Brazilian ICUs, mortality in mechanically ventilated patients was 38.8%.23 Furthermore, a nationwide retrospective cohort study that included critically ill patients undergoing mechanical ventilation for > 48 hours in Korean population reported 35.4% of in-hospital mortality.17 Considering these results, patients in this study were probably too good to get any potential benefit in mortality. For example, we excluded patients who were expected to die within 90 days, which might have contributed to lower mortality compared to previous studies. Furthermore, the epidemiologic features of a single nation distinct from other regions might have resulted in a potential risk of biases.
The current guideline published in 2018 suggests using light sedation in critically ill, mechanically ventilated adults.12 Similar to our finding, this guideline evaluated that light sedation was associated with a shorter time to extubation, but not 90-day mortality from several randomized trials.2124252627282930 Nevertheless, previous trials have rather focused mainly on sedation interruption in mechanically ventilated patients.89 However, a systematic review did not find strong evidence that daily sedation interruption alters the duration of mechanical ventilation, length of ICU, and mortality.10 Even a recent randomized, controlled trial comparing a plan of no sedation and a plan of light sedation with daily interruption showed that the plan of no sedation resulted in no important differences in the number of ventilator-free days or length of ICU or hospital stay.11 Results from these studies increase the concern about omitting sedation in mechanically ventilated patients.31 Daily awakening from sedation may require more intensified monitoring and nursing staff and may result in unplanned extubation.3233 A randomized trial comparing no sedation with light sedation showed more events of accidental extubation requiring reintubation within 24 hours in nonsedated patients (8.9% vs. 4.0%) although most participating ICUs in this study had a nurse-to-patient ratio of 1:1.11
Several limitations should be considered in interpreting our results. First, the design of this cohort study limited the establishment of causality. The association of sedation depth with prognosis may be found because deep sedation might have been introduced for serious illness. Considering this aspect, well-designed, randomized, controlled trials will be needed to demonstrate the causality between early deep sedation and worse outcomes. Second, although multivariable analysis adjusted for confounders, the risk of unmeasured variables may be present in this study. A prospective, randomized study to minimize the confounding effects is warranted. Third, in addition to ambiguous exclusion criteria such as patients with a disease that likely leads to death within 90 days, there may be more factors that could contributed to the lower mortality rate than previous studies. Thus, further studies will be needed to monitor long-term mortality in order to minimize the effects of these factors. Fourth, although patients’ delirium was assessed daily based on confusion assessment method for the ICU (CAM-ICU), it was difficult to properly assess patients’ delirium in the deep sedation group due to the nature of CAM-ICU which can only evaluate patients with −3 or higher of RASS value. Finally, our study did not assess the long-term complications, such as posttraumatic stress disorder.
In conclusion, early deep sedation was highly prevalent in mechanically ventilated patients in many Korean ICUs. Early deep sedation was associated with delayed extubation, but not associated with prolonged ICU stay or in-hospital death in the present study.
 XML Download
XML Download