

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary arterial hypertension (PAH) is a disease characterized by elevated pulmonary arterial pressure and pulmonary vascular resistance leading to right ventricular heart failure and death.1)2) Given the rare nature of the disease, it is challenging to understand its true prevalence, incidence, and prognosis.3)
Following an unprecedented economic growth, the national health policies have also advanced for the past 30 years in South Korea. The nature of PAH in South Korea has been unknown until the early 2000s.4) However, the collaborative effort by the Korean government and academic societies has accelerated the adoption of advanced diagnostics and therapeutics for rare diseases, including PAH, in a relatively short period. As such, a comprehensive report on recent progress in diagnosis and management of PAH may be crucial to understand the impact of the advancing healthcare infrastructure on real-world clinical practice of PAH.
Herein, using a nationwide health claims database, we delineated temporal trends in the prevalence, incidence, medication prescription pattern, and 5-year survival of PAH in Korea. We also assessed cumulative survival and potential predictors of mortality among incident PAH patients.
METHODS
Ethical statement
The study complies with the ISHLT Ethics statement and was approved by the Institutional Review Board of Severance Hospital, Seoul, Korea (#4-2020-0207). Written informed consent was waived, as this is a retrospective study of de-identified administrative data.
Data source
We used a nationwide database provided by the National Health Insurance Service (NHIS), which is the single provider of universal healthcare coverage in South Korea. The NHIS database contains sociodemographic details, medical reimbursement claims records with the International Classification of Diseases (ICD), 10th revision (ICD-10) coding, and death information of the entire South Korean population.5)6)
Definition of pulmonary arterial hypertension
We designed a 3-component algorithm for defining PAH to overcome the current challenges in analyzing administrative health data for PAH—ICD-10 codes do not reflect the current World Health Organization (WHO) pulmonary hypertension (PH) classifications properly. For example, many Korean Eisenmenger-related PAH patients with Eisenmenger-related PAH are usually given ICD-10 codes for both secondary PH (I27.2 or I27.8) and Eisenmenger syndrome (Q21.8). However, the WHO PH classification states that patients with PAH related to congenital heart diseases (PAH-CHD) be classified as group I PH (ICD-10; I27.0). We therefore devised an algorithm to include ICD-10 codes for primary PH (I27.0), secondary PH (I27.2 and I27.8), and Eisenmenger syndrome (Q21.8) to minimize the chance of leaving out true subjects with PAH.
We added two additional components to our algorithm for defining PAH; those who had been prescribed PAH-specific drug and had undergone right heart catheterization (RHC) at least once were defined as having PAH (Supplementary Table 1). The PAH-specific drug class included endothelin receptor antagonist (ERA), phosphodiesterase-5 inhibitor (PDE5i), and prostacyclin analogue (PCA). Soluble guanylate cyclase stimulator and epoprostenol were excluded since they were not available in Korea at the time of the study.1) PDE5is generally prescribed for erectile dysfunction and calcium channel blockers were considered non-specific for PAH and were thus excluded as well.
Study population
For repeated cross-sectional analysis of the PAH prevalence and PAH-specific drug prescription in Korea, we identified all patients with PAH aged ≥20 years who had been prescribed PAH-specific drug in each year between 2002 and 2018. For longitudinal analysis of the long-term survival of PAH, we excluded the first 2 years of the database (i.e., 2002–2003), during which the date of PAH diagnosis could not be accurately ascertained, and identified 2,799 patients newly diagnosed with PAH between 2004 and 2018. After excluding 648 who had been diagnosed before the age of 20, a final study sample of 2,151 incident PAH cases remained.
Key variables and outcomes
We extracted data on demographics, class and regimen of PAH-specific drug, and the presence of comorbidities, including hypertension,7) diabetes,8) dyslipidemia,9) coronary artery disease, chronic obstructive pulmonary disease, chronic kidney disease, cancer, and human immunodeficiency virus infection. Detailed definitions and codes for comorbidities are presented in Supplementary Table 1. Prevalence of PAH was defined as the number of patients with PAH per million people. Incidence of PAH was defined as the number of patients newly diagnosed with PAH per million person-years. We defined the date of PAH diagnosis as the date of the first prescription of PAH-specific drug. PAH-specific drug regimen (i.e., mono-, dual-, or triple therapy) was determined based on the maximal number of PAH-specific drug classes prescribed during the follow-up. All comorbidities were determined from claims data during a look-back period of 2 years prior to the date of PAH diagnosis.
The primary outcome of the longitudinal analysis was all-cause mortality. Vital status was ascertained by linkage to the national mortality data via resident registration numbers. Participants in the longitudinal analysis were followed up from the date of PAH diagnosis until the occurrence of the primary outcome event or December 31, 2018, whichever came earliest.
External validation of the 3-component algorithm
We validated our 3-component algorithm in a separate validation cohort. The validation cohort consisted of all patients who visited the Pulmonary Hypertension clinic at Gachon University Gil Medical Center for suspected PAH. Two independent cardiologists reviewed medical records, including physician chart, echocardiography and RHC data, and medication prescription records, to adjudicate PAH diagnosis. The sensitivity, specificity, positive predictive value, and negative predictive value of the algorithm were calculated.
Statistical analysis
Baseline characteristics were presented as median [interquartile range] or number (%). Intergroup comparisons were made using Wilcoxon rank-sum test or χ2 test. The cumulative survival of the incident PAH patients was estimated using the Kaplan-Meier method. We used Cox proportional hazard regression models to identify potential predictors of mortality. The proportional hazard assumption was tested by visual assessment of log-minus-log plots and Schoenfeld residuals. Because PAH-specific drug regimen violated the assumption, it was not included in the first multivariable model (Model 1). The second model was stratified by PAH-specific drug regimen to additionally adjust for it without violating the assumption (Model 2). The final model included PAH-specific drug regimen along with other variables (Model 3). Analyses were carried out using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Annual trends in pulmonary arterial hypertension prevalence/medication
The overall prevalence of PAH per million people has risen from 0.4 in 2002 to 29.9 in 2018(75-fold increase; Figure 1A and Supplementary Table 2). The prevalence was consistently higher in women than in men (Supplementary Table 2, Supplementary Figure 1A). The prevalence has steadily increased in all age groups (i.e., 20–39, 40–64, and ≥65 years), but more rapidly in older age groups (i.e., 40–64 and ≥65 years) after the late 2000’s (Supplementary Figure 1B). The number of individuals with PAH who died from any cause has also gradually increased regardless of sex, age, or etiology of PAH (Supplementary Table 3).

Figure 1
Annual trends in prevalence, incidence, and medication prescription pattern of pulmonary arterial hypertension in Korea. (A) Prevalence and incidence of PAH. (B) medication prescription pattern of PAH in Korea, 2002-2018. In 2018, the number (proportion) of patients on monotherapy, dual therapy, and triple therapy were 895 (71.0%), 309 (24.5%), and 57 (4.5%), respectively (pie chart).
PAH = pulmonary arterial hypertension.
![]()
PCA was first authorized for use in Korea in 1997 (beraprost; Supplementary Figure 2). The first ERA, bosentan, was approved in 2006, followed by ambrisentan in 2011 and macitentan in 2016. ERA has been the most frequently prescribed drug class since 2008, with a higher-than-75% prescription rate after 2011 (Supplementary Figure 2). PDE5i was the second most frequently prescribed drug class in 2018 (38%) (Supplementary Table 4, Supplementary Figure 2).
In terms of drug regimens, monotherapy had been predominant in the early-mid 2000s, when PCA was the only available PAH-specific drug class in Korea (Figure 1B, Supplementary Table 4). In 2018, 71% of the patients were given monotherapy, about 70% of whom were on ERA. Dual therapy first emerged in 2007, in accordance with the approval of bosentan, and has steadily increased up to 24.5% in 2018. Triple therapy was first observed in 2014, 1 year after the approval of PDE5i. Although the number of patients on triple therapy has also continuously grown, it still held a minor proportion in 2018 (4.5%; Figure 1B, Supplementary Table 4). Overall, the proportion of combination therapy was increased by 2.6-fold in 2018 (29%) compared to 2007 (11.3%).
Annual trends in pulmonary arterial hypertension incidence
The incidence of PAH has increased over time regardless of sex or age (Figure 1A,Figure 2A, B, and Table 1). The overall incidence (per million person-years) increased by 12-fold between 2004 (0.5) and 2018 (6.3). The female to male ratio ranged from 1.6 to 3.1. The incidence of idiopathic PAH (IPAH) has rapidly increased, while those of PAH related to connective tissue disease (PAH-CTD) and PAH-CHD have been stagnant (Figure 2C, Table 1).
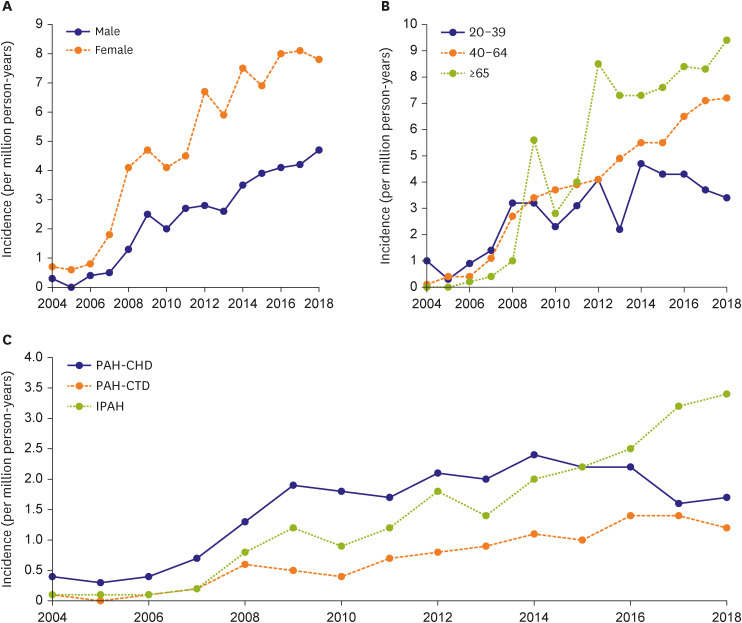
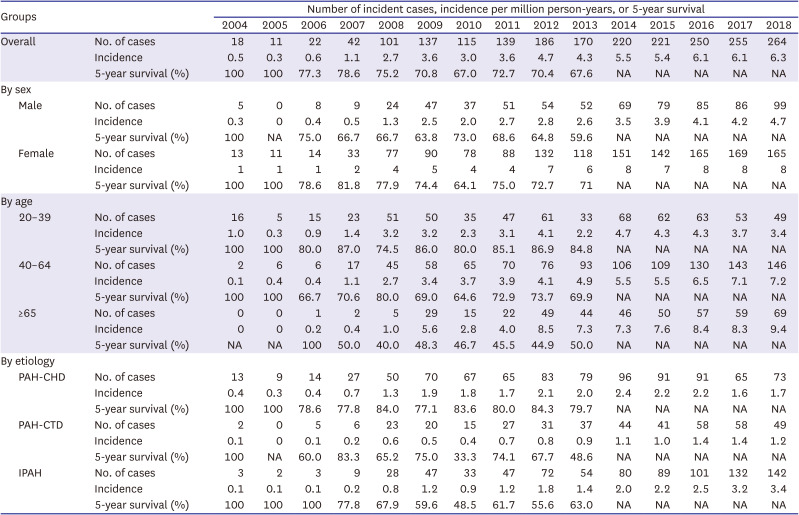
Figure 2
Annual trends in incidence of pulmonary arterial hypertension in Korea, 2002–2018. (A) sex-specific, (B) age-specific, and (C) etiology-specific incidence of pulmonary arterial hypertension in Korea.
IPAH = idiopathic pulmonary arterial hypertension; PAH-CHD = pulmonary arterial hypertension related to congenital heart diseases; PAH-CTD = pulmonary arterial hypertension related to connective tissue disease.
![]()
Table 1
Annual trends in incidence and 5-year survival of pulmonary arterial hypertension in Korea, 2004–2018
Incidence was calculated as the number of incident cases per million Korean adults per year. 5-year survival was calculated as the proportion of incident cases who had been alive for 5 years after the diagnosis of pulmonary arterial hypertension.
IPAH = idiopathic pulmonary arterial hypertension; PAH-CHD = pulmonary arterial hypertension related to congenital heart disease; PAH-CTD = pulmonary arterial hypertension related to connective tissue disease.
![]()
Baseline characteristics of longitudinal cohort
Of the 2,151 incident PAH cases (median [interquartile range] age, 50 [37–62] years; 67.2% female) (Figure 3), 1,614 (75.0%), 467 (21.7%), and 70 (3.3%) were on mono-, dual, and triple therapy, respectively. Sixty nine percent of the patients were taking ERA, 31% were taking PDE5i, and 28% were taking PCA. Prevalence of hypertension and diabetes were 74.2% and 18.5%, respectively. There were no patients with human immunodeficiency virus infection (Table 2).

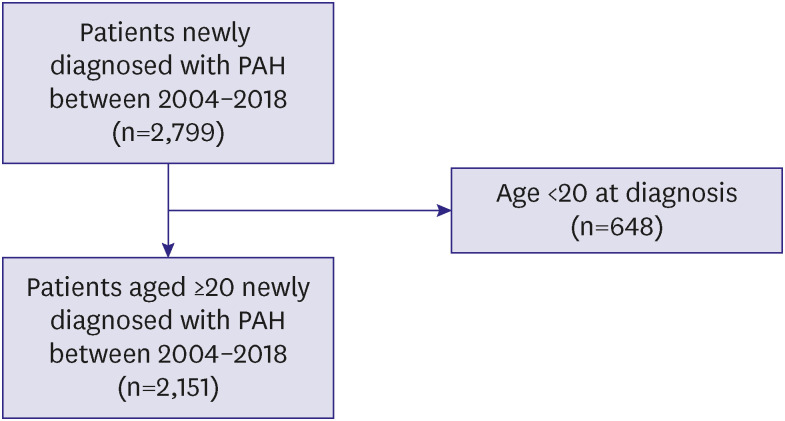
Table 2
Baseline characteristics of incident pulmonary arterial hypertension cases
Values as median [interquartile range] or number (%).
COPD = chronic obstructive pulmonary disease; ERA = endothelin receptor antagonist; HIV = human immunodeficiency virus; IPAH = idiopathic pulmonary arterial hypertension; PAH = pulmonary arterial hypertension; PAH-CHD = pulmonary arterial hypertension related to congenital heart disease; PAH-CTD = pulmonary arterial hypertension related to connective tissue disease; PCA = prostacyclin analogue; PDE5i = phosphodiesterase-5 inhibitor.
*Categorized based on quartiles among the entire Korean population.
†Counted with duplicates for combination therapy.
![]()
The number (proportion) of patients classified as PAH-CHD, PAH-CTD, and IPAH were 893 (41.5%), 416 (19.3%), and 842 (39.1%), respectively (Table 2). The median age was the highest in the IPAH group (56 years). Female sex was more common than male sex in all etiology groups, the proportion of which was the highest in the PAH-CTD group (86.5%). Patients with IPAH had higher household income than those with other PAH subtypes. The use of combination (dual or triple) therapy was more frequent in the PAH-CHD and PAH-CTD groups than in the IPAH group. Patients with IPAH exhibited higher prevalence of comorbidities than those with other subtypes, probably due to their older age (Table 2).
Survival and predictors of mortality
The 5-year survival of incident PAH patients ranged from 67.0% to 78.6%, except in 2004 and 2005 (Table 1). During a maximum of 14.9 years of follow-up, the median survival of the overall incident PAH patients was 13.1 years (Figure 4A and Supplementary Table 5). Patients with PAH-CHD exhibited higher cumulative survival than those with other PAH subtypes (Figure 4B). The survival rate did not differ significantly between those on mono-, dual, and triple therapy (all pairwise log-rank p>0.05;Figure 4C). Patients with a history of cancer showed worse prognosis than those without (Figure 4D). The survival of patients stratified by year of PAH diagnosis are presented in Supplementary Figure 3.
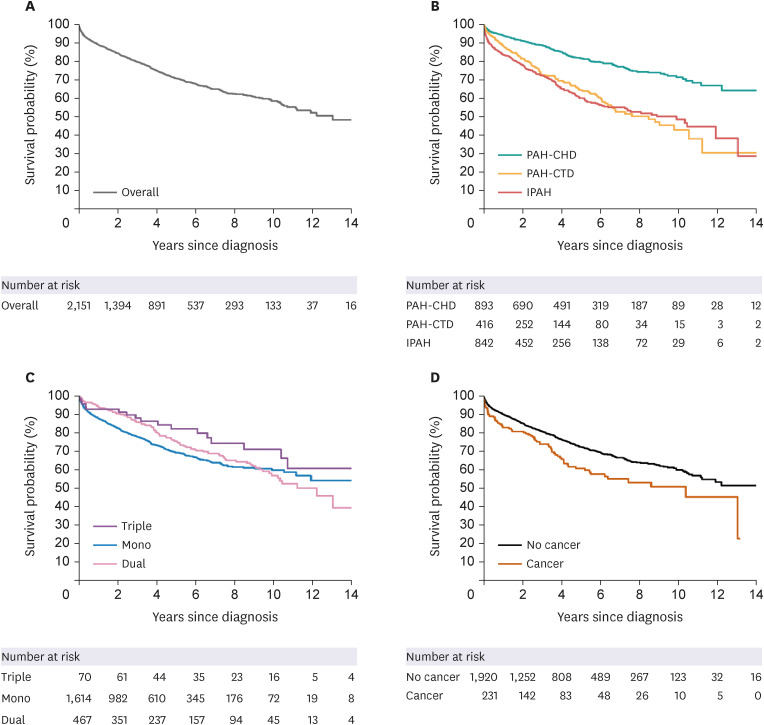
Figure 4
Kaplan-Meier survival curves of patients with incident pulmonary arterial hypertension. Cumulative survival of (A) overall incident PAH cases and that of patients stratified by (B) etiology of PAH, (C) PAH-specific drug regimen, and (D) cancer history. IPAH = idiopathic pulmonary arterial hypertension; PAH = pulmonary arterial hypertension; PAH-CHD = pulmonary arterial hypertension related to congenital heart disease; PAH-CTD = pulmonary arterial hypertension related to connective tissue disease.
![]()
In a univariable Cox regression model, older age, highest household income quartile, IPAH or PAH-CTD etiology (as compared with PAH-CHD), and the presence of comorbidities were associated with an increased risk of mortality. On the contrary, female sex and the use of combination therapy were predictors of favorable prognosis (Table 3). After multivariable adjustment, older age, IPAH or PAH-CTD etiology (as compared with PAH-CHD), diabetes, dyslipidemia, and chronic kidney disease remained as predictors of higher mortality. Female sex was the only remaining predictor of favorable prognosis. The use of combination therapy and history of cancer were no longer independent predictors of mortality after multivariable adjustment (Models 1-3; Table 3).
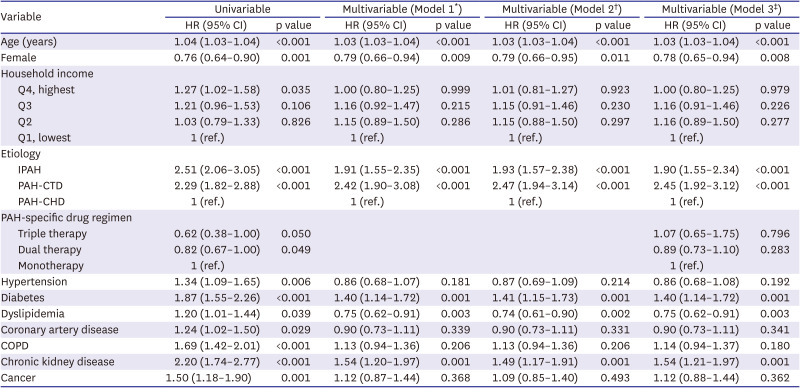
Table 3
Predictors of mortality in patients with pulmonary arterial hypertension
CI = confidence interval; COPD = chronic obstructive pulmonary disease; HR = hazard ratio; IPAH = idiopathic pulmonary arterial hypertension; PAH-CHD = pulmonary arterial hypertension related to congenital heart disease; PAH-CTD = pulmonary arterial hypertension related to connective tissue disease.
*Model 1 was not adjusted nor stratified for PAH-specific drug regimen; †Model 2 was stratified by PAH-specific drug regimen; ‡Model 3 was additionally adjusted for PAH-specific drug regimen.
![]()
Validation of the 3-component algorithm
Of the 248 participants in the validation cohort (median [interquartile range] age, 59 [46–70] years; 64.9% female), 113 (45.6%) were adjudicated as having PAH. The number (proportion) of participants classified as having PAH according to the 3-component algorithm was 94 (37.9%). The sensitivity, specificity, positive predictive value, and negative predictive value of the algorithm were 81.4%, 98.5%, 97.9%, and 86.4%, respectively (Supplementary Table 6).
DISCUSSION
The present study demonstrated that the prevalence and incidence of PAH have constantly risen in Korea. The 5-year survival of incident PAH patients was 71.8%. Although less than 30% of the patients received combination therapy in 2018, this proportion will likely continue to grow in the future, as governmental restrictions on upfront combination therapy have been lifted in Korea since 2019. In our analysis, patients on combination therapy showed comparable outcomes with those on monotherapy despite the probability that patients on multiple drug classes may have higher disease severity than those on monotherapy. PAH-CHD was significantly associated with a lower risk of mortality than IPAH or PAH-CTD, and there was a signal of better prognosis among patients with IPAH than those with PAH-CTD, findings generally consistent with those of previous studies.10)
The observed rapid increase in the prevalence and incidence of PAH in Korea is unprecedented when compared to other countries in which the increase was less than 2-fold11) or hospitalizations were paradoxically reduced by 58% during a similar period.12) Such findings might be a result of the collaborative effort led by the Korean government and academic communities to advance healthcare policies and academic platforms for rare diseases in Korea.13) The establishment of the KORPAH (Korean Registry of Pulmonary Arterial Hypertension) was the first initiative to bring PAH to center stage, encouraging physicians to be more aware of the disease. Such movement was succeeded by the foundation of the Korean Pulmonary Hypertension Society, which provided a platform for more efficient collaboration between researchers and physicians. The Korean government and Korean Pulmonary Hypertension Society also jointly hosted public campaigns to promote the importance of early detection and treatment of PAH to physicians and patients. These comprehensive movements may have altogether contributed to an unprecedented increase in detection, and thereby in prevalence and incidence, of PAH in Korea.
The Korean government currently reimburses 90% of the medical costs for patients with PAH, which allows physicians to prescribe any type of PAH-specific drug that best suits the patient regardless of its cost. This may explain, at least in part, an interesting finding that ERAs are the most prescribed PAH-specific drugs in Korea despite being approximately 4 times more expensive than PDE5is. Contrariwise, US pharmacy claims data showed that PDE5i has consistently been the most commonly prescribed drug class, followed by ERA and PCA.14)
Previous reports on the survival rate of PAH in Korea have varied. In KORPAH, the first Korean nationwide prospective registry of PAH, the 3-year survival rate was 84.4%.15) Since the majority (60.2%) of patients were diagnosed with PAH via echocardiography, it is suspected that many patients might have been false-positives, which could have led to the underestimation of mortality.16) In a previous analysis of the Korean Health Insurance Review and Assessment Service (HIRA) database, the 5-year survival rate was 46%.17) Given that the HIRA database only includes information on in-hospital death5) and patients without any health claim for over 1 year were considered deceased in the above study,17) the mortality could have probably been overestimated. On the contrary, all vital statuses were ascertained by linkage to the national mortality data in the present study, ensuring the accuracy of death information.
In the 1980s, the 5-year survival of PAH was approximately 30%, with a median survival duration of less than 3 years.18) The REVEAL (Registry to Evaluate Early and Long-term Pulmonary Arterial Hypertension Disease Management) registry from the US showed improved prognosis in the 2000s, with the 5-year survival rate of 61–65%.19) The most recent European COMPERA (Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension) registry reported the 5-year survival rate of 71%.20) The findings were generally consistent in East Asian reports—71.8% in Korea (current study), 20–73% in China,21)22) 74% in Japan,23) and 78% in Taiwan24)—suggesting that the prognosis of PAH in East Asian countries is now comparable to that in western countries.
Current international guidelines for PAH recommend an upfront combination therapy for high-risk patients.1)25)26) Although the upfront use of multiple PAH-specific drug classes is currently not covered by the Korean national health insurance, the rapid escalation to combination therapy within one month in poor responders to monotherapy has been approved since 2019. Accordingly, the proportion of combination therapy use was relatively low in our report, which was based on health claims data before 2019. The observed nonsignificant differences in cumulative survival between those on mono, dual, and triple therapy, in addition, may not reflect the true effects of combination therapy due to the observational nature of the study. Our findings, however, suggest that patients on combination therapy may have a comparable prognosis with those on monotherapy despite having higher illness severity.
Although the survival rate of PAH has dramatically improved over recent years, it remains unsatisfactory. Improving adherence to guideline-directed medical therapy—including but not limited to early combination therapy—and developing novel diagnostics and therapeutics for precision medicine may help further improve the prognosis of PAH.1) Our group has recently delineated the prevalence and clinical features of bone morphogenetic protein receptor type 2 mutation in Korean IPAH patients.27) Moreover, novel genetic variants in Korean PAH patients are currently being investigated through deep phenotyping in a nationwide platform.28) Such efforts are expected to lay the groundwork for personalizing diagnosis and management of PAH in Korea.
To our knowledge, this is the first non-US study using a 3-component algorithm to define PAH in a nationwide administrative health claims database.29) Most previous analyses of nationwide claims data implemented 1- or 2-component diagnostic algorithms (e.g., ICD code only, ICD code plus PAH-specific drug prescription or diagnostic procedure code), the accuracies of which were lower than that of our 3-component algorithm.3)30)
This study has several limitations. First, the diagnoses of PAH were neither confirmed by attending physicians nor centrally adjudicated, the problem intrinsic to the analysis of administrative health claims database. In addition, there may have been some false-negative PAHs, including those who had not been prescribed PAH-specific drug at any time during follow-up. However, our newly developed 3-component diagnostic algorithm for PAH exhibited high accuracy in our validation cohort. Second, because we defined the date of PAH diagnosis as the date of the first prescription of PAH-specific drug, patients with severe PAH who had not survived until their first drug prescription were excluded from the analysis. This survivorship bias may explain in part the higher survival rate observed among the participants diagnosed in the earlier period of the database (i.e., 2004–2007). Third, because of the retrospective, non-randomized nature of the study, the possibility of residual confounding and bias cannot be ruled out in our association analyses. In particular, the lack of an association between the number of PAH-specific drug classes and mortality may have been affected by the difference in the severity of PAH among the groups and the time-varying nature of PAH-specific drug prescription, both of which could not be adequately addressed in our analysis. Fourth, external validation of our 3-component algorithm was conducted only in a single center cohort, and we could not validate our definition of PAH etiology. Fifth, we could not age-standardize our incidence and prevalence estimates because the counts by age group were too small to be standardized. Lastly, our results were derived from the Korean population and should be interpreted with caution when applied to other populations.
In conclusion, the prevalence and incidence of PAH and use of combination therapy have steadily increased in Korea since the early 2000s. The 5-year survival rate of PAH in Korea was comparable to those in western countries. Age, sex, etiology of PAH, diabetes, dyslipidemia, and chronic kidney disease were independent predictors of mortality. It appears that the collaborative effort by the Korean government and academic societies aimed at improving healthcare infrastructure for PAH led to an increase in the detection of PAH and use of guideline-directed combination therapy in Korea.
 XML Download
XML Download