

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) is a global health issues and is closely related to significant morbidity and mortality.1)2) In particular, HF is one of the main causes of hospitalization and death in the elderly population, and the prevalence of the elderly over 80 years old is much higher than that of the general population.2)3) The prevalence is estimated to increase further as the aging society progresses. In the past decades, clinical tools for diagnosing HF, such as genetic testing and cardiac magnetic resonance imaging, have been developed, and treatments option have also continued to be developed.4) The American College of Cardiology (ACC)/American Heart Association (AHA), European Society of Cardiology (ESC) and Korean HF guidelines have developed evidence-based treatment for HF to help physicians to manage appropriately to improve clinical outcomes which reduced mortality and hospitalization.5)6)7) A recent guideline emphasizes combination therapy of 4 main drugs, including renin-angiotensin system (RAS) blockers (angiotensin converting enzyme inhibitors [ACEIs], angiotensin receptor blockers [ARBs], and angiotensin receptor/neprilysin inhibitors [ARNIs]), beta-blockers [BBs], mineralocorticoid antagonist [MRA], and sodium-glucose cotransporter-2 [SGLT2] inhibitors for the treatment of patients with heart failure with reduced ejection fraction (HFrEF). The guideline also considers up-titration to evidence-based target doses as optimal guideline-directed medical therapy (GDMT).5)6) However, despite the evidences, mortality and hospitalization rates for HF remain steady, early mortality after discharge from HF admission continues to be high, and the GDMT rate is still low.8)9)10)11) These findings suggest that there is a gap between guidelines and clinical practice and highlight the importance of quality assessment of HF care. Therefore, it is necessary to find ways to apply evidence-based management for HF treatment more easily and efficiently.
This review article aims to investigate HF treatment patterns and treatment adherence in the real-world practice, identify clinical gaps in practice, propose ways to improve quality of care for HF, and finally improve care and clinical outcomes for patients with HF.
Go to : 
HEART FAILURE TREATMENT PATTERNS AND TREATMENT ADHERENCE IN HEART FAILURE WITH REDUCED EJECTION FRACTION
A recently published systemic review and meta-analysis of 75 trials for medical therapy in patients with HFrEF demonstrated that a combination of medications, especially ARNI, BB, MRA, and SGLT2 inhibitor had the greatest benefit for reducing a composite outcome of cardiovascular death or first hospitalization for HF (hazard ratio [HR], 0.36; 95% confidence interval [CI], 0.29–0.46).12) The benefits of performing GDMT to improve clinical outcomes in patients with HF are clear.13) However, the administration or up-titration of GDMT in real-world practice remains low. Figure 1 summarizes several registries showing GDMT compliance rates in real-world practice.2)8)14)15)16)17)18)19)20)21)22)23)24)25)26)27)28) The prescription rate is different for each registry, and the prescription rate of ACEI/ARB or BB is over 80% in some registry data; however, the actual GDMT prescription rate is generally low. Even in the most recent data, there was no significant difference in GDMT rates compared to with those of Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) trial published in 2007. A retrospective observational study showed similar results that outpatient use of GDMT remained low at 54% in the year after hospital discharge.10) Novel GDMTs such as ARNI or SGLT2 inhibitor have been recommended as essential drugs for patients with HFrEF in recent guidelines. There is little real-world data on ARNI and SGLT2 inhibitor adherence. A recent analysis of 266,589 patients with recent hospitalization for HF in Japan, Sweden, and the US showed that approximately 10% of patients received ARNI or SGLT2 inhibitor, and these drugs tended to be administered later than other conventional GDMTs such as ACEI/ARB, BB, or MRA.8) Recently, the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF), the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and Reduced Ejection Fraction (EMPEROR-Reduced), the Global Approach to Lowering Adverse Cardiac Outcomes through Improving Contractility in Heart Failure (GALACTIC-HF), and the Vericiguat Global Study in Subjects with Heart Failure with Reduced Ejection Fraction (VICTORIA) trials, which are landmark randomized controlled trials in the field of HF, showed that the ARNI administration rate was less than 20% and only about 2.7% of patients took SGLT2 inhibitors together in the GALACTIC-HF trial.29)30)31)32)33) While the proportions of BB were all above 90%, most MRA prescription rates were only about 70% (Figure 2). Although recent guidelines recommend ARNI or SGLT2 inhibitor as first-line drugs, they are not widely used, and data on actual adherence are still sparse. Additional data are required in the future.
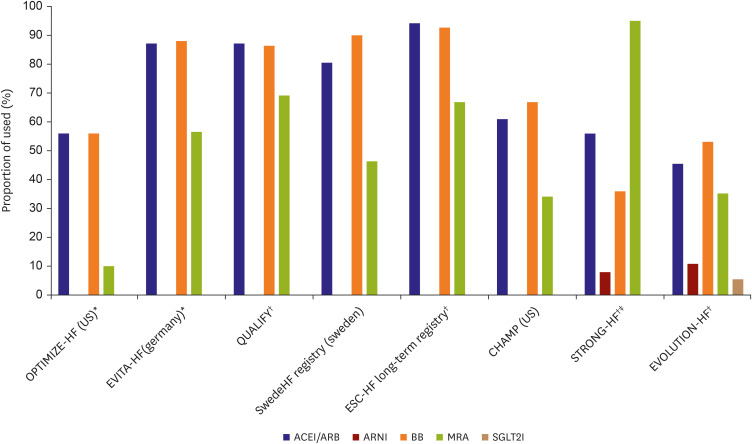 | Figure 1Guideline-directed medical therapy adherence in real-world practice.ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor/neprilysin inhibitor; BB = beta-blocker; CHAMP = Change the Management of Patients; ESC = European Society of Cardiology; EVITA-HF = Evidence Based Treatment - Heart Failure; EVOLUTION-HF = Utilization of Dapagliflozin and Other Guideline Directed Medical Therapies in Heart Failure Patients; HF = heart failure; MRA = mineralocorticoid antagonist; OPTIMIZE-HF = Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure; SGLT2I = sodium-glucose cotransporter-2 inhibitor; STRONG-HF = Safety, Tolerability and Efficacy of Rapid Optimization, Helped by NT-proBNP Testing, of Heart Failure Therapies; QUALIFY = Quality of Adherence to guideline recommendations for LIFe-saving treatment in heart failure surveY.
*In-patients trial; †Multinational study; ‡Prospective randomized trial.
|
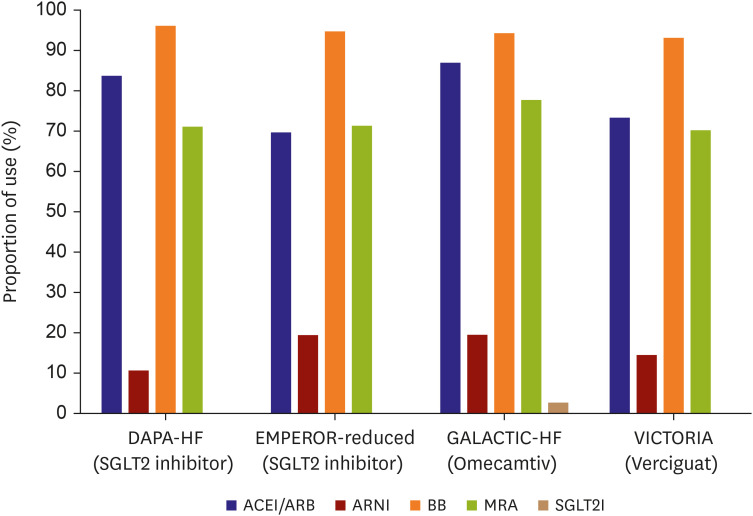 | Figure 2Guideline-directed medical therapy adherence in landmark randomized controlled trial.ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor/neprilysin inhibitor; BB = beta-blocker; DAPA-HF = Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure; EMPEROR-Reduced = Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and Reduced Ejection Fraction; GALACTIC-HF = Global Approach to Lowering Adverse Cardiac Outcomes through Improving Contractility in Heart Failure; MRA = mineralocorticoid antagonist; SGLT2I = sodium-glucose cotransporter-2 inhibitor; VICTORIA = Vericiguat Global Study in Subjects with Heart Failure with Reduced Ejection Fraction.
|
Low prescription rates as well as insufficient dosage are also a problem (Figure 3). When high-dose ACEI or ARB treatment was compared with low-dose ACEI or ARB treatment, all-cause mortality and HF hospitalization rates were lower in the high-dose treatment group.34)35) BB showed a dose-related improvement in left ventricular ejection fraction and a dose-related reduction in all-cause mortality and hospitalization rates.36)37) The Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (Paradigm-HF) trial showed that dose reduction of both sacubitril/valsartan and enalapril was associated with a higher risk of a primary outcome (HR, 2.5; 95% CI, 2.2–2.7). It is more beneficial to administer a dose that is close to the target dose than a low dose to reduce the risk. The Change the Management of Patients with Heart Failure (CHAMP-HF), a prospective observational registry conducted from 150 sites in the US showed that only 1% of patients were receiving maximal target doses of 3 medications (ACEI/ARB/ARNI: 31%, BB: 28%, and MRA: 77%).19) In the Safety, Tolerability and Efficacy of Rapid Optimization, Helped by NT-proBNP Testing, of Heart Failure Therapies (STRONG-HF), a prospective randomized trial, which aimed to prove the efficacy and safety of early GDMT up-titration in patients with acute HF, few patients attained the target dose of ACEI/ARB/ARNI (2%), BB (4%), and MRA (46%) 3 months after discharge in the usual care group. The only increase of target dose administration was seen in MRA 180 days after discharge (60%), although a few patients received the optimal dose.24) In the most recent study, the Utilization of Dapagliflozin and Other Guideline Directed Medical Therapies in Heart Failure Patients (EVOLUTION-HF) trial, a prospective observational trial for 3 nations (Japan, Sweden, and the US), nearly 80% of patients were taking GDMT within 100 days of discharge from HF admission; however, after 1 year, the discontinuation rates of ACEI/ARB, BB, MRA, and ARNI were high, and target dose achievement rates were low in all 3 participating countries.8)
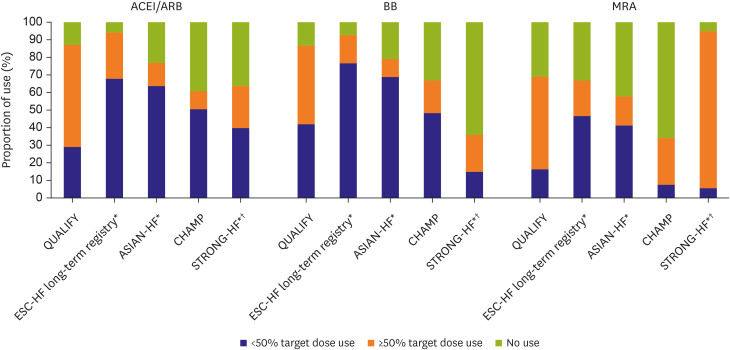 | Figure 3Guideline-directed medical therapy prescription rates according to target dose.ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; BB = beta-blocker; CHAMP = Change the Management of Patients; ESC = European Society of Cardiology; HF = heart failure; MRA = mineralocorticoid receptor antagonist; STRONG-HF = Safety, Tolerability and Efficacy of Rapid Optimization, Helped by NT-proBNP Testing, of Heart Failure Therapies; QUALIFY = Quality of Adherence to guideline recommendations for LIFe-saving treatment in heart failure surveY.
*Multinational study; †Prospective randomized trial.
|
Compared to Western countries, Asian countries tend to have a relatively low prescription rate.38) The Acute Decompensated Heart Failure Syndromes registry for patients with HF hospitalization in Japan showed that the prescription rate increased more at discharge than before admission, but only 76.6% of patients received ACEI/ARB and 67.4% of patients received BB.26) Another registry in Japan, the Japanese Registry Of Acute Decompensated Heart Failure (JROADHF), also showed low prescription rates of ACEI/ARB (46.2%), BB (36.3%), and MRA (21.6%).27) Taiwan had a particularly low prescription rate. According to the Taiwan Society of Cardiology-Heart Failure with reduced Ejection Fraction (TSOC-HFrEF) registry, both ACEI/ARB and BB prescription rates were low compared to those in the US and Europe, and BB prescription rate was particularly low (8–27%). Although the prescription rate of MRA was 49%, which was relatively high compared to Western countries, this is still considered low overall.22) A HF registry of China showed that the overall use of ACEI/ARB, BB, and MRA at discharge was 37.5%, 70.0%, and 74.1%, respectively.28) In Korea, a nationwide observational study using the National Health Insurance Service Database reported that 28.6% of elderly HF patients were not receiving GDMT.39) The Korean Heart Failure (KorHF) registry, a multicenter cohort study of HF in Korea, that was published in 2013, showed that the prescription of ACEI/ARB was 53.7%, BB was 58.6%, and MRA was 53.1%.2) Another study showed that the rates of GDMT prescription of ACEI/ARB (89.7%), BB (69.2%), and MRA (65.9%).40) According to the Korean Acute Heart Failure registry, which was conducted 5 years after of the KorHF trial, the prescription rates were 68.8%, 52.2%, and 46.6%, respectively, which are still relatively low rates.2)
In some patients, increasing the target dose is not possible for several reasons, including adverse effects. However, it should be noted that in landmark clinical trials of HFrEF medications, approximately 30–50% of patients achieved the significant improvements despite not reaching the target dose. Importantly, even the low doses of medication can have significant effects.41)42)43) Therefore, the first consideration is to start the required drug at a low dose at an early time point and, if possible, increase the dose to the target dose according to the patient’s tolerance.41)
Go to :
CAUSES FOR THE GAP BETWEEN GUIDELINES AND REAL-WORLD PRACTICE
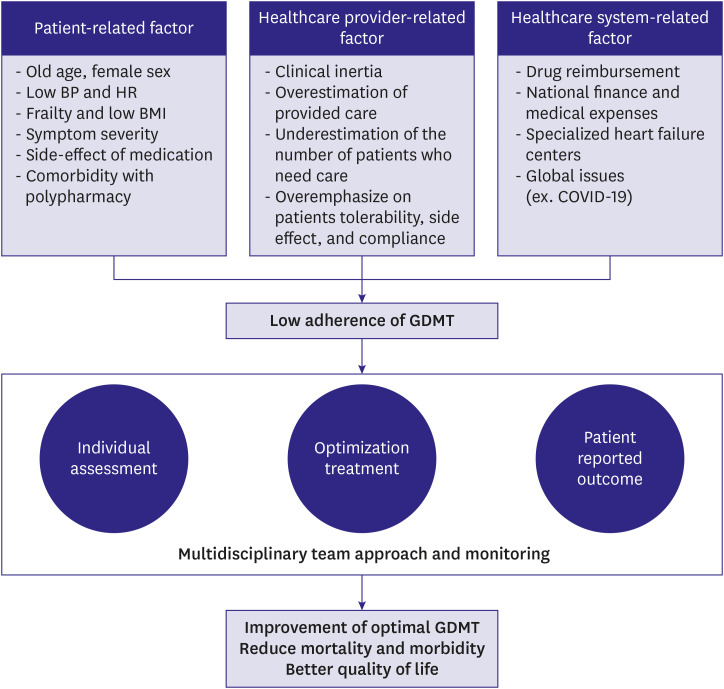
There are several reasons for the low adherence rate of GDMT, including patient-related, healthcare provider-related, and health system-related factors.
Patient related-factors
The most important factors involved in the low adherence rate of GDMT are patient-related factors. Patient characteristics such as sex, age, blood pressure, heart rate, body mass index and HF severity were consistently associated with a low prescription or failure to up-titration of GDMT. In addition, some clinical factors including patients’ comorbidities and polypharmacy also affect adherence of GDMT. Since there are slight differences depending on the drugs, there may be contraindications and various side effects which causes hesitancy in drug prescription. Low blood pressure, renal insufficiency, and old age were the main reasons for the low medication use in the CHAMP-HF trial.19) In particular, hypotension, hyperkalemia, and renal insufficiency were the main reasons for the impeded use of RAS blockers or MRA, and pulmonary disease, hypotension, and bradycardia were associated with low adherence of BB.14) Sex and race also affect the low usage of medication. In the EVOLUTION-HF trial, just 20% of Japanese were taking the target dose of ARNI, compared to more than 40% in Sweden at 1 year after discharge of HF admission.8) Additionally, regarding the guideline adherence drug score by race, each country had a different score; in particular, Korea had a relatively low score compared to Western countries.14) The novel GDMTs, ARNI or SGLT2 inhibitor, tended to be more highly prescribed in diabetes mellitus (DM) or chronic kidney disease patients.8) This is thought to be because of the renal protective effect of these drugs, as confirmed in a recent study, and only DM patients were targeted at the beginning of the study based on SGLT2 inhibitor.29)44)45)46)47)48) However, recent studies on SGLT2 inhibitor (dapagliflozin and empagliflozin) have shown favorable results regardless of DM, and their effectiveness has been demonstrated not only in HFrEF but also in HF with preserved ejection fraction; an active administration protocol is thus warranted.49) Socio-economic status, lack of formal education, and low health knowledge may also be major contributors to low prescription rates and it is directly related to poor drug adherence.50) Patients living in high-income areas received more than 6 times more GDMT than those living in low-income areas.
Healthcare provider-related factors
Physician-related factors are known to contribute the most to clinical inertia.51) Several surveys have shown that even when physicians follow guidelines, many patients do not receive optimal care.52) This is because physicians overestimate health care they provide and underestimate the needs of their patients. Physicians prescribe GDMT; however, insufficient control management of its administration led to persistent clinical inertia. In addition, physicians often overemphasize on patients’ tolerability or side-effects of certain drugs to patients, and complain about their non-compliance or time constraints. Lack of education or training program, motivation, awareness and knowledge of patients are well-identified contributors.9)53) Studies have shown that effectiveness increases when a patient is treated by a doctor who is familiar with and has experience with the patient.9) Therefore, continuing medical education for both physicians and patients and improving organizational management are essential to improve HF treatment.
Healthcare system related-factors
Differences and inequalities in healthcare between and within countries can affect adherence of GDMT. Inequalities in drug reimbursement are a major obstacle. There are many differences in national healthcare policies, public function and services. In many countries, GDMT are reimbursed prescription, but in some countries, there is still no public funding. In particular, only a part is fully reimbursed in the case of novel drugs such as ARNI and SGLT2 inhibitor.9) National Finance and medical expenses are another barrier to providing GDMT.54) The higher the total government health expenditure and the lower the out-of-pocket health expenditure, the higher the GDMT rate.50) In addition, awareness of the importance of domestic specialized HF centers, availability or accessibility of HF centers, communication between primary and tertiary hospitals, and continuity of physician care are important factors.9) In addition, global issues such as the coronavirus disease 2019 (COVID-19) pandemic may also be a factor influencing compliance with the GDMT. A recently published study found that hospital care following the COVID-19 pandemic was similar to that observed during the pre-COVID-19 period. However, the prescription rate of triple drugs for HFrEF at discharge in patients with COVID-19 was significantly lower than that in patients without COVID-19.55)
In Korea, as the proportion of the elderly population in their 70s and 80s is increasing, the percentage of patients with comorbidities is also high; on average, 5.3 medications are taken per person over the age of 65. In addition, Koreans have relatively low body weight and are more fragile than Westerners; therefore, there is a limitation in the up-titration of GDMT. Recently, novel treatments are being introduced, but their benefits are delayed due to financial limitations of health insurance, and appropriate managements cannot be implemented due to high pharmaceutical expenses. However, the reimbursement criteria for ARNI and SGLT2 inhibitor have been expanded in recent clinical trials; GDMT adherence can therefore be expected to increase. An ongoing clinical trial called the Optimize Heart Failure Care During Transitional Period in Patients with Acute Heart Failure (TRANS-HF) registry is underway to identify the cause of the lower use of GDMT in Korea (NCT04900584).56) Although as yet unpublished, in this trial, more than 30% of drug noncompliance was due to unexplained reasons and it was thought to be influenced by clinical inertia. Therefore, it is necessary to enthusiastically promote GDMT through vigorous change and control for factors other than those related to patients’ comorbidities of side effects, especially those in the field of physicians and healthcare.
Go to :
HOW TO IMPROVE QUALITY OF CARE FOR HEART FAILURE
HF is a representative disease that is treated with evidence-based treatment strategies.40)57) Most guideline recommend rigorous, evidence-based treatment strategies that have demonstrated reductions in mortality and major morbidity. Therefore, it is very important for medical staff to understand the latest treatment guidelines and establish the best treatment plan for each patient. Although clinical outcomes can be improved by establishing guidelines through academic reports based on randomized control trials and registry data, the improvement in mortality or morbidity does not coincide with increases in quality of life. Thus, while efforts on GDMT are needed, efforts must also be focused on improving our awareness of the effects of these treatments on patients, particularly whether patients experience side effects and how it is important to the patients themselves. Measuring treatment outcomes and evaluating clinical quality indicators in patients with HF can help improve the quality of HF care and patient prognosis.
Performance measure and enhancing the quality of care for heart failure
The performance measure is an indicator of HF care quality. It is an objective measurement of treatment and clinical outcomes and consequently increase the efficiency and effectiveness of specific programs. Performance measures are standards of care that involve the performance of definitive diagnostic or therapeutic actions according to a set of standards; physicians that fail to comply with these standards may be held to be in error.58) These evidence-based performance measures will bring meaningful outcomes for patients and society and should also be valid, reliable, interpretable, actionable, explicitly definable and adjusted for patient variability.58)59) Performance measures are developed in different nations through government agencies, relevant organization, and medical payers that have instituted programs to promote improved clinical care for HF hospitalized patients.60)
In the US, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has established 5 in patient HF performance measures; the Agency for Healthcare Research and Quality defines quality indicators in detail by dividing them into preventive quality indicators, hospitalization quality indicators, and patient safety indicators.61)62) Quality indicators are included in current clinical practice guidelines to facilitate quality improvement. The ACC/AHA HF guideline contain quality indicators from admission to hospital discharge for HF; the determination of these indicators is based on evidence and the clinical situation.5)63) The guidelines contain thirteen of clinical performance measures, 4 of quality measures, one of structural measure, and 2 of rehabilitation performance measures (Table 1). In addition, they also include an assessment of overall HF mortality, HF readmission rate, 30-day mortality rate, and 30-day readmission rate for HF, and apply these standardized performance measures to improve readmission rates and mortality rates. In particular, the AHA implemented the ‘Get with the Guideline (GWTG)’ quality improvement program and improved prognosis by increasing the achievement of each institution’s performance measurement.64)65) The ESC HF guideline also emphasize the effective application of quality control indicators and performance evaluation, and quality indicators are divided into 5 domains (structural framework, patient assessment, initial treatment, therapy optimization, and assessment of patients health-related quality of life) (Table 1).6)66) When selecting clinical quality indicators, measurability, reproducibility and ease of use should be evaluated for each item, and decisions should be made by excluding conflicts of interest between various institutions. Although standardized quality management indicators have not yet been developed in Korea, the Korean Society of Heart Failure guidelines recommend evaluating quality measurement based on ESC guidelines, considering the usefulness of their clinical application.
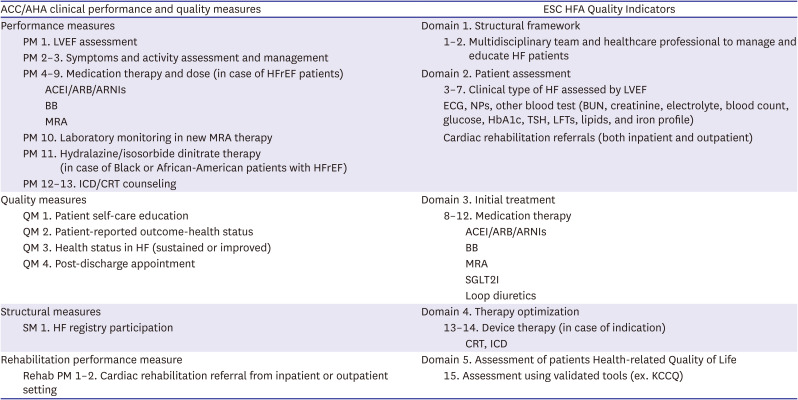
Table 1
ACC = American College of Cardiology; ACEI = angiotensin converting enzyme inhibitor; AHA = American Heart Association; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor/neprilysin Inhibitor; BB = beta-blocker; BUN = blood urea nitrogen; CRT = cardiac resynchronization therapy; ECG = electrocardiography; ESC = European Society of Cardiology; HbA1c = hemoglobin A1c; HF = heart failure; HFA = Heart Failure Association; HFrEF = heart failure with reduced ejection fraction; ICD = implantable cardioverter defibrillator; KCCQ = Kansas City cardiomyopathy questionnaire; LFT = liver function test; LVEF = left ventricular ejection fraction; MRA = mineralocorticoid receptor antagonist; NP = natriuretic peptide; PM = performance measure; QM = quality measure; Rehab = rehabilitation; SGLT2I = sodium-glucose cotransporter-2 inhibitor; SM = structural measure; TSH = thyroid-stimulating hormone.
![]()
The need for these performance measure is well demonstrated in the Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVE-HF) registry results.67) The proportion of patients receiving GDMT after 24 months increased when interventions that monitor the appropriate use of ACEI/ARB, BB and MRA, device therapy (cardiac resynchronization therapy or implantable cardioverter defibrillator), and education for HF patients were implemented. Given that GDMT is essential for reducing mortality and morbidity, it is important to improve the quality of HF care using these performance measures. In a study on the conformity of JCAHO using the Acute Decompensated Heart Failure National Registry, hospitals that assessed discharge instructions, left ventricular function measurements, ACEI use, and smoking cessation had significantly lower lengths of stay and lower mortality rates compared to other hospitals that did not assess them.68) The OPTIMIZE-HF is the largest national hospital-based registry to improve management and education of HF patients.69) This study showed that the composite rates of mortality or hospitalization and in-hospital mortality for HF were significantly lower in the group that used care tools (admission order set or discharge checklist) than in the group that did not. The achievement of active clinical quality indicators and the use of performance indicators can improve patient prognosis. In addition, the GWTG-HF score based on the AHA GWTG-HF program data is known to predict in-hospital mortality in patients with acute HF.65) In a study that applied this to Japanese patients and confirmed the clinical significance of the GWTG-HF score, it was confirmed that the cardiovascular event increased 1.58 times for every 10-point increase in the GWTG-HF score.64) A recent study found that an electronic health record-based system for outpatients with HFrEF increased GDMT rates at day 30 when compared to usual care group (25.7% vs. 18.7%, p=0.03).70) This intervention can be rapidly incorporated into clinical practice, accelerating the application of low-cost, high value managements in HF.
The UK has traditionally emphasized quality of care and created an objective basis through a unique structural and systematic approach. To improve the quality of effective medical treatment, the National Institute for Health and Care Excellence (NICE) of the UK provides guidance on program to enhance the quality of HF care in patients with HF.71) The NICE quality standards are a set of standards designed to improve attainable indicators of patient safety, patient experience, and clinical effectiveness in the HF domain. Table 2 shows the list of quality statement (QS) for HF management in NICE. Seven QSs are presented, and the importance of each item is explained from the point of view of HF specialists, healthcare providers, and HF patients. All specialists and healthcare providers should have sufficient and appropriate training and competence to manage these QSs, and the training of the relevant staff should be considered. It also recognizes that families and caregivers play an important role in care of patients with HF, and therefore emphasizes the participation of family members and caregivers in decision-making about diagnosis, treatment, and management. According to the report, these QS achievement rates improved treatment scores from 63% to 76%, and mortality and HF hospitalization rates when compared with before.71)

Table 2
![]()
To improve the quality of HF treatment, it is important to create and implement performance measures or clinical indicators tailored to each country’s circumstances. In addition, to develop a program to improve the quality of HF care, it is required to encourage the participation of healthcare providers led by the government or a specific subject group.
In-hospital strategies for improving implementation of guideline-directed medical therapy
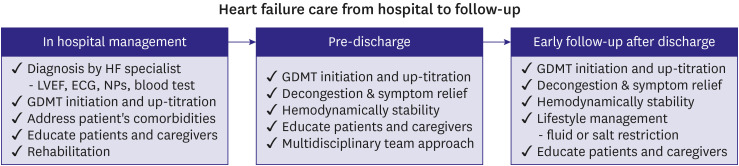
Mortality is particularly high in the early stages of hospitalization; patients with HF often undergo repeated hospitalizations,72) each of which causes myocardial and renal damage and contributes to the inevitable vicious cycle.73) Hospitalization is therefore a critical moment in optimizing treatment and discharge if it is the “beginning” of the HF treatment journey. The ESC guidelines recommend initiating and up-titrating pharmacology and device therapy to improve quality of life and survival rates and prevent early readmission of patients with acute HF.6) ACC/AHA guidelines also recommend that GDMT should be started during hospitalization and should not be discontinued if it is taken.5) However, in actual clinical practice, it is very rare for acute HF patients to start or rapidly up-titrate medication due to safety concerns regarding side effects, and in most cases, the drug is discontinued. Recent studies have shown that early and active interventions are important. The STRONG-HF trial demonstrated that a high-intensity strategy during hospitalization and early post-discharge monitoring is safe and decreases readmission for HF or all-cause mortality rates and improves quality of life for HF patients.24) In addition, a recently published the Comparison of Outcomes and Access to Care for Heart Failure (COACH) trial showed that an early intervention improved clinical outcomes in patients with acute HF. Risk stratification using a specific tool can be used to determine hospitalization or rapid outpatient follow-up at emergency room, reducing all-cause death and hospitalization for cardiovascular-cause within 1 month.74) Evaluation of management is important, but appropriate intervention for patients in the early stage is also important to reduce the clinical events. The NICE guidance in the UK emphasizes the quality of care for patients with acute HF and provides a list of QS as in chronic HF (Table 2).75) NICE guidance includes intervention by HF specialists within 24 hours of admission, evaluation including transthoracic echocardiography within 48 hours, initial use of ACEI/ARB, BB, and MRA, and follow-up clinical assessment within 2 weeks of discharge in patients with acute HF.
Implementing quality of care programs during hospitalization has the advantages of longer contact times between patient and medical staff, ease of application of programs or checklists, and better use of a multidisciplinary team approach for patient or caregiver education or rehabilitation. In addition, it enables easy monitoring of drug reactions, including side effects. However, in the initial stage of hospitalization, many unstable patients require aggressive treatment, and the hospitalization period can be extended for performance measurement. The performance measure for patients with chronic HF aims to reduce hospitalization and improve the ability to manage long-term conditions and medication safety. For patients with acute HF, performance measures aim to reduce major cardiovascular event rates, lengths of hospitalization, readmission rates, and adverse events. Ultimately, the goal for management of both chronic HF and acute HF is to reduce mortality and increase quality of life. Therefore, regardless of whether it is chronic or acute HF, it is most important to create an appropriate performance measurement program and apply it appropriately in clinical practice (Figure 4).
The need for education programs for heart failure professionals and heart failure patients
GDMT clearly reduces mortality and morbidity in patients with HF. Physicians play an important role in prescribing GDMT. However, because clinical inertia occurs even for experienced physicians, physicians and nurses should increase their awareness of HF and receive ongoing education about its management.53) A systematic review and meta-analysis showed that HF self-management training by nurses with HF expertise improves clinical outcomes.76)77) However, since there is still a shortage of professional nurses in many countries, it is essential to recognize the need for such professional nurses and to recruit them.9) Continuing education on clinical inertia is essential for nurses as well. In addition, there is a need for education regarding patients receiving direct treatment. Establishing a system of formal education and support intervention can help reduce 1-year readmission rates and medical costs for patients with HF.78) Just one-hour of education upon discharge could improve clinical outcomes and increase adherence to self-care measures.79) Patient self-management is also very important in reducing deaths and hospitalizations due to HF. HF patients who are good at self-management have a good quality of life and a good clinical prognosis.80) Therefore, HF societies should increase learning opportunities through educational conferences or seminars, and information transmissions through materials such as brochures and flyers, social media, the Internet, and mobile phones. HF professionals, including physicians and nurses, must raise public recognition of HF and provide ongoing education and appropriate treatment to patients and their families.
The role of national policy for high quality of heart failure care
Adherence to clinical guidelines improves the outcomes of patients with HF. However, there are significant differences across countries in how hospitals follow national HF guidelines.81) While it is important to promote HF education programs to raise awareness of the guidelines among healthcare professionals, it is also important for countries to develop specific policies to improve the quality of HF diagnosis and treatment. Such policies may include encouraging improvement in care using locally appropriate performance measures and incentives, and funding research to measure evidence-based health outcomes. Each policy should be tailored to the circumstances of the country. Patients in low- and middle-income countries are less aware of HF symptoms due to lack of access to hospitals and health insurance. Therefore, in low-income countries, there is a need for performance measures tailored to reflect the local circumstances. In addition, since the underlying causes of HF also vary worldwide, specific policies for developing and preventing HF must be devised for each country.81) Country-based policies can assess patients care quality and outcomes through audits and registry operation that reflect real-world practice to increase guideline compliance through real-world, case-based feedback. NICE in the UK collects information from inpatients with HF and proves whether the introduction of a HF specialist team and increased adherence to guideline recommendations reduced the survival or readmission rates.71)75) Professional initiatives such as GWTG in the US provide advice and support to improve compliance with the guidelines.64) Such policies may encourage enhancements in hospital performance by providing monetary rewards or imposing monetary penalties.81) In addition, since incentives and management systems for HF care should be based on evidence through clinical trials, policymakers should actively support activities that promote evidence-based research. In conclusion, extensive data collection through registries and audits as well as the promotion of evidence-based research on clinical outcomes should be implemented under national initiatives.
Multidisciplinary treatment and cardiac rehabilitation
Multidisciplinary treatment (MDT) is highly recommended in most HF management guidelines to improve the quality for HF care. The ESC guidelines also assess the presence of a multidisciplinary team as a structural quality indicator.6)66) As HF is a multisystem dysfunction, the use of MDT to recognize these complexities and address the disease in multiple dimensions is a gold standard model. In several meta-analyses, MDT has been demonstrated to reduce mortality and hospitalizations.82)83)84) MDT also has a positive impact on cost-effectiveness of care delivery, patients’ quality of life, and increased GDMT and medication adherence.79)82)85)86)87) Cardiac rehabilitation is a representative MDT. It is recommended for all HF patients to improve quality of life and exercise capacity, and reduce readmission for HF.88)89)90)91) Studies have shown that cardiac rehabilitation reduces overall or HF readmissions in patient with HFrEF, and a higher exercise participation rate is associated with lower hospitalization rates.6)88)89)90)91)92)93) To increase the cardiac rehabilitation participants, it is necessary for healthcare providers and patients to recognize the necessity of rehabilitation and to ensure that all patients receive cardiac rehabilitation as much as possible.94)
Cooperation with HF specialists, professional nurses, pharmacists, nutritionists, physical therapists, psychologists, and social workers is important. HF specialists should lead the MDT, and professional nurses are a key part of the clinical team.87) Essential management practices that a HF multidisciplinary team should be able to implement include HF progress monitoring, optimization of HF treatment, management of comorbidities, HF education for patients and caregivers, lifestyle modifications such as diet and exercise, and psychosocial assessment, palliative care, and appropriate counseling. MDT should engage patients as early as possible and be easily accessible throughout the entire disease process. MDT enables trust-based care by providing continuity of care and taking responsibility for individual patient care. When discharged, all team members must be involved in the detailed planning and communication with the patient and family.
HF is a complex disease and MDT improves outcomes by reflecting the characteristics of HF. There is no defined MDT, and it must be applied according to each country, region, or center. It is clear that MDT improve the quality of HF care.
Go to :
CONCLUSION
As the burden of HF increases, it is necessary to manage and treat HF effectively. First, it is important to optimize treatment based on evidence-based guidelines to the greatest extent. There is still poor drug adherence, and many patients do not receive GDMT, including RAS blockers (ACEI, ARB, or ARNI), BB, MRA, and SGLT2 inhibitor, especially at the early stages. To improve medication adherence, qualitative evaluation through performance measurement as well as education of patients, caregivers and medical staff through a multidisciplinary approach are important (Figure 5).
Go to :
 XML Download
XML Download