

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary vein isolation (PVI) is the standard of care in the interventional treatment of atrial fibrillation (AF).1) Worldwide, thermal energy sources by terms of radiofrequency (RF) and cryoballoon ablation are the leading techniques to perform PVI and have demonstrated satisfactory outcome results and safety profiles.2) Recent randomized studies highlighted the importance of PVI by showing advantageous results of an early interventional treatment alongside with a decreased risk of adverse outcomes even in asymptomatic AF patients with concomitant cardiovascular conditions3) and superior outcomes as compared to antiarrhythmic drugs.4)5) This leads to extended indications for PVI with an increased number of procedures to be expected to be performed worldwide. However, even after years of experience and significant technical advancements6)7) there are certain limitations of thermal energy-based ablations. In RF ablation, lesions are usually created point-by-point, which can be technically challenging and time consuming. Here, lesion transmurality depends on the experience of the operator with respect to catheter stability/catheter-tissue contact and is negatively influenced by larger nearby vessels (heat sink effect) or tissue properties (fat pads serve as insulators). Cryoballoon ablation, however, can be challenging in complex anatomies regarding optimal coaxial balloon alignment at the pulmonary vein (PV) ostia, and, as a single shot device it is mainly limited to PVI. Furthermore, thermal energy is not solely addressing the myocardium, e.g., collateral tissue damage can occur and potentially result in severe adverse events, such as esophageal complications (e.g., atrioesophageal fistula),8) phrenic nerve palsy9)10) or PV stenosis.11)12) In RF ablation, there is an additional risk of thromboembolic events through tissue coagulation13) and in cryoablation, ice formation in the bronchial system leading to hemoptysis or ulcers formation has been described.14) Therefore, continuous technical developments are desired to improve the efficacy and safety profile of the procedure. Pulsed field ablation (PFA) is considered a non-thermal, tissue-sensitive treatment alternative in interventional electrophysiology since myocardial cells are more susceptible to electroporation than surrounding structures. Its current field of application is mostly AF ablation, e.g., PVI,15) but other ablation approaches in the atria or ventricles have been investigated in animal models16)17)18)19) and as an off-label use in humans.20)21)22) The technique utilizes high amplitude pulsed electrical fields that are exposed to sensitive myocardial cells, which leads to subsequent cell death through the mechanism of irreversible electroporation (IRE). Electroporation acts by increasing the permeability of the cell membrane after exposure to electric fields.23) Earlier pre-clinical and first investigations of PFA in clinical practice have demonstrated remarkable results by means of creating transmural and durable myocardial lesions in a time-efficient and safe procedure without affecting adjunctive tissue.15)24)25)26)27) These unique characteristics might enable PFA to become the treatment of choice to perform catheter ablation of arrhythmias. This review focuses on the pearls and pitfalls of PFA (Figure 1) with emphasis on the clinical perspective based on current literature as well as already available and upcoming PFA technologies.
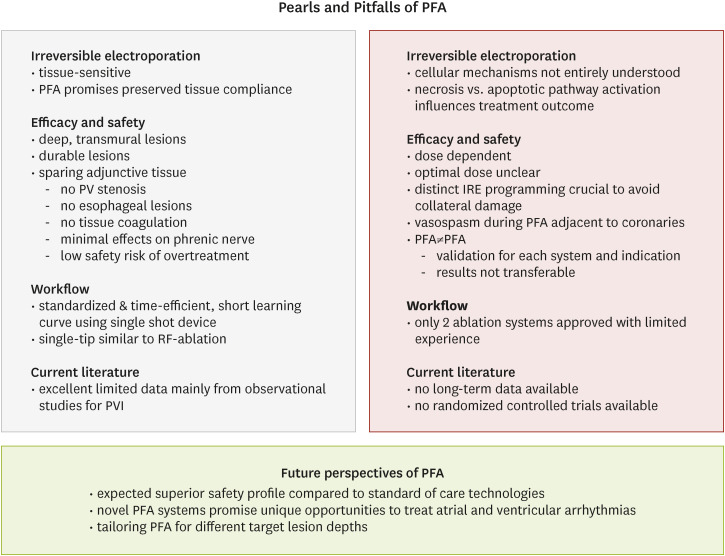 | Figure 1Pearls and Pitfalls of PFA. Summary of the main “pearls” (light green) and “pitfalls” (red) of PFA as well as the future perspectives of the technology.IRE = irreversible electroporation; PFA = pulsed field ablation; PV = pulmonary vein; PVI = pulmonary vein isolation; RF = radiofrequency.
|
Go to : 
ELECTROPORATION AND PULSED FIELD ABLATION
History of electroporation in medicine
The exposure of sufficiently strong electrical fields on cells results in a transient or permanent increase in the permeability of the cell membrane, a mechanism that is referred to electroporation. Since electroporation is applicable to any biological cell, the areas of application are various and have been well-known in the food industry, the pharmaceutical sector, plant sciences and others28) before its implementation in the medical field. The principle of electroporation with its use in medicine dates back to 1982 when its name givers applied pulsed electric fields to enable the delivery of foreign DNA into cells.29) Afterwards, clinical applications to treat tumors have been developed such as electrochemotherapy to deliver chemotherapeutics into tumor cells,30) gene electrotransfer to deliver DNA or RNA into cells to induce anti-cancer effect31) and the ablation of solid tumors through IRE.23)32)
Initial experiences in cardiac electrophysiology
In cardiology, first attempts that were related to the effects of electroporation were described in 1982 by delivering single monophasic shocks of high amplitude (direct current, DC) for atrioventricular nodal ablation to treat supraventricular arrhythmias as an alternative strategy to open-chest surgical procedures.33)34) However, the extent of the ablated tissue was hardly to control and the approach put the patient at risk of barotrauma and arcing and was replaced by the more elegant RF ablation in the 1990s.35) Nowadays, the quality of pulsed electric fields can be adapted and better controlled by a specific electroporation protocol that includes a series of electrical pulses with a determined voltage amplitude, pulse width, and repetition frequency,32) which is why electroporation is again been considered for cardiac ablation procedures.
Technology
Biophysics: a brief overview
Each biological cell is surrounded by a bilayer lipid plasma membrane that contains several proteins serving as ion pumps or channels allowing for transportation of specific molecules between the inside and outside of the cell. For other substances, it serves as a biological barrier to protect the cell from its environment. The lipids of the plasma membrane consist of a hydrophilic (polar) und hydrophobic (non-polar) part. Together with the ion pumps and channels, the cell maintains an electric potential difference between the inner and outer side of the plasma membrane. The so-called resting transmembrane voltage ranges from −40 to −70 mV in eukaryotic cells. The exposure of cell membranes to an electrical field exceeds the transmembrane voltage and can—if it is strong enough—influence the electrical conductivity and increase the permeability of the membrane by creating aqueous pores. This allows transmembrane transport for usually impermeable molecules and subsequently leads to alteration of cell integrity. Depending on the strength of the electrical field, effects on cell integrity can be transient, e.g., the cell can re-establish its electrical and structural integrity, or irreversible, e.g., consequently leading to cell death.36) Cell death after exposure to electric fields can be primarily necrotic or initiated via different apoptotic pathways. Specifically, necrosis, apoptosis, necroptosis and pyroptosis have been mentioned in the context of electroporation.37) The exact mechanism of (co-activated) cell death pathways, following different pulsed electric field protocols is, however, less understood and can affect treatment outcome and hamper the comparability of different protocols. For the treatment of cardiac arrhythmias, the aim is reaching the state of IRE. Successful IRE is influenced by multiple factors. Most importantly, the required electrical field strength depends on the cell type38) and therefore, electroporation protocols must be tailored relating to the target tissue and cannot be adopted from existing results of other areas. A relevant secondary effect of electric current is the increase of tissue temperature due to energy dissipation which occurs when electric current encounters tissue that resists the current (Joule heating). Heating is proportional to the square of the delivered current and to its application time. Thus, it is important to bear in mind that electroporation is not per se non-thermal and that affection of adjacent tissues39)40) through Joule heating is possible. The undesired effect of Joule heating for cardiac electroporation procedures needs to be considered while designing electroporation protocols to allow effective cardiac ablation without significant tissue heating. Another secondary effect of electroporation is the formation of gaseous microbubbles due to electrolysis that has been described after application of monophasic pulses.41)42) This can potentially lead to thromboembolic complications. However, both cerebral magnetic resonance imagings (MRIs) and cerebral histology of dogs did not show cerebral events after 200 J monophasic anodal applications.43) Shorter pulses and anodal applications were associated with significantly less,41) and biphasic pulses with no gas bubble formation,44) respectively. Monophasic current (DC) was most commonly used for electroporation in the past, but may be associated with painful nerve and muscle capture45) or arcing.46) These possible side effects can be overcome by biphasic/alternating current (AC). A proof of concept study has demonstrated feasibility and safety of AC-PFA in the atrial and ventricular myocardium of swine,44) others have shown reduced muscle contractions and pain in human tibialis anterior muscles using biphasic high frequency pulses.47) Electroporation protocols contain several parameters that can be adapted, e.g., voltage, number of pulses, pulse width, pulse shape, pulse delay and frequency.48) The electric field can be delivered in the form of mono- or bipolar pulses usually applied over nano- or milliseconds, as single pulses, or hundreds of pulses within one or several bursts of applications.49)50) The pulse shape can be rectangular, triangular, sinusoidal, or exponentially decaying.51)
Figure 2 exemplarily depicts pulsed electric field waveform characteristics and parameters to be considered when designing electroporation protocols. Additionally, local tissue properties, cell size, cell geometry and cell orientation to the electric field vector and therefore also catheter shape and electrode arrangements influence successful IRE.52)53)
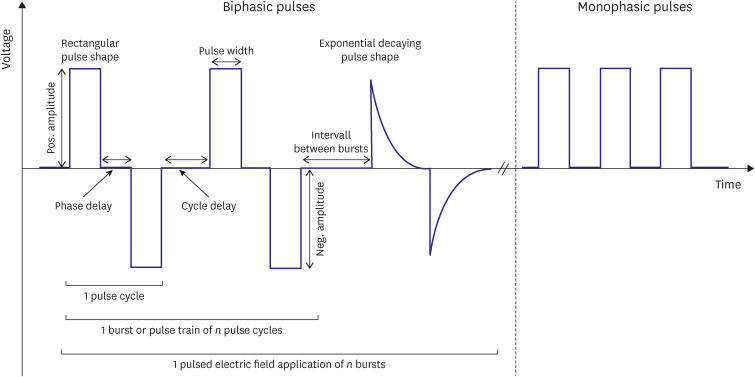 | Figure 2Pulsed electric field waveform parameters. An exemplary overview of the most relevant pulsed electric field waveform characteristics and adjustable parameters for designing electroporation protocols. Each parameter setting and various pulse shapes available, its combinations and alterations result in different electric field strengths and influence the effect of electroporation, successful ablation, and safety.
|
Tissue sensitivity
The phenomenon of electroporation comes to effect when the transmembrane voltage reaches a certain threshold that is unique for each tissue or cell. The IRE threshold for cardiac cells is lower than that of surrounding tissues, such as nerves (3,800 V/cm),54) vascular smooth muscle cells or the endothelium (each 1,750 V/cm).15)55) Individualized data for cardiac electroporation thresholds are derived from cellular studies. However, different non-standardized electroporation protocols with inconsistent pulse parameters applied (and pulse parameter definitions) and the use of different electroporation generators complicate comparability, reproducibility of data and translation into human studies.56) Exemplarily, cellular data using different electroporation protocols resulted in different electroporation thresholds: 375 V/cm for rat myoblasts,57) 500 V/cm for rat ventricular cells (resulting in 80% cell death),58) 750 V/cm for human cardiomyocytes,59) and 1,250 V/cm for another cardiac cell line,60) respectively. With respect to the biophysical properties, it is crucial that any working system, i.e., the combination of a generator and an ablation catheter, requires its own qualified IRE protocol with individual electrical pulse settings approved for the system.
Effects on myocardium and safety to adjacent tissue
In 2007, Wijffels et al.61) described electrogram alterations and tissue lesions around the electrodes in the atria of goats after internal DC shocks via standard diagnostic electrophysiology catheters, which might have been the occasion to reconsider the abandoned ablation technique for cardiac indications. Almost at the same time, the first studies on the effect of electroporation on the myocardium were conducted and its benefits were demonstrated. Lavee et al.16) performed successful electrical isolation of the atrial appendage(s) in a surgical procedure in swine and demonstrated transmural lesions at all sites of application. In 2011, Wittkampf et al.62) were the first to perform ostial PV ablations using a decapolar circular ablation catheter via a transseptal endocardial approach and proved feasibility and safety in a pilot study in swine with DC applications below the arcing threshold (200 J applied by an external defibrillator). Van Driel et al.24) reported that circumferential 200 J electroporation applications within the PV ostia were not associated with PV stenosis during follow-up. Witt et al.25) confirmed these findings using a prototype balloon ablation catheter in canines. Here, the balloon was positioned inside the PV and at the PV antrum. DC energy was delivered between 2 local electrodes of the balloon. Additionally, the group described transmural lesion formation and no injury to the esophagus or other significant adverse events related to electroporation were noted during 1 month follow-up. In another animal study, the architecture of the esophagus remained unaffected acute and long-term after applying DC energy with up to 200 J directly on the adventitia of the esophagus. Histologically, a small scar was noted at the outer part of the muscularis, whereas the mucosa and submucosa were described normal.63) Others have shown intact epithelial surfaces after esophageal electroporation ablation.17) To investigate the effect of electroporation on the phrenic nerve, Van Driel et al.64) performed electroporation ablation at the superior vena cava with a circular ablation catheter and a single 200 J application. Diaphragmatic contractions were observed in the animals immediately after energy application and rarely within a 30-minute delay. Phrenic nerve function remained unaffected after the procedure and during follow-up several weeks after. However, phrenic nerve response has shown to be dose dependent and was associated with catheter proximity.65) Transferred into clinical medicine, the electrophysiologist should keep in mind that phrenic nerve affection is possible during PFA. Although no persistent phrenic nerve palsies have been observed at this point of time,27) additional data are valuable to proof these findings.
In 2009, Hong et al.17) developed 2 systems using a bipolar clamp device or a linear surface probe to perform epicardial electroporation after thoracotomy in sheep in the context of a feasibility study. In addition to electroporation in the atria, transmural lesions were also proven after electroporation in the right ventricular outflow tract and the left ventricular free wall. A further animal study on ventricular electroporation near or even on coronary arteries demonstrated deep lesions and the presence of coronary artery blood flow did not seem to affect myocardial lesion formation. Repeated coronary angiography and histological studies did not reveal any long-term adverse effects on coronary arteries. However, transient coronary artery narrowing immediately after ablation was suggestive of coronary spasm.66) Similar results with absence of major complications related to electroporation were proven with different catheters and epicardial accesses. With energy titrations up to 300 J, the lesion size was significantly larger,67)68)69) while the coronary arteries remained unaffected also in the long-term.68)69) Ablation within the coronary sinus (CS) is necessary in some ablation procedures. Buist et al.18) have demonstrated feasibility of electroporation in the CS in a porcine model. In a proof-of-concept study, Koruth et al.19) investigated electroporation of the ventricular myocardium with a prototype focal ablation catheter inserted via a transfemoral access in swine. The results showed homogeneous, deep lesions specific to the myocardium in a safe procedure.
More recently, Zager et al.48) have demonstrated in an animal study that IRE had a graded effect on the myocardium, i.e., the extent of ablated tissue increased with higher output, longer pulse duration and a larger number of pulses. Balancing these parameters is essential for a safe and effective ablation. Baena-Montes et al.59) reported that pulse timing or the burst number, rather than the absolute field strength, may be superior parameters to generate a more predictable ablation area. At lower field strengths, the authors observed a delayed cell death within hours presumably via the selective activation of apoptotic pathways (which could be advantageous by minimizing inflammatory and immunogenic responses) rather than acute necrosis that predominantly occurs at higher field strengths.59)
Based on the aforementioned studies demonstrating pearls and potential pitfalls of electroporation, PFA systems have been developed for the application in clinical medicine and PVI for the interventional treatment of AF has been the first target of PFA to be investigated.70)
Go to :
PULSED FIELD ABLATION SYSTEMS
To date, only the FARAPULSETM and CENTAURITM PFA systems have a CE-mark and are approved for routine clinical use in Europe. Other systems are investigated in pivotal clinical trials. All studies published have prospective observational designs and so far, no randomized controlled studies comparing PFA to standard of care technologies have been completed.
FARAPULSETM system
The FARAPULSETM PFA system (FARAPULSE, Inc., Menlo Park, CA, USA) consists of an ablation catheter, steerable sheath, and a generator. The FARAWAVETM ablation catheter is a 12.8F over-the-wire tool with 20 electrodes. The deployable distal part of the catheter is available in 31 mm and 35 mm maximal diameter dimensions, consists of 5 splines with 4 electrodes each and can be shaped as a flower petal (maximal diameter) or variable basket morphologies through a slide control mechanism on the handle of the catheter. All electrodes allow delivering of pulsed electric fields, and the third electrode on each spline enables electrogram acquisition and pacing. The ablation catheter is inserted through a 13F (16.8F outer diameter) steerable sheath (FARADRIVETM). The sheath is translucent and easily allows checking for possible air bubbles after inserting the ablation catheter and removing them. For each PFA application, the FARASTARTM generator outputs proprietary bipolar, biphasic pulses applied between the adjacent splines of the ablation catheter over approximately 2.5 seconds.15)70) The voltage amplitude (1.8, 1.9 or 2.0 kV) is the only parameter that can be adjusted. Meanwhile, 5 pulses with a fixed waveform and a voltage amplitude of 2.0 kV are recommended for one PFA application according to data from initial procedures.15) The IMPULSE and PEFCAT trials were the first in-human investigations that have proven feasibility of the system demonstrating ultra-rapid PVI with excellent durability and safety.15) Mean catheter LA dwell time was 33.7±16.6 minutes, which is remarkably shorter than reported for cryoballoon (92 minutes) or RF ablation (109 minutes) in the FIRE AND ICE trial.2)
The PersAFOne trial has proven feasibility and safety of PVI and posterior wall isolation in patients with persistent AF71) and has paved to way for the technique to be performed in more progressed forms of AF. Further (follow-up) studies are on the way, e.g., PersAFOne II (NCT05152966) and PersAFOne III (NCT05272852). Additional clinical studies have been published and will be presented later in the manuscript. The system is commercially available in Europe since January 2021. Figures 3 and 4 show the FARAPULSETM system for fluoroscopy guided-PVI and a complex left atrial procedure with integration in a 3-dimensional (3D) electroanatomical mapping system.
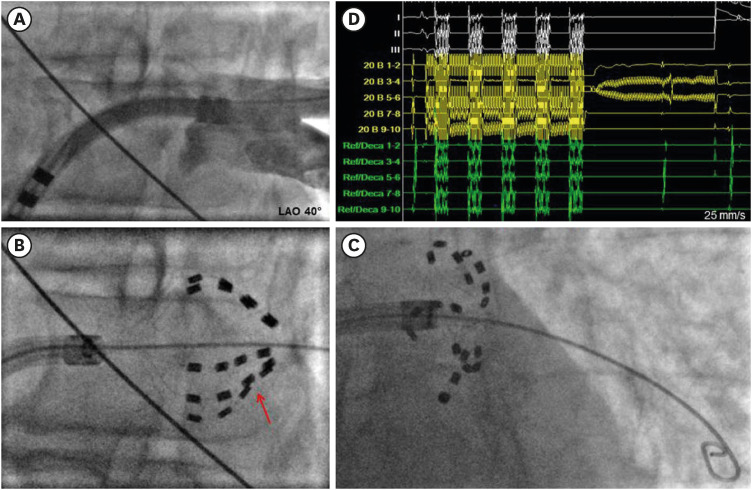 | Figure 3Pulsed Field Ablation with the pentaspline catheter for PVI. Fluoroscopy-guided PVI using the FARAPULSETM system. Fluoroscopic images in LAO 40°. (A) PV angiography of the left inferior PV illustrates the PV ostium to ease optimal catheter placement. (B) Pentaspline catheter is positioned at the PV ostium in basket configuration. The indentation of the splines (arrow) suggests catheter-tissue contact. (C) Pentaspline catheter in its flower position. The backward flexing suggests catheter-tissue contact. A J-tip guidewire was advanced deep inside the PV to improve catheter stability. (D) Electrograms during pulsed electric field application (white: surface electrocardiogram, yellow: pentaspline ablation catheter, green: coronary sinus catheter). Note the attenuation of the atrial electrograms of the pentaspline catheter (yellow) after the first of in total 8 applications per PV.LAO = left anterior oblique; PV = pulmonary vein; PVI = pulmonary vein isolation.
|
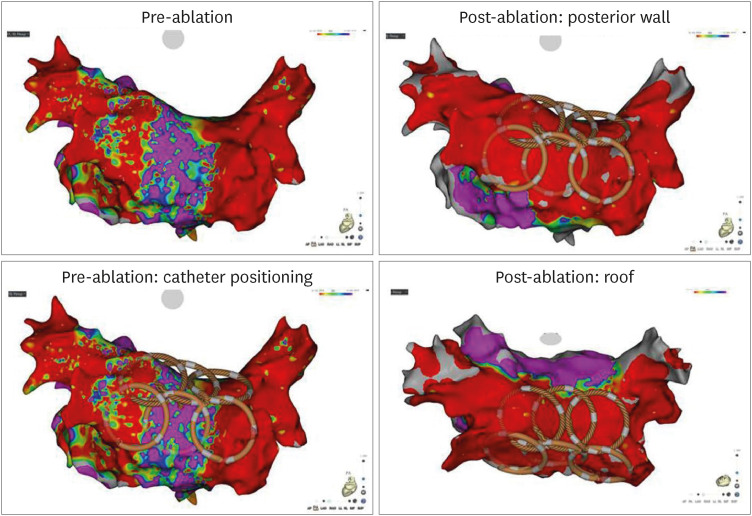 | Figure 4Visualization of the pentaspline pulsed field ablation catheter in 3-dimensional electroanatomical mapping system to guide LA posterior wall isolation and roof isolation. The FARAPULSETM ablation catheter in flower configuration for LA posterior wall isolation and LA roof isolation in a patient after multiple prior LA procedures and significant atrial fibrillation burden. Empirical re-ablation of all durably isolated PV was additionally performed under fluoroscopic guidance. Shown are voltage maps generated with the PENTARAYTM mapping catheter (Biosense Webster, Diamond Bar, CA, USA) in a posterior-anterior projection. Voltage settings were 0.10–0.50 mV. Pre-ablation maps (left panes) show a diseased left atrium, and catheter visualization of in total 6 ablation locations in the CARTO®3 electroanatomical mapping system (Biosense Webster). Post ablation voltage maps (right panes) demonstrate isolation of the posterior wall, the LA roof (posterior-anterior view oblique to roof) and the PV.LA = left atrium, PV = pulmonary vein.
|
CENTAURITM system
The CENTAURITM PFA system (Galvanize Therapeutics, Inc., San Carlos, CA, USA) is commercially available in Europe since August 2022. The system consists of a generator, a connect box for catheter cable plug in and the IVY Cardiac Monitor (IVY Biomedical Systems Inc., Branford, CT, USA) and is intended to treat AF. Several established focal ablation catheters of different manufacturers (Abbott, Biosense Webster, Boston Scientific) that are in use for RF ablation can be combined with the generator. The connect box allows visualization of the catheter in electro-anatomical 3D mapping systems to guide the procedure. Thus, aside from the energy applied, the workflow is not significantly different as compared to point-by-point RF ablation. Within the waveform optimization process, the company developed different ampere settings instead of voltage settings. The total target current to be achieved during one application can be selected by the user between 19, 22 and 25 amperes. A customized impedance dependent algorithm continuously adapts the waveform (of usually 3 pulses) and the number of bursts during an application to achieve the default ampere setting. Energy application in form of biphasic, monopolar pulsed electric fields is performed by pressing a foot switch. Once pressed, energy is delivered synchronized to the patient’s heartbeat over several seconds. Energy delivery will be automatically stopped by the generator after completion of the ablation cycle (delineated by an Energy Progress Bar on the generator and a signal tone) or in case of too low or too high impedance measurements. After pressing the foot switch, catheter visualization and contact force measurements are not available for at least 10 seconds from our experience. The company currently recommends a target contact force of 7.5–20 grams and 22 A for ablation at the posterior segment and 25 A for ablation at the anterior segment of the wide antral ablation line during PVI. A 20% overlap of the ablation points should be ensured since the border zone of the ablated tissue can be subject to reversible electroporation and thus reconnection can occur. In left atrial posterior wall isolation using single tip PFA, scar regression was infrequently seen.71) However, lesion regression of PV antral isolation was not observed after PFA using the multi-electrode basket/flower catheter.72) The irrigation flow rate during idle, as well as ablation, is 4 mL/min. First preliminary results of the unpublished pivotal ECLIPSE-AF trial (NCT04523545) for PVI in patients with paroxysmal or persistent AF convince without adverse events associated with PFA (no esophageal or phrenic nerve injury, no PV stenosis, no microbubbles in echocardiogram during ablation) and a high durability of PVI with different ablation catheters (84–92% at 3 months). The SPACE AF trial (NCT04652778) will add further data on the performance and safety of the CENTAURITM system in PVI procedures. Initial experiences with acute results are available as an abstract. In 12 patients having received PVI and posterior wall isolation, the authors demonstrated acute ablation success and no adverse events were observed. Energy was set to 25 A in most patients (68%) and 22 A in 32%, respectively. The estimated study completion date for both trials is April 2023. An interesting study in porcine ventricles pointed out that dose titration results in different lesion depths, e.g., the 25 A setting created the deepest lesion (8.2 mm),73) which allows dose adaptation for different wall thicknesses of the heart and tailor ablation therapy even for indications beyond PVI. Figures 5 and 6 show the CENTAURITM generator and a PVI procedure guided by 3D electroanatomical mapping.
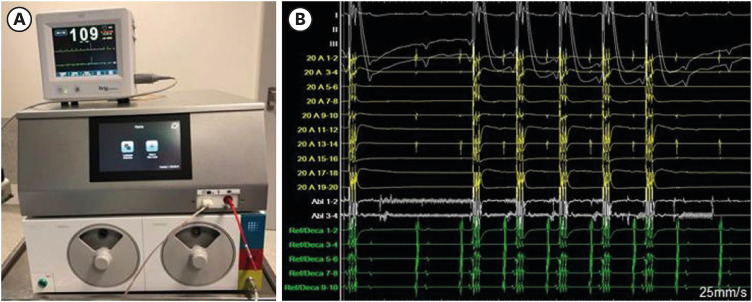 | Figure 5CENTAURITM generator with compatible monitor and pulsed electric field application. (A) Monitor for ECG-triggering (top), CENTAURITM generator (middle) with round connector boxes (bottom) for single-tip ablation catheters and integration in 3-dimensional electroanatomical mapping systems. (B) Electrograms during single-tip pulsed electric field application (top white: surface ECG, yellow: pentaspline mapping catheter positioned in contralateral pulmonary vein during ablation, lower white: single-tip ablation catheter, green: coronary sinus catheter).ECG = electrocardiogram.
|
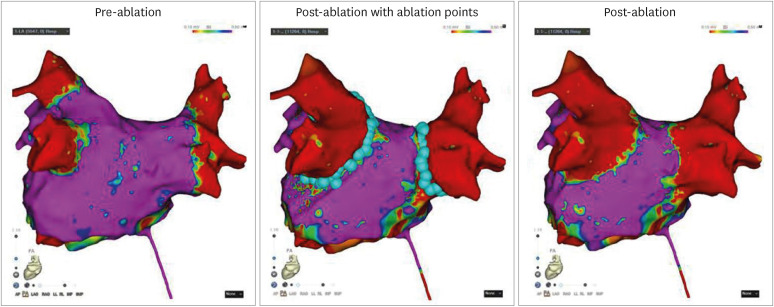 | Figure 6Voltage maps in the setting of PVI using single-tip PFA. Pre- and post-ablation voltage maps in the context of a single-tip PVI using the CENTAURITM generator for PFA. The connector box was used for the connection with the CARTO®3 electroanatomical mapping system. Shown are voltage maps generated with the PENTARAYTM mapping catheter (Biosense Webster, Diamond Bar, USA) in a posterior-anterior projection. Voltage settings were 0.10–0.50 mV. Ablation was performed with a THERMOCOOL SMARTTOUCHTM catheter (Biosense Webster, Diamond Bar, CA, USA). Left: pre-ablation voltage map. Middle: post-ablation voltage map with PFA points bilateral around PVs. Right: post-ablation voltage map demonstrating bilateral PVI.PFA = pulsed field ablation; PV = pulmonary vein; PVI = pulmonary vein isolation.
|
PulseSelectTM system
The PulseSelectTM system (Medtronic, Inc., Dublin, Ireland) is under clinical investigation and not yet commercially available. The generator delivers a biphasic, bipolar waveform over an over-the-wire 9F ablation catheter like the PVAC GOLD catheter. The circular catheter incorporates 9 gold electrodes and allows additional electrogram acquisition, pacing and measurements of temperature changes up to 1 second after energy delivery. The system is equipped with several proprietary pulsed electric field profiles with voltages ranging from 500 to 1,500 V.74) Due to the electrode arrangement, catheter rotation is required for successful circumferential PVI. According to the protocol, 4 series of energy applications are delivered in each catheter position. Initially, a low pulse is applied allowing repositioning in case of phrenic nerve capture. The first-in-human PULSED AF pilot trial investigated the system in 38 PVI procedures. The authors demonstrated 100% acute PVI without any serious adverse events, such as phrenic nerve palsy, esophageal lesions, or stroke. Left atrial dwell time was 82±35 minutes. A temperature rise of 2 degrees was observed at the electrodes, but no rise in esophageal temperature monitoring was noted in a subset of patients.74)
VARIPULSETM catheter, TRUPULSETM generator
This ablation system is under clinical investigation and not yet commercially available. It consists of the novel circular VARIPULSETM ablation catheter, comparable to a “Lasso” catheter, and is combined with the TRUPULSETM PFA generator, both compatible with the CARTO®3 electroanatomical mapping system (Biosense Webster, Inc., Irvine, CA, USA). The 7.5F over-the-wire ablation catheter is provided with 10 electrodes with individual irrigation pores, is bidirectionally deflectable and can be adjusted between 25 and 35 mm in diameter, which facilitates catheter maneuvering and allows adaptation to fit different PV ostial anatomies. For each PFA application the generator produces trains of microsecond-range bipolar pulses with 1,800 V that are applied between adjacent and every other electrode over a total of approximately 250 microseconds (4 mL/min continuous irrigation flow rate).75) In an animal study, the system produced durable atrial lesions and did not show esophageal or phrenic nerve damage.75) The ongoing inspIRE trial (NCT04524364) is the first in-human study investigating the ablation system for paroxysmal AF ablation.
AFFERA system in combination with radiofrequency energy
The system is under clinical investigation and not yet commercially available. The AFFERA system utilizes a dual-generator (HexaGen and HexaPulse, respectively) allowing to switch between RF and pulsed electric field applications that are delivered through a lattice-basket tip ablation catheter (Sphere-9) designed to create large focal lesions. The catheter is visualized in an electroanatomical mapping system (HexaMap, Prism-1; Affera, Inc., Watertown, MA, USA). The 7.5F ablation catheter is bidirectionally steerable and has a spherical surface with an expandable 9-mm diameter lattice electrode that contains 9 mini-electrodes of 0.9 mm each and a center electrode. Tissue-catheter contact is based on impedance measurements between each mini-electrode and the center electrode.76) The programmable PFA generator generates trains of biphasic, microsecond-scale pulses over 3 to 5 seconds to deliver a total current between 24 A and 32 A through the ablation catheter without synchronization to P-wave or QRS complexes.77) In a first-in-human trial, a total of 76 patients underwent PVI with either a combination of PFA and RF or PFA only, respectively. A subset of patients received additional ablation of the mitral and cavotricuspid isthmus or left atrial roof lines. 99.2% of PV could be isolated, and all additional ablations were entirely successful using the Sphere-9 ablation catheter. Reddy and colleagues reported that both approaches could be safely and efficiently performed. PVI itself (first to last ablation) took 22.6±8.3 minutes. No device related complications occurred. However, in 2 patients of the PFA/RF group, minor esophageal injuries were noted. Silent cardiac magnetic resonance imaging (cMRI) positive cerebral lesions were verified in 5.9% of patients. The authors conclude that all these patients had an initial ACT below the target range and that a careful ACT monitoring could minimize events. Only recently, the Sphere-9 catheter was used in healed infarcted ventricular myocardium in a swine model. The authors concluded that PFA in ventricular scar areas may be advantageous over RF ablation producing lesions that are not limited to the subendocardium and eliminate viable myocardium in between collagen and fat.78)
The manufacturer has recently designed a single shot PFA catheter for PVI, the SpherePVITM catheter. The 7.5F over-the-wire lattice basket catheter is expandable to 34 mm and has proven fast and durable PVI in a first animal study.79)
Pulsed field cryoablation using the CryoPulseTM catheter
The system offers the opportunity of a combination of initial 30 seconds ultra-low temperature cryoablation followed by pulsed electric field applications using the same ablation catheter. The CryoPulseTM ablation catheter (8.5F, 20 pole non-deflectable, central lumen for round stylet to create circular configuration, steerable sheath for navigation), the proprietary PFA console and the iCLASTM cryoablation console (Adagio Medical, Inc., Laguna Hills, CA, USA) complete the system. In a pre-clinical animal study, Verma and colleagues demonstrated feasibility of pulsed field cryoablation showing a more favorable thermal profile without muscle contractions or microbubbles while extending lesion depth as compared to PFA alone in an overall feasible and safe procedure. The generator delivered high-voltage, biphasic, bipolar pulsed electric fields of at least 1,100 V over multiple channels.80) However, in this study, only a single PFA train was delivered, which is significantly different to other PFA protocols with multiple trains that can as well be adjusted to eliminate microbubbles or muscle stimulation. Nevertheless, the combined energies might have summative effects on lesion formation and the freeze can improve tissue-catheter contact throughout the entire ablation application. First clinical results of the PARALLEL trial (NCT05408754) comparing PFA alone vs. pulsed field cryoablation in persistent AF patients are awaited.
Utrecht university custom pulsed field ablation catheter
Loh et al.81) reported about a single pulse IRE ablation using a custom 8F non-deflectable 14-polar circular IRE ablation catheter with a variable hoop diameter (16–27 mm). A deflectable sheath was used to maneuver the catheter. The IRE catheter was connected to an external defibrillator to deliver single, R-wave triggered, monophasic IRE pulse (6 ms, 200 J). Two patches on the lower back of the patient were used as indifferent electrodes. All PVs of 10 patients could be successfully isolated and no acute device related complications occurred.
AccuPulse system
The AccuPulse system consists of the AccuBlator generator, the AccuPulse catheter and the AcQMap® (Acutus Medical, Inc., Carlsbad, CA, USA) high-resolution mapping system that gathers anatomical information via ultra-fast ultrasound and allows non-contact mapping of electrical activity. The PFA catheter is currently a prototype investigational device.
AtriAN epicardial electroporation system
The ablation of ganglionated plexi as an additional interventional treatment option can be beneficial in AF patients.82) The AtriAN epicardial electroporation system (AtriAN Medical, Galway, Ireland) was designed for cardioneuronal ablation in the treatment of AF. The system consists of a generator delivering monopolar, monophasic pulses, and a specific focal catheter or glove catheter that are inserted through a subxiphoidal access to target ganglionated plexi and neurons without affecting the myocardium. After initially investigating DC applications in the epicardial ablation of ganglionated plexi,83) a pre-clinical proof-of-concept study showed safe, effective ganglionated plexi ablation with minimal collateral damage in a canine model.84) The Neural-AF trial (NCT04775264) currently assesses feasibility and safety of atrial deganglionation as an adjunctive therapy for AF in a first in human investigation.
Go to :
PULSED FIELD ABLATION: EFFICACY, SAFETY, AND FIELDS OF APPLICATION IN CLINICAL STUDIES
Since market release in Europe in January 2021 (FARAPULSETM) and August 2022 (CENTAURITM), limited data of clinical studies have been published and no randomized controlled trials are available. Most data were derived from the FARAPULSETM ablation system. So far, PFA is approved for AF ablation, e.g., PVI, but several other targets have been addressed as an off-label use. The ongoing randomized BEAT PAROX-AF trial (NCT05159492) comparing PFA vs. contact force RF ablation and the ADVENT trial (NCT04612244; PFA vs. contact force RF vs. cryoballoon ablation) will give important additional information for the future direction of the interventional treatment of AF. Comparisons to novel technologies, such as very high-power short duration RF ablation or ultra-low temperature cryoablation can be of particular interest to determine the optimal strategy regarding a time-efficient and effective ablation without compromising safety. The following section will give a summary of the currently available clinical studies.
Pulsed field ablation to treat atrial fibrillation
The safety and feasibility studies of Reddy and colleagues, IMPULSE,15) PEFCAT15) and PEFCAT II were the first reporting on PFA for paroxysmal AF in clinical trials.26) In total, 121 patients received fluoroscopy guided PVI with the single-shot FARAPULSETM system. Acute PVI was achieved in 100% independently of the waveform applied.26) In a remap analysis of the above trials, the importance of an optimal pulsed electric field protocol became obvious. Durable PVI was documented in 96% of PVs (84% of patients) in subjects who were treated with an optimized biphasic waveform that was developed during the study course, whereas PVs of patients who were treated with the initial monophasic waveform showed durable PVI in only 45% (18% of patients).26) Others confirmed the advantage of the novel waveform in patients who necessitated redo procedure after initial PFA-PVI: solely 9.1% of PV showed reconnection.85) Additional works reported that the chronic antral lesion size created with PFA (pentaspline catheter) persists over time72) and is comparable to the ones with RF, cryo- or laserballoon ablations.86) Interestingly, in an MRI study, most of the large late gadolinium enhancement (LGE) lesions acutely induced by PFA disappeared over time, whereas those persisted after RF- or cryoablation, e.g., caused chronic fibrosis. The authors concluded that in PFA this process may contribute to preserved tissue compliance and can prevent myocardial stiffness.87)
At 1 year, freedom from any atrial arrhythmias of the IMPULSE, PEFCAT and PEFCAT II trials was 78.5% for the entire cohort and 84.5% for patients having received PFA with the optimized waveform, respectively. The procedure showed a favorable safety profile with common adverse events (2.5%) associated with catheter ablation. No adverse events possibly related to the energy source were registered.26)
The MANIFEST-PF survey reports on the real-world outcomes of PFA for PVI in a typical cohort of a total of 1,758 patients with paroxysmal or persistent AF treated in 24 high-volume electrophysiology centers across Europe.27) PVI was achieved in 99.9%. The mean procedure time was 65 minutes including pre- and post-ablation mapping being performed in a subset of patients. The mean radiation time was 13.7 minutes. The overall adverse event rate with 1.6% major and 3.9% minor complications was comparable to conventional thermal energy sources. However, several complications seem meanwhile to be preventable. Several tamponades were related to a straight extra-stiff guide wire that was initially recommended to guide catheter positioning but lead to perforations and subsequently to tamponades. After utilization of a J-tip guide wire, no further tamponades were observed for this reason. Other tamponades resulted from repositioning of the CS catheter to perform RV back-up pacing in cases of transient asystole following PFA delivery. Asystole after the first PFA of left PVs was also observed by our group in 33% of cases.88) After administration of atropine before the first energy delivery, no more need for back-up pacing was reported. Cerebral events were explained by suboptimal catheter/sheath management in most cases. Specific adverse events possibly related to PFA itself, however, were sparse. No esophageal lesions, PV stenosis or phrenic nerve paralysis were noted. Transient phrenic nerve palsy accounted for 0.46% and completely recovered in all patients before discharge.27) This might be explained by recent findings of Avazzadeh et al.89) In contrast to previous studies, they observed a similar susceptibility of cardiac cells and neurons after exposure to electroporation,89) which should be incentive for further studies. Some patients underwent additional mitral isthmus PFA with one patient developing coronary artery spasm, which was successfully treated with intracoronary nitroglycerin.27) Other clinical studies reported similar data all highlighting the acute efficiency, short procedure time, beneficial safety profile and favorable rate of clinical outcomes up to 1 year follow-up.88)90)91)
Distinct reports on the safety profile of PFA in humans have been published. In a comparative analysis of PFA and RF-ablation, PV narrowing or stenosis did not occur following any PFA procedure, but in 12.0% and 32.5% of RF ablations, respectively.92) Others investigated esophageal and aortic lesions with LGE-MRI. Acute esophageal lesions did not occur in patients with PFA (0%) but in 43% after thermal ablations (RF- and cryoablation; p<0.001) and acute aortic injuries were found in 33% (PFA) and 43% (thermal energies; p=not significant), respectively. However, none of the patients showed clinical complications and all esophageal and aortic LGE resolved at 3 months follow-up MRI.93) To date, lesions of the descending aorta are of unclear significance but should be considered in patients receiving PVI, or posterior wall isolation with PFA or thermal ablation.
The vasospastic potential of PFA has already been described in animal studies.66) Reddy et al.94) performed coronary angiography concomitantly to PFA (FARAPULSETM system) and routinely observed subclinical, yet often severe coronary artery spasms during applications in proximity to coronary arteries, e.g., cavotricuspid and mitral isthmus ablation. The authors recommended to consider prior intravenous nitroglycerin administration before PFA. In case of ST-segment elevation immediate coronary angiography should be performed followed by intracoronary nitroglycerin administration and additional oral nitroglycerin was suggested for several days to prevent recurrent spasms.94) Another patient developed ventricular fibrillation after severe coronary spasm with ST-segment elevation following PFA of the cavotricuspid isthmus .95) Coronary artery spasms during PVI or left atrial posterior wall isolation have not been observed in this study,94) but should be kept in mind as a possible, but assumingly infrequent event.
Our group concluded that PFA seems to be a safe ablation modality for the brain by reporting a low rate of silent cerebral events (3%, 1/30 patients) in cMRI performed after PFA for PVI. The lesion of unknown origin completely resolved during follow-up.96) Chen et al.97) recently reported in a pilot cohort study that PFA in patients with implantable electronic devices (n=20) appears to be feasible and safe under the guidance of a systematic approach. The lack of esophageal affections, PV stenosis, rare events of transient phrenic nerve palsies or others reported after PFA is in line with preclinical studies and highlights the overall favorable safety profile of the technology.
Go to :
FIRST CLINICAL EXPERIENCES BEYOND PULMONARY VEIN ISOLATION
PFA has been investigated as an off-label approach beyond PVI. Promising initial experiences have been described but need to be proven in larger comparative studies. PVI using the FARAPULSE system is guided by fluoroscopy, but integration in a 3D electroanatomical mapping system for complex continuous lesion sets should be supported to verify optimal catheter placement. The visualization of the catheter is impedance-based and offers accurate identification in 2 established mapping systems. In flower position, feasibility was demonstrated for the creation of posterior LA wall isolation, roof lines, anterior lines, or mitral isthmus lines in very small cohorts.20)21)22) However, Kueffer et al.22) mentioned that additional RF-ablation was necessary in some cases to achieve bidirectional block of the anterior line and the mitral isthmus and stated that a focal ablation catheter might be more suitable for these indications, which is already possible as an off-label approach using the Galaxy generator in combination with conventional focal ablation catheters. In the PEFCAT II trial, successful PFA of the cavotricuspid isthmus was achieved by a focal ablation catheter in 4 patients.26) It remains to be seen if the risk of vasospasm can be reduced using a single-tip PFA catheter for ablations in proximity to coronary arteries. Other successful PFA applications in right atrial tachycardias have been described in case reports.98)99)
Go to :
CONCLUSIONS AND FUTURE PERSPECTIVES
PFA is an emerging technology in interventional electrophysiology. First clinical data in AF ablation show excellent efficacy and a favorable safety profile in a time-efficient procedure. Due to these promising results, PFA is growing to become a valuable alternative to established treatment modalities, such as RF- or cryoablation. However, randomized studies comparing PFA to standard-of-care including extended follow-up data on the clinical success and lesion durability, and particularly the safety profile that is expected to be superior for PFA are awaited to determine the optimal treatment strategy to perform PVI. Further pre-clinical data and data of PFA in off-label indications have added favorable first results to the literature and promise extended indications of PFA applications for atrial tachycardias, ventricular arrhythmias, within the CS or epicardial ablations including ganglionated plexi ablations. PFA in areas close to the coronary arteries100) does not seem to be associated with structural artery damage (which is a limitation for standard treatment), but severe vasospasm was frequently reported making preventive measures and/or modifications of electroporation protocols mandatory. Furthermore, it must be seen, if other PFA systems might be more suitable for ablations adjacent to coronary arteries. Several PFA systems with different catheters that have just recently been market-approved in Europe or are currently under preclinical investigation will add unique opportunities to treat arrhythmias. Fully visualization in 3D electroanatomical mapping systems should be enabled to optimize the treatment and reduce radiation exposure. Nevertheless, one must be aware that the technology is in its infancy in the field of cardiac arrhythmias. The distinct mechanisms of electroporation on a cellular basis are not yet fully understood and might reveal new opportunities or better control in the future.101) Additionally, it is unknown whether one or another IRE protocol or ablation system is superior to another and, different protocols of the systems hamper comparability, e.g., the results are not transferable. Furthermore, it is unclear whether the same protocol can be applied for different indications (e.g., in atria or the ventricles) or in how far and to which extent dose adaptations will be necessary for successful ablation while avoiding collateral damage.
Go to :
 XML Download
XML Download