

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Donor shortage for heart transplantation (HTx) is a global phenomenon, including South Korea.1)2) As of 2020, only 174 of 774 (22.5%) waitlisted patients have received donor hearts.3) Even in status 0 patients with the highest priority, defined as receiving an extracorporeal membrane oxygenation (ECMO) or mechanical ventilator defined by the Korean Network for Organ Sharing, only 40–60% were allocated with donor hearts.4) This implies that lower priority patients in South Korea do not have a legitimate chance of receiving a heart until mechanical circulatory support is necessary. The high waitlist mortality rate of 15% may indeed be related to donor shortages in South Korea.
There are numerous ways to expand the donor pool: improvement of the conception through nationwide organ donation campaigns, modification of the law and system on organ donation as France, modification of the definition of brain death, or utilization of donors after circulatory death by the organ care system.5) However, these systematic changes are extremely challenging, for its time-consuming logistics and the necessity of astronomical figures of budget. Clinicians must accordingly devise rapid solutions within the system to save lives. Use of donor hearts classified as “marginal,” which has been conventionally abandoned, can be a practical way to expand the donor pool.
A marginal donor (MD) is one with medical conditions not optimal for organ donation which may be related with poor post-transplantation outcomes. A significant numbers of donor hearts have been abandoned for their marginality, especially in South Korea: donor heart utilization rate is 30–40%.6) However, we question whether such donors were truly marginal and doomed to translate into poor outcomes. Herein, we report outcomes of HTx using MD hearts.
METHODS
Ethical statement
The study was approved by the Institutional Review Board of the Pusan National University Yangsan Hospital (05-2021-209). The requirement for informed consent was waived owing to the retrospective nature of the study.
Study design and population
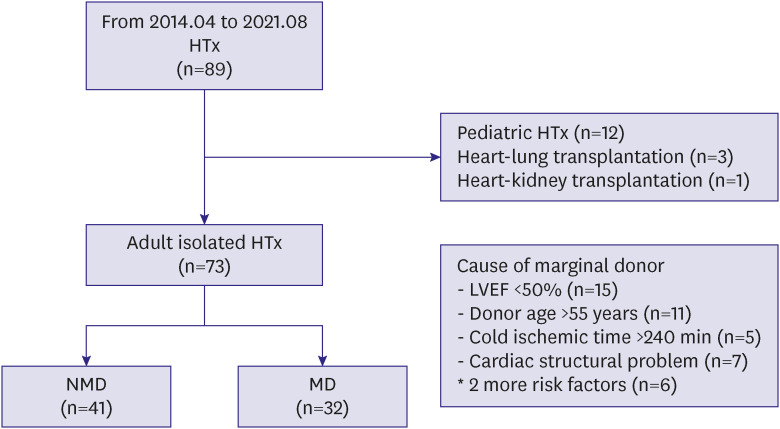
This retrospective observational study included patients who underwent HTx at a single center between June 2014 and March 2021. All data were collected from an institutional prospective surgical database and electronic charts. During the study period, 89 patients underwent HTx at a single institution. Of these, 77 (86.5%) cases of HTx were conducted in adult recipients, and 73 patients were included in present study after excluding four multiorgan transplantation cases. MD was defined as based on the following criteria: donor age >55 years, left ventricular ejection fraction (LVEF) <50% on preoperative echocardiography, cold ischemic time >240 minutes, or significant cardiac structural problems on any imaging study. Thirty-two (43.8%) recipients were classified into the MD group, and the remaining 41 (56.2%) were included in the non-marginal donor (NMD) group (Figure 1).
Figure 1
Inclusion criteria and classification of each group by definition of marginal donor.
HTx = heart transplant; LVEF = left ventricular ejection fraction; MD = marginal donor; NMD = non-marginal donor.
The primary and secondary endpoints were mortality and primary graft dysfunction (PGD), respectively. The definition of PGD was any graft dysfunction that occurs within 24 hours of HTx, and complies with the International Society for Heart and Lung Transplantation (ISHLT) meeting in 2014 (Supplementary Table 1).7) Graft function after HTx was evaluated based on vasoactive inotropic score (VIS). VIS was derived from summing of inotropic dose rates: Dopamine Dose (μg/kg/min) + Dobutamine Dose (μg/kg/min) + 100 × Epinephrine Dose (μg/kg/min) + 10 × Milrinone Dose (μg/kg/min) + 10,000 × Vasopressin Dose (unit/kg/min) + 100 × Norepinephrine Dose (μg/kg/min).
Additionally, to quantify preoperative recipient risk, we employed the Index for Mortality Prediction after Cardiac Transplantation (IMPACT) score.8)9) The details of IMPACT score ere described in Supplementary Table 2.
Surgical procedures
We performed a conventional median sternotomy with selective vena caval cannulation for HTx. Inferior vena cava was drained cannulation via the femoral vein access. A recipient who underwent preoperative ECMO was converted to cardiopulmonary bypass (CPB) using existing cannulas. In such cases, cannulation of the superior vena cava was performed before aortic cross clamping (ACC). For patients who did not receive ECMO, arterial cannulation was routinely performed in the distal aorta. To minimize the CPB time, the heart of the recipient was explanted just before the donor heart arrived. Donor hearts were protected with infusion of a 4°C HTK solution (Custodiol®; Köhler Chemie GmbH, Bensheim, Germany) for 8 minutes before harvesting. The harvested heart was washed with the HTK solution and transported using an ice package. The standard bicaval anastomosis technique was routinely performed.
Management in the intensive care unit during the early period
A Swan-Ganz catheter was inserted in the operating room. All patients were transferred to the cardiac intensive care unit (ICU) after surgery. The postoperative target ranges of the monitoring indicators were as follows: cardiac output, 4–7 L/min; target heart rate, 95–110 beats/min; pulmonary capillary wedge pressure (PCWP), 15–20 mmHg; central venous pressure, <15 mmHg; <1/3 of pulmonary arterial pressure over systemic arterial pressure; lactate level, <2.0 mmol/L; mixed venous oxygen, >70 mmHg; pulmonary partial pressure of oxygen, > 100 mmHg; urine output >100 mL/hr; and potassium level >4.0 mmEq. Low dose dobutamine and norepinephrine were the most frequently used agents to maintain vital signs. If the patient’s demand for inotropes increased and isolated pulmonary arterial hypertension was detected, milrinone was given, and if decreased systemic vascular resistance was detected with norepinephrine demand >0.2 mcg/kg/min, vasopressin was administered. Isoproterenol was used to achieve the target heart rate in cases of poor response to chronotropic drugs or complete atrioventricular block, and temporary or epicardial pacing was applied. After confirming consciousness and controlled bleeding, the patients were extubated. They were sent to the general ward from 3 days after the operation according to their medical conditions. Cardiac rehabilitation was started after chest tube removal and continued until discharge.
Immunosuppression protocol
An anti-interleukin-2 receptor monoclonal antibody (basiliximab) was used for induction from June 2014 to July 2018. Antithymoglobulin (rabbit) was replaced with basiliximab from August 2018. However, in cases of recipients older than 65 years of age or those with a high risk of infection, induction therapy was omitted. A bolus of 500 mg of methylprednisolone was administered when allograft left atrial anastomosis was initiated. The initial postoperative dose of prednisolone for maintenance therapy was 1 mg/kg/day, which was tapered to 0.25 mg/kg/day at 1 month and then to 2.5–5 mg/day at 1 year. Prednisolone was discontinued at approximately 1 year after HTx, except in the patients who experienced any type of rejection. Maintenance immunosuppression consisted of tacrolimus, mycophenolate mofetil (500–1,000 mg), and corticosteroids. Twelve months postoperatively, tacrolimus and everolimus, with or without prednisolone, were administered. In cases of cross-matching positive transplantation, pre-/post-desensitization with plasma pheresis and intravenous immunoglobulin (total, 1 mg/kg for 3 days) were administered. Rituximab, with or without bortezomib, was used to prevent antibody-mediated rejection.
Statistical analysis
Variables were summarized by frequency and percentage for categorical data and mean ± standard deviation and median (range) for numeric data. Group differences were tested using the χ2 test or Fisher’s exact for categorical data and independent t-test or Mann-Whitney U test for numeric data as appropriate. To check if its distribution is normal, we used Shapiro-Wilk’s test.
Univariate and multivariate logistic regression analysis were performed to identify prognostic factors which are independently related to event. Due to the small number of deaths, risk factor analysis for the primary endpoint has been judged to be inappropriate and was not described. Instead, risk factor analysis was performed on the PGD, a secondary endpoint. Variables for analysis were selected as factors considered clinically meaningful, including MD. And variables known as risk factors in previous reports were also included.7)10) Variables that were too small to be suitable for analysis were excluded (such as race, weight mismatch ≥30%, etc.) To check the multicollinearity problem, the variance inflation factor (VIF) was also estimated. VIF quantifies the severity of multicollinearity in regression analysis and VIF less than 10 indicated that there was no problematic multicollinearity among the independent variables (VIF <10).
Overall survival and PGD-free survival were estimated using Kaplan-Meier curve. Survival curves were compared between groups using the log-rank test. Univariate and multivariate analyses, using Cox proportional hazard regression analysis, were performed to identify prognostic factors which are independently related to time to event (death or PGD).
Considering the nature of the repeated measured data of echocardiography (LVEF), a generalized linear mixed model (GLMM) with random intercepts was used to fit a model. The GLMM model included repeated measures of numeric variables as dependent variables; group, time, and group × time interaction as fixed effects; and subject as a random effect. To avoid making any assumptions about the covariance structure, we used an unstructured covariance matrix that was allowed to differ across groups for the GLMM analysis.
All statistical analyses were carried out using SPSS 26.0 statistical software (IBM Corp. Released 2019, IBM SPSS Statistics for Windows, version 26.0; IBM Corp., Armonk, NY, USA) and R statistical software (version 3.4.0; R Foundation, Vienna, Austria, http://www.r-project.org/). The p values less than 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
Donors in the MD group were older than those in the NMD group. LVEF was significantly lower in the MD group (Table 1). Twenty-five percent of patients in the MD group were rejected more than 5 times by other hospitals with a higher HTx allocation priority. Sex and medical history were not significantly different between the two groups. However, the rates of preoperative ECMO and ICU admission, the degree of emergency were higher in the NMD group. Although the preoperative creatinine level was higher in the NMD group than in the MD group, other laboratory results were comparable between the groups. Donor and recipient characteristics are described in detail in Table 1.
Table 1
Preoperative characteristics of donor and recipient
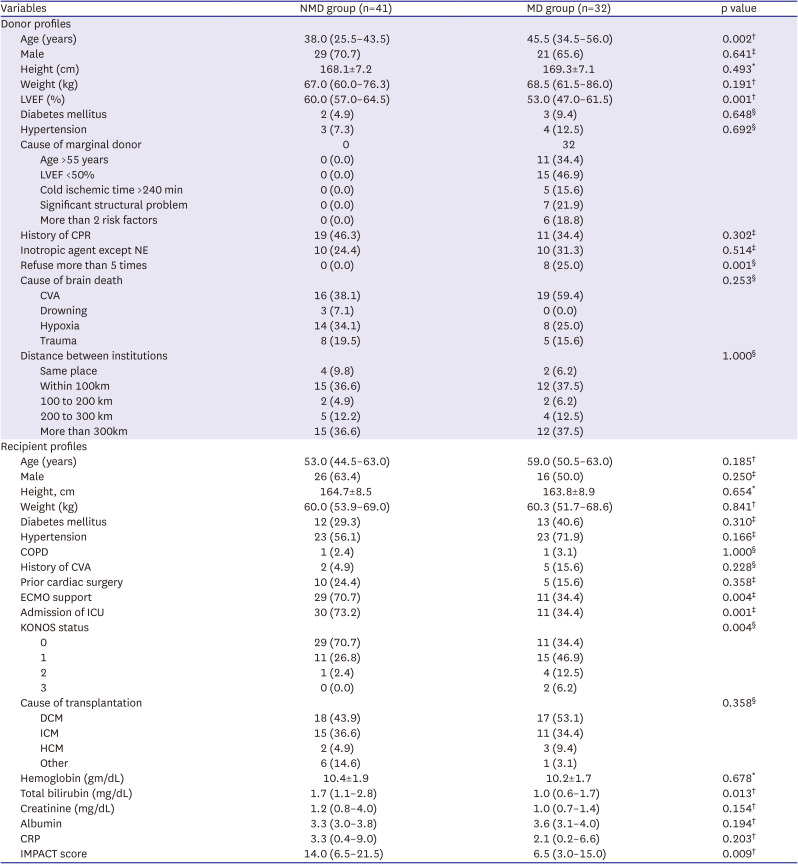
Values are presented as number (%), mean ± standard deviations, or median (interquartile range).
COPD = chronic obstruction pulmonary disease; CPR = cardiopulmonary resuscitation; CRP = C-reactive protein; CVA = cerebrovascular accident; DCM = dilated cardiomyopathy; ECMO = extracorporeal membrane oxygenation; HCM = hypertrophic cardiomyopathy; ICM = ischemic cardiomyopathy; ICU = intensive care unit; IMPACT = The Index for Mortality Prediction After Cardiac Transplantation; KONOS = Korean Network for Organ Sharing; LVEF = left ventricular ejection fraction; MD = marginal donor; NE = norepinephrine; NMD = non-marginal donor.
*p values were derived from independent t-test. †p values were derived from Mann-Whitney’s U test. ‡p values were derived from χ2 test. §p values were derived from Fisher’s exact test. Shapiro-Wilk’s test was employed for test of normality assumption.
Perioperative clinical results
Cold ischemic and total ischemic times were numerically longer in the MD group. The ACC and CPB times in the recipients were also similar. There was one case of early mortality in each group. The incidence of other adverse events during the perioperative period between the groups. The surgical and perioperative details are presented in Table 2.
Table 2
Surgical and perioperative profiles
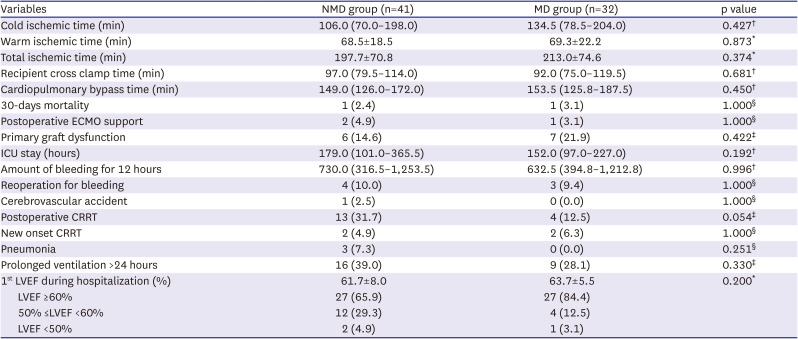
Values are presented as number (%), mean ± standard deviations, or median (interquartile range).
CRRT = continuous renal replacement therapy; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; LVEF = left ventricular ejection fraction; MD = marginal donor; NMD = non-marginal donor.
*p values were derived from independent t-test. †p values were derived from Mann-Whitney’s U test. ‡p values were derived from χ2 test. §p values were derived from Fisher’s exact test. Shapiro-Wilk’s test was employed for test of normality assumption.
Immediate postoperative, 30-day, and long-term clinical results
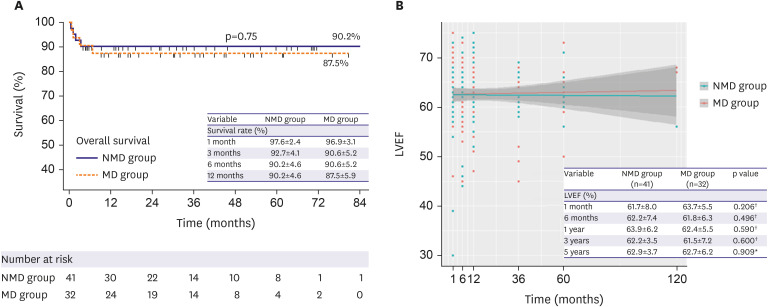
Immediate postoperative creatine kinase-MB isoenzyme levels were similar between the two groups, and vasoactive inotropic scores were not different within 24 hours (Figure 2A). The cardiac index showed a slightly lower trend in the MD group compared to the NMD group without a statistical difference immediately postoperatively; however, it became similar between groups after 24 hours (Figure 2B). Moderate or higher grade PGD developed in 13 (17.8%) patients during the perioperative period, and there was no difference in the incidence of PGD between the groups. On the first echocardiography performed 1 week postoperatively, there was no difference in the LVEF between groups (Table 2). The 30-day and 1-year survival rates were 97.6±2.4% and 90.2±4.6% in the NMD group and 96.9±3.0% and 87.5±5.9% in the MD group (p=0.87, 0.73 respectively). There was no difference in the long-term mortality rate between groups: 12.5% vs. 9.8% in MD vs. NMD during follow up (mean 26.3±24.6 vs. 29.1±17.6 months, p=0.75; Figure 3A). The LVEF on serial echocardiography showed no difference between 2 groups during long-term follow-up (Figure 3B).
Figure 2
Trend of postoperative vasoactive inotropic scores and cardiac index in each group.
(A) Vasoactive inotropic score of immediate, 6 hours and peak value within 24 hours post operation. (B) Serial cardiac index within 72 hours post operation.
MD = marginal donor; NMD = non-marginal donor.
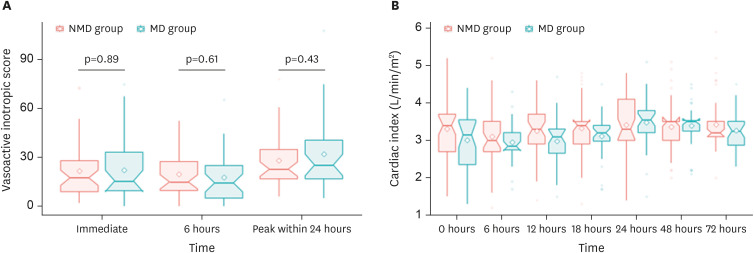
Figure 3
Overall survival and left ventricular function during follow up period.
(A) Overall long-term survival between groups. (B) Long-term follow-up LVEF between groups.
LVEF = left ventricular ejection fraction; MD = marginal donor; NMD = non-marginal donor.
*p values were derived from independent t-test. †p values were derived from the Mann-Whitney test. Shapiro-Wilk’s test was employed for the test of the normality assumption.
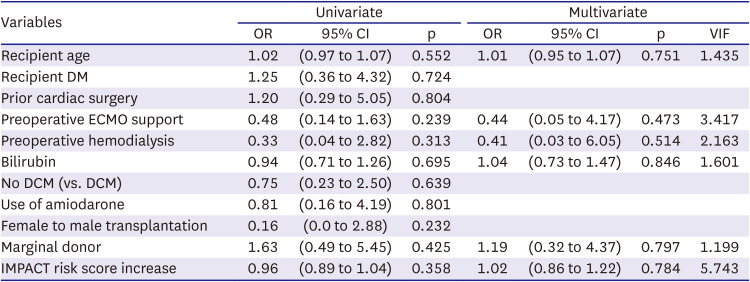
Risk factor analysis of primary graft dysfunction
In the multivariate logistic regression analysis for PGD, there were no meaningful predictors. MD hearts or IMPACT scores were not significant predictors of PGD. Logistic regression analysis failed to converge since there was no case of PGD in female to male transplantation. The detailed values of the univariate analysis are shown in Table 3.
Table 3
Risk factor analysis for primary graft dysfunction
Sub-group analysis: clinical impact of marginal donor according to recipient’s status
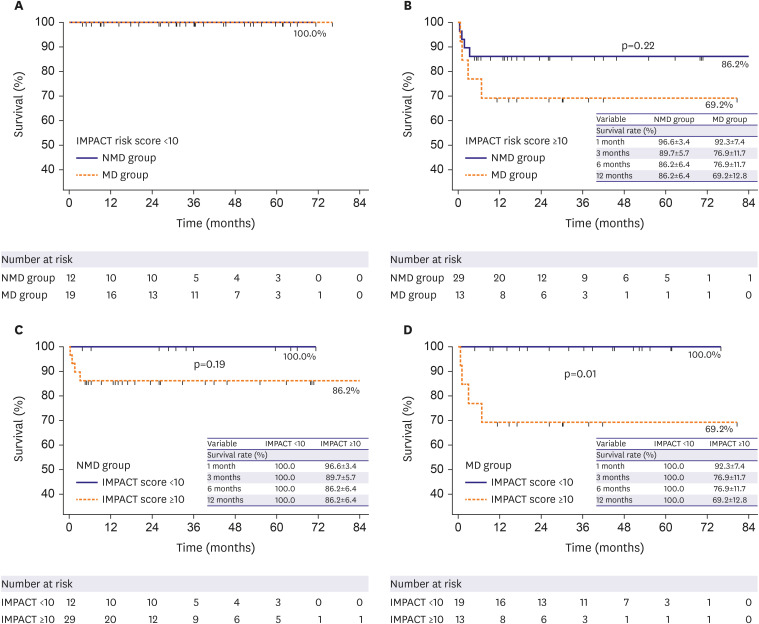
Of the MD group, 19 recipients (59.3%) were classified as low-risk groups (IMPACT Risk Score <10) and 13 as high-risk groups (IMPACT Risk Score ≥10). There was no difference in donor characteristics or surgical profiles between the low- and high-risk groups (Table 4). The high-risk group showed higher incidence of prolonged ICU stay (Table 4). Other clinical outcomes were not different between two groups. However, the low-risk group showed better long-term survival than high-risk group (Figure 4). Particularly, there was no mortality in low-risk group during follow-up regardless of donor’s marginality (Figure 4A). On the other hand, high-risk recipients transplanted with marginal donor showed lower survival during follow up period (Figure 4B). In the NMD group, recipient risk status did not affect the survival (low-risk vs. high-risk recipient group, 100% vs. 86.2%, p=0.19; Figure 4C). However, in the MD group, the survival was significantly different according to the recipient risk status (low-risk group vs. high-risk group, 100% vs. 69.2%, p=0.01; Figure 4D).
Table 4
Major outcomes according to risk stratification of recipient
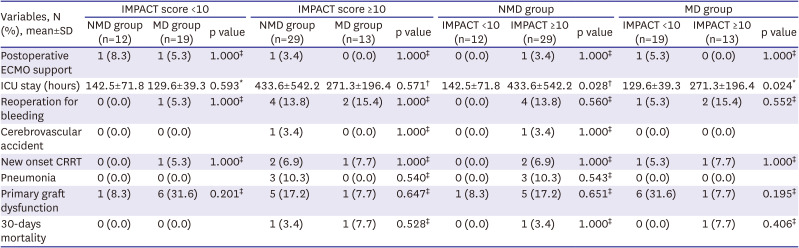
Values are presented as number (%) or mean ± standard deviations.
CRRT = continuous renal replacement therapy; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; IMPACT = Index for Mortality Prediction after Cardiac Transplantation; MD = marginal donor; NMD = non-marginal donor.
*p values were derived from independent t-test. †p values were derived from Mann-Whitney’s U test. ‡p values were derived from Fisher’s exact test. Shapiro-Wilk’s test was employed for test of normality assumption.
Figure 4
Kaplan–Meier survival curve by donor and recipient medical status.
(A) Survival rate in the low-risk recipient (IMPACT score <10) group. (B) Survival rate in the high-risk recipient (IMPACT score ≥10) group. (C) Survival rate in NMD group. (D) Survival rate in MD group.
IMPACT = Index for Mortality Prediction after Cardiac Transplantation; MD = marginal donor; NMD = non-marginal donor.
Characteristics of donors declined >5 times
Like other donor allocation programs, Korean Network for Organ Sharing (KONOS) re-allocates declined donor heart to the patient with highest priority among the remaining candidates. We collected the specific reasons for turning down donor hearts among candidates with higher priority than our patients. We considered that if a donor heart was declined more than 5 times by other candidates due to the ‘donor factor,’ it was discerned as a marginal donor by other institutions meaningfully. Supplementary Table 3 summarizes the characteristics and results of seven transplant cases utilizing donor hearts that were declined more than 5 times by other listed candidates. The specific reasons for ‘medical unsuitability’ of donor hearts were various, including old age (61 years), bradycardia, eccentric left ventricular (LV) hypertrophy, LVEF of 47% with regional wall motion abnormalities, right ventricular dysfunction (suspicious intracardiac right to left shunt), LVEF of 35% with global hypokinesia, and one case with an unidentifiable reason. In two donors whose donations were delayed for remnant electroencephalogram signals, the LVEF recovered to the normal range after transplantation. Donor #4, whose diastolic LV septal and posterior wall thicknesses exceeded 13 mm, required permanent pacemaker implantation for atrioventricular dyssynchrony despite 1 month of waiting for recovery after transplantation. Sinus rhythm was completely restored 2 weeks after permanent pacemaker insertion. All recipients had excellent 1-year survival rates.
DISCUSSION
In the present study, we compared the clinical outcomes MD and NMD hearts. Early outcomes including PGD, 30-day and long-term mortality were comparable between groups. Notably, the clinical status (emergency status) of the recipients of MD group was better. In addition, even the donor hearts declined by more than 5 candidates of higher priority on the waiting list showed excellent short- and long-term outcomes. To our knowledge, this is the first MD heart utilization report in South Korea.
Optimal donor characteristics are defined as age <55 years, absence of significant structural abnormalities (wall thickness >13 mm on echocardiography and significant valvular, congenital, and coronary artery disease), adequate physiologic function (LVEF >45%, mean arterial pressure >60 mmHg; PCWP, 8–12 mmHg), no inotrope dependence, acceptable donor-recipient body size (20–30% of height and weight), negative hepatitis C virus (HCV) antibody, hepatitis B surface antigen, and human immunodeficiency virus (HIV) serology, and absence of active malignancy.11) Although donors ineligible for these conditions may be classified as an MD, the specific criteria differ from one center to another, depending on the experiences of each center (Supplementary Table 4).12)13)14)15)16)17)18) In an effort to guide clinicians, an integrative scoring system was suggested based on UNOS data.19) Predictive risk models have been developed to optimize donor selection; however, they are not widely applicable or adopted in clinical practice.20)
Around 40% of our HTxs were performed by hearts that met the MD criteria (Supplementary Figure 1). Individual donor selection requires detailed review and repeated discussion within the transplant team. From the accumulation of our experience and data, the consensus within our multidisciplinary HTx team for donor selection principles are as follows: donor age ≤65 years with the difference of donor and recipient age less than five years, LVEF ≥40% with reversibility (e.g., prominent stress-induced cardiomyopathy features in echocardiogram or documented improvement with serial follow-up echocardiogram), cold ischemic time >240 minutes without risk factors, structural heart disease that can be easily corrected or controllable with medical therapy and negative HCV and HIV serology. However, we would like to stress out “donor-recipient coupling” when considering utilization of MD from our experiences. As shown in Figure 4, low-risk recipients (IMPACT score <10) had excellent long-term outcome despite utilizing MD hearts. High-risk recipients (IMPACT score ≥10) matched with MD showed worst outcome. Based on such findings, our multidisciplinary HTx team no longer receive MD hearts in high-risk recipients.
The most frequently encountered medical conditions for MD in our study were old age and LV dysfunction. The ISHLT stresses the importance of donor age as an important predictor of early death in risk-adjusted models.21) Advanced donor age is associated with increased mortality, although there is conflicting results.22)23)24) However, with increased life expectancy, we can expect better medical outcomes from aged donors than in the previous era. Blanch et al. suggested that carefully selected donor hearts over 50 years of age may have similar long-term survival and related outcomes as younger donor organs.22) It is widely accepted that life expectancy reported by the World Health Organization has increased. Between 2000 and 2019, global life expectancy at birth increased from 66.8 years in 2000 to 73.3 years in 2019, and healthy life expectancy increased from 58.3 to 63.7 years.25) Indeed, recent ISHLT registry and Eurotransplant reports have shown an increase in the average recipient and donor age.1)26)
During brain death, a surge in the adrenergic response results in pulmonary and systemic hypertension, which increases the afterload in both ventricles, causing myocardial ischemia and stress-induced cardiomyopathy.10) Additionally, prolonged cardiopulmonary resuscitation or severe hypoxia induced by suicide deteriorates LV contractility. LV systolic dysfunction has been reported to occur in up to 42% of patients with brain death.27) However, Madan et al.28) reported that LVEF may frequently improve to the normal range on repeated transthoracic echocardiography (TTE) after brain death. Interestingly, hearts with improved systolic function over time (12–24 hours) showed clinical outcomes similar to those of hearts with an initially normal LVEF.28) These data highlight the importance of a second or third TTE evaluation before procurement in patients with poor initial systolic function. The Korean Organ Donation Agency does not routinely assess the recovery of LVEF in donor hearts unless requested. We apply a watch-and-wait strategy for assessing donor hearts with low LVEFs but high chances for improvement, e.g., prolonged cardiopulmonary resuscitation and stress-induced cardiomyopathy, to acquire follow up TTE results. Such watch-and-waits were unfeasible in several of our patients because the donor care physician did not concur with the second TTE exam.
In addition, dysrhythmias are common (25–32%) in patients with brain damage due to activation of the hypothalamic–pituitary–adrenal axis.29) Some cases are caused by extreme volume loss combined with disturbances in electrolytes and arterial gas disorders caused by central diabetes insipidus in brain-dead patients. However, most neurogenic arrhythmias are benign, and proper donor management with volume replacement along with serial electrocardiogram tracings can save transplantable hearts.29) In our experience, donor #3 showed junctional bradycardia with a heart rate of <50 beats/min and recovered normal sinus rhythm during donor management (Supplementary Table 1).
Actively using MD hearts could be an effective way to expand the donor pool and shorten waiting time. However, it is challenging because short- and long-term results should be guaranteed. Although this study included data from a single center, the results showed no significant statistical difference in PGD and long-term survival between the MD and NMD groups.
These findings indicate that carefully selected ‘marginal’ donor hearts could be used to address the donor shortage without increasing the risk of negative events and may actually result in optimal outcomes for HTx. Present study has all potential limitations inherent to retrospective/observational design. As the data were retrospectively collected from a single center, geographic and demographic biases could be present. Even with various customized analyses, several potential confounding factors may have influenced the study. The average follow-up duration was not sufficient for estimating coronary allograft vasculopathy, accounting for approximately 47.4% of post-transplant deaths at 10 years.30) We conducted post-hoc power analysis and the observed power was calculated as 5.8% for mortality and 12.8% for the PGD. In this study, both the relatively small sample size and total number of events reduced the post-hoc power. For this reason, we could not statistically evaluate the risk factor of death, but instead evaluated the risk factors of PGD. Therefore, the further study with larger sample size is need. Follow-up was good, but there were deaths of various causes, which limit the clinical impact of MD on survival.
In conclusion, HTx is expected to continue as an important option for treating advanced heart failure. Active use of the MD could be one of the solutions to the worldwide shortage of donors. Although this was an underpowered cohort, our findings suggest that the selected MD hearts can achieve comparable clinical outcomes to NMD hearts, especially in HTxs using MDs in low-risk recipients.
 XML Download
XML Download