

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Spinal cord injury (SCI) can be classified into traumatic SCI (TSCI) and non-traumatic SCI (NTSCI) according to the primary mechanism. In general, TSCI is caused by traumatic accidents, such as sports, traffic accidents, falls, or assaults.1 Conversely, NTSCI is not caused by traumatic accidents, but by various etiologies. The most common causes are suggested to be degenerative disorders, congenital or genetic diseases, benign or malignant tumors, vascular diseases, infections, or inflammation.2345
Globally, the number of patients with NTSCI is increasing in developed countries due to population aging.3 Patients with NTSCI are at increased risk of disability and have a high risk of death or complications. Therefore, it is important to examine the incidence of NTSCI and measure the size of the disease in order to reduce its enormous socioeconomic burden.
Although both patients with TSCI and those with NTSCI have impaired spinal cord function, patients with NTSCI have distinct epidemiological characteristics.6 Previous studies have reported that patients with NTSCI are older than those with TSCI in many developed countries.267 In addition, the proportion of men was slightly higher than that of women among patients with NTSCI, while the men-to-women ratio was less prominent in patients with TSCI.678 Previous studies have also demonstrated that the incidence of NTSCI was higher than that of TSCI in developed countries.91011
Nevertheless, epidemiological studies on NTSCI are still lacking in many countries compared to those on TSCI. The reason for this might be that the etiology of NTSCI is very complicated and following up the history of various etiologies is difficult. In this regard, Korea is one of the most suitable countries to study the incidence of diseases or injuries on a national scale.121314 The Republic of Korea implements universal health coverage that provides national health insurance to all citizens from birth to death. Through a retrospective cohort design, we were able to identify the past histories of various etiologies as well as the occurrence of NTSCI during the past 14 years using the data of the National Health Insurance Service (NHIS) for the period from 2007 to 2020. Moreover, since Korea is one of the representative developed countries in Asia where aging is progressing the fastest in the world, a study on the incidence of NTSCI in Korea is extremely insightful. According to a report from the U.S. Census Bureau released in 2022, Asia’s population is aging faster than any other part of the world, and the aging population in Asia is expected to nearly triple over the next 40 years.15 Therefore, identification of the epidemiologic pattern of NTSCI in Korea would be helpful in predicting its epidemiology across Asia.
The aims of this study were: 1) to investigate the trend of NTSCI incidence in Korea during the past 14 years on a nationwide scale, and 2) to describe the characteristics of these patients according to the NTSCI type or etiology.
METHODS
Data source and study population
The incidence of NTSCI in Korea was evaluated using data from the NHIS for the period between 2007 and 2020. The NHIS is a national health insurance that covers the entire population of Korea, which numbers over 50 million people.16 It provides lifelong coverage for the prevention and treatment of diseases and injuries caused by everyday activities.17 It also covers all general medical claims, including inpatients and outpatients with health care institutions.18
Patients with NTSCI were identified according to the International Classification of Diseases, 10th revision (ICD-10). Patients who were diagnosed with both paralytic and reliable etiologies were selected as the study population. First, we selected patients admitted to a hospital between 2007 and 2020 with a diagnosis of paralysis, including paraplegia, tetraplegia, or cauda equina. Among them, only patients who had a diagnosis of etiologies (congenital or genetic, degenerative, infection, inflammatory, benign or malignant tumor, vascular, or unknown diseases) established prior to the diagnosis of paralysis were selected as the final study population. The ICD-10 codes for paralysis and etiologies refer to previous study of Jaglal et al.19 and are presented in Supplementary Tables 1 and 2. Only newly diagnosed patients with NTSCI during the study period were included to avoid double counting of one person from each year.
Statistical analysis
The annual number of NTSCI cases was divided by the mid-year population estimates (Supplementary Table 3) to calculate the crude incidence. The mid-year population estimates were derived from the annual resident population data from the Korea National Statistical Office (http://www.kosis.kr). The age-specific incidence was calculated by dividing the number of cases in 10-year age groups by the total number of individuals in that age group. Direct standardization was used to calculate the age-adjusted incidence using the 2005 Korean or the 2000 United States population as a standard population. Joinpoint regression analysis was used to calculate the annual percentage changes (APCs) in NTSCI incidence across the study period.20 The Cochrane-Armitage trend test was used to examine the trends of NTSCI cases according to the types or etiologies.
SAS version 9.4 (SAS Institute, Cary, NC, USA) was used for statistical analysis. The Cochrane-Armitage trend test was conducted using R version 4.0.1 (R Development Core Team, Vienna, Austria). APCs were calculated using the Joinpoint Regression Program version 4.9.0.0 (National Cancer Institute, Bethesda, MD, USA). All reported P values are 2-sided. Statistical significance was set at P < 0.05.
Ethics statement
The requirement for ethical approval for this study was waived by the Institutional Review Board of Seoul National University Hospital, Seoul, Korea (IRB No. E-2011-004-1168). The requirement for informed consent was also waived because all data in the NHIS were anonymized and deidentified.
RESULTS
Table 1 shows the annual incidence of NTSCI in Korea from 2007 to 2020. During the entire study period, the number of NTSCI cases increased about threefold, from 1,254 in 2007 to 3,317 in 2020. After stratification by sex, the number of NTSCI cases increased in both men and women, from 655 and 599 in 2007 to 1,833 and 1,484 in 2020, respectively. The crude incidence of NTSCI in the overall population increased from 25.52 per million in 2007 to 64.60 per million in 2020, with a significant APC of 8.55% (P < 0.05). The age-adjusted incidence with the standard population of Korea also presented significant increases, from 24.11 per million in 2007 to 39.83 per million in 2020, with a significant APC of 4.93% (P < 0.05). Similar results were obtained for the age-adjusted incidence with the standard population of the United States. After stratification by sex, the crude and age-adjusted incidence increased in both men and women, but the incidence in men was higher and increased more rapidly than that in women.
Table 1
Annual incidence rate of non-traumatic spinal cord injury (per million)
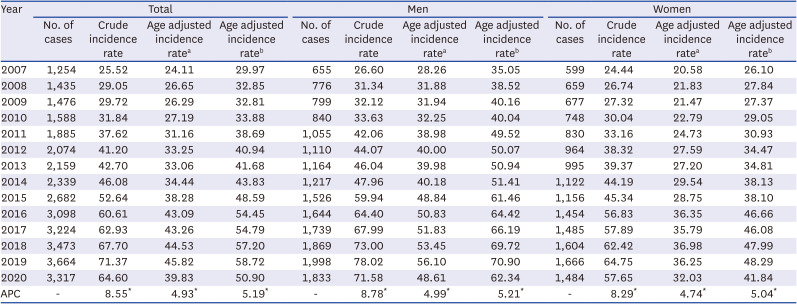
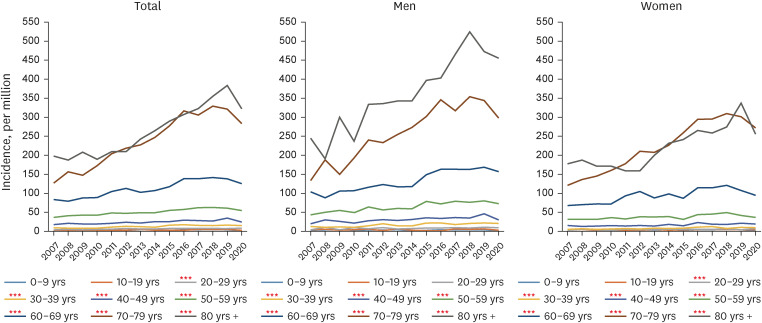
Fig. 1 presents the annual age-specific incidence of NTSCI according to age groups and sex. Between 2007 and 2020, those in their 70s and 80s or older presented the highest values and fastest increase in age specific incidence (70s APC = 7.41%, P < 0.001; 80s or older APC = 5.80%, P < 0.001). The age-specific incidence for those in their 20s to 60s also showed significant increase. In men, the age-specific incidence was the highest in those in their 80s or older, while in women, those in their 70s and 80s or older had the highest incidence at a similar level. From 2007 to 2020, the incidence difference between men and women was the largest among older adults over 80 years of age (65.26 per million in 2007 and 200.87 per million in 2020). During the study period, the age-specific incidence was higher in men than that in women in all age groups over the age of 20.
Fig. 1
Incidence of non-traumatic spinal cord injury according to age groups and sex.
Red asterisk indicates an increasing trend.
***P for trend < 0.001.
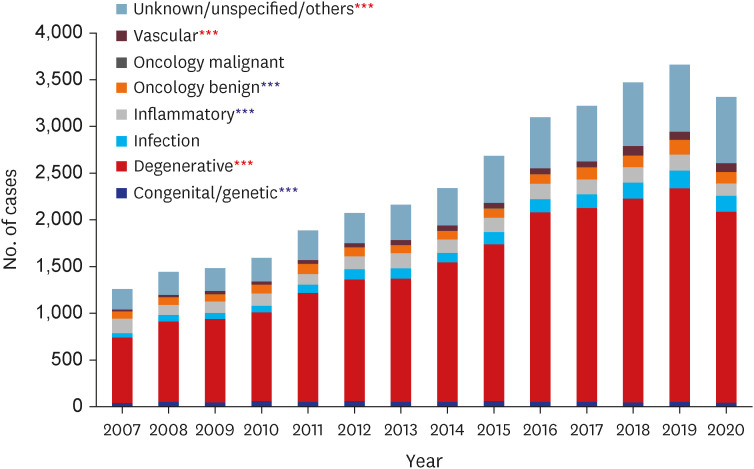
The annual distribution of NTSCI cases according to the type of NTSCI is presented in Fig. 2. The number of cases increased from 2007 to 2020 for all three types of NTSCI (tetraplegia, paraplegia, and cauda equina). However, the proportion of paraplegia and cauda equina among the total population increased significantly (from 36.55% to 42.89% for paraplegia, and from 21.04% to 27.50% for cauda equina), whereas that of tetraplegia decreased significantly (from 42.41% to 29.61%). With regard to the etiologies, degenerative diseases accounted for the largest proportion among all etiologies (Fig. 3). The distribution of the etiologies over time showed that the proportion of degenerative, vascular, and unknown diseases increased significantly from 2007 to 2020 (from 55.85% to 61.51% for degenerative, from 1.82% to 2.80% for vascular, and from 17.33% to 21.48% for unknown diseases). In contrast, the proportion of congenital, inflammatory, and benign diseases decreased significantly during the same period (from 3.09% to 1.45% for congenital, from 12.74% to 4.04% for inflammatory, and from 5.46% to 3.61% for benign diseases).
Fig. 2
Distribution of the types of non-traumatic spinal cord injury.
Red asterisk indicates an increasing trend; blue asterisk indicates a decreasing trend.
***P for trend < 0.001.
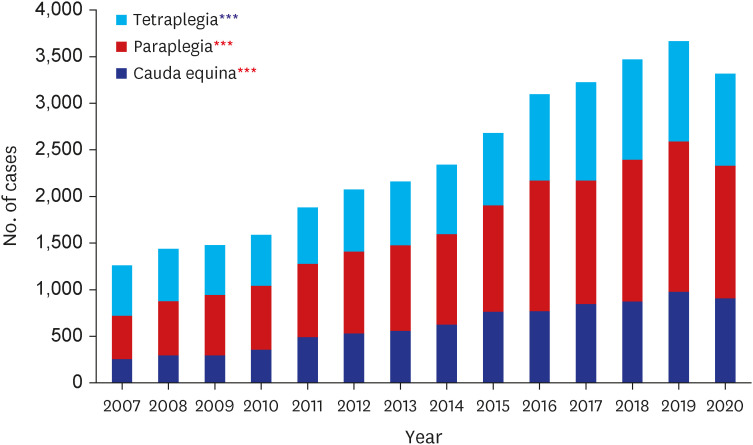
Fig. 3
Distribution of the etiologies of patients with non-traumatic spinal cord injury.
Red asterisk indicates an increasing trend; blue asterisk indicates a decreasing trend.
***P for trend < 0.001.
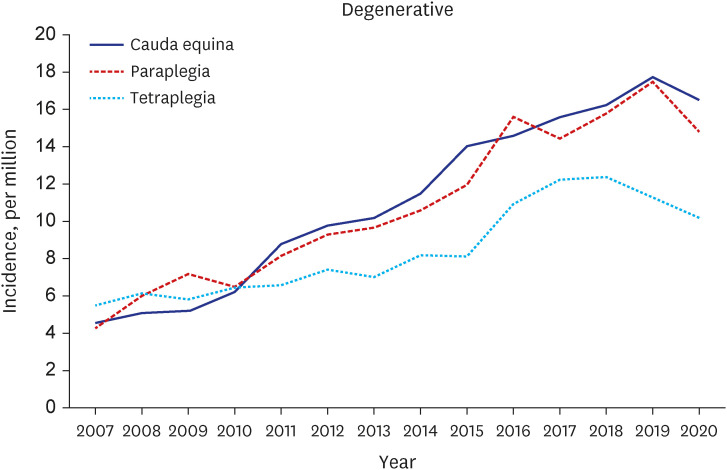
The distribution of etiologies according to the type of NTSCI between 2007 and 2020 is shown in Supplementary Fig. 1. Overall, from 2007 to 2020, the proportion of paraplegia increased, whereas that of tetraplegia decreased in most etiologies. The changes in the type of paralysis over time according to each etiology are shown in Fig. 4 and Supplementary Fig. 2. In patients with NTSCI with degenerative etiology, which accounted for the highest proportion among the etiologies, the incidence of paraplegia and cauda equina increased more rapidly than that of tetraplegia (Fig. 4). The changes for other etiologies are shown in Supplementary Fig. 2. In most etiologies, except for congenital and malignant diseases, the incidence of all three types of NTSCI showed increasing trends annually.
Fig. 4
Changes in the types of paralysis in NTSCI patients with degenerative etiology.
NTSCI = non-traumatic spinal cord injury.
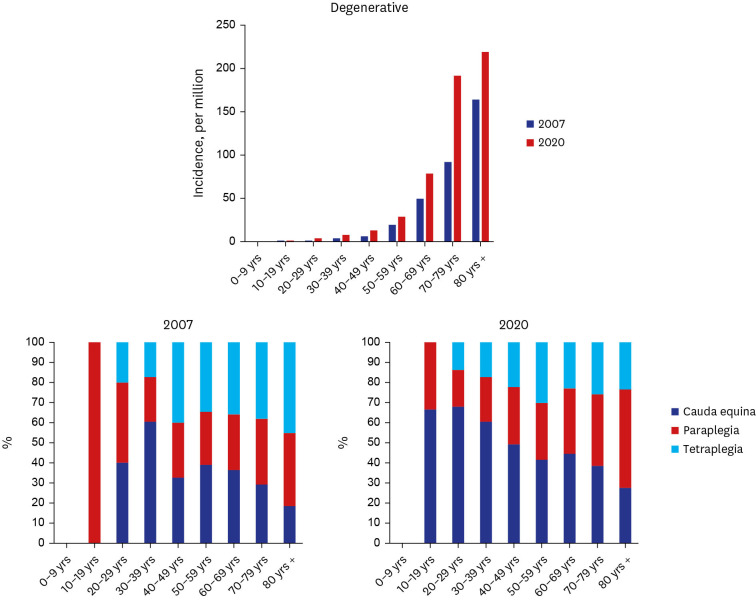
The median age of patients with NTSCI for all etiologies increased in 2020 compared to that in 2007 (Supplementary Fig. 3). Etiologies with the largest increase in the median age were benign and vascular diseases. Fig. 5 presents the distribution of age groups in patients with NTSCI with degenerative etiology in 2007 and 2020. Among patients with degenerative etiology, older adults in their 70s showed the largest increase in incidence difference between 2007 and 2020. In addition, the proportion of paraplegia and cauda equina increased, whereas that of tetraplegia decreased in this population. Similarly, in most etiologies except for congenital disease, the proportion of older adults over 70 years of age showed the largest increase in incidence difference between 2007 and 2020 (Supplementary Fig. 4).
DISCUSSION
To the best of our knowledge, this is the first study that reported the incidence of NTSCI in Korea on a national scale using the NHIS database. In this study, we investigated the trends in the incidence of NTSCI over the past 14 years and identified the characteristics of these patients according to the types or etiologies of NTSCI. The age-adjusted incidence of NTSCI increased by 4.93% annually from 24.11 per million in 2007 to 39.83 per million in 2020. Patients aged > 70 years presented the highest age-specific incidence with rapid increments from 2007 to 2020. After stratification by sex, the age-specific incidence was higher in men than that in women in all age groups over the age of 20. With regard to the type of NTSCI, the proportion of paraplegia and cauda equina increased, whereas that of tetraplegia decreased significantly from 2007 to 2020. The proportion of degenerative diseases was the largest among all etiologies and significantly increased during the study period.
In line with our results, several previous studies have also reported higher NTSCI incidence in men or higher proportion of men patients among NTSCI patients compared to women patients in countries such as Ireland,6 Norway,7 UK,21 Australia,9 New Zealand,22 and Korea.232425 Notably, we found that the difference in incidence between men and women patients was the largest among older adults over 80 years old. Since women have a longer life expectancy, the total number of women population, which is the denominator of the incidence rate in the older group, is greater than the men population. When considering NTSCI patients aged > 80 years in 2020, the reported number of men and women patients were 287 and 325, respectively. However, the total count of the men population aged > 80 years was 627,780 and that of the women population was 1,267,931, a difference of more than double. Additionally, the NTSCI incidence in 2020 slightly decreased compared to that in 2018 or 2019, and we believe that this could be related to the outbreak of the coronavirus disease 2019 (COVID-19) global pandemic. Since our incidence results were calculated based on claims data, the decrease in medical utilization of NTSCI patients due to COVID-192627 can be seen as a decrease in NTSCI incidence rate. Therefore, further studies are needed to compare the trend on NTSCI incidence and patient’s medical utilization after the COVID-19 outbreak with follow-up data.
In this study, the NTSCI incidence in older adults and the proportion of degenerative diseases were the highest among patients with NTSCI in Korea and showed significantly increased trends over the past 14 years. Several previous studies in developed countries have reported consistent results. A prospective population-based study in Ireland demonstrated that the age-specific incidence of NTSCI was highest among older adults over 76 years of age and the most common etiology was degenerative disorders.6 Another population-based study in Victoria, Australia, reported that the age-specific incidence of NTSCI among older adults aged 75 years or older was 14 times higher than that in younger patients aged 15–24 years (rate ratio of patients aged 75–84 years = 14.4; rate ratio of patients aged 85 years or older = 14.6).9 The authors also found a strong correlation between age and the incidence of NTSCI in both men and women.9 A provincial study in Manitoba, Canada, found that older adults aged 61–70 years accounted for the highest proportion among patients with NTSCI and the most common cause was spondylomyelopathy, a type of degenerative disease.21
In general, aging and degenerative diseases are closely related. As aging progresses, aging of the spinal cord also occurs. Furthermore, the paraspinal muscle mass and vertebral bone mineral density decrease during the aging process.28 These aging phenomena may lead to frequent occurrences of degenerative diseases around the spinal cord among older adults, such as spondylolisthesis and spinal stenosis.29303132 In this context, the incidence of etiologies related to the aging process, such as infections, vascular, and oncologic diseases, has also increased dramatically among older adults over the past 14 years. As Korea is a rapidly aging society, these results have significant implications in terms of preventing NTSCI among older adults. Since NTSCI is not a disease caused by a sudden accident, but develops gradually from the etiology, it is expected that permanent disability can be minimized if older patients with the corresponding etiology are actively monitored and rehabilitation treatment is started early in the onset of NTSCI. As the aging problem is a global issue, our results have important implications for many other developed countries as well.
Our study found that the proportion of paraplegia and cauda equina increased, whereas that of tetraplegia decreased significantly over the past 14 years in Korea. In particular, paraplegia had the highest proportion accounting for 42.9% among the three types of paralysis in 2019 (29.6% for tetraplegia, 27.5% for cauda equina). According to a previous meta-study that reported the worldwide distribution of NTSCI incidence, the proportion of tetraplegia was higher than that of paraplegia in the Asia-Pacific region, whereas the proportion of paraplegia was higher than that of tetraplegia in all the other WHO regions, except for the Asia-Pacific region.3 In this previous study, the results in the Asia-Pacific region were reported based on the NTSCI incidence rate in Okayama Prefecture, Japan between 1988 and 1989.33 However, since this present study was investigated the incidence of NTSCI in the entire of Korean population, our results can be considered more representative incidence rates for the Asia-Pacific region. In addition, the time point when each study was conducted also can be one of the reasons explaining the difference between the results of the two studies. Even in our study, the proportion of tetraplegia was higher than that of paraplegia in 2007 as the results of Japan, accounting for 42.2% and 36.6%, respectively. Therefore, the proportion of tetraplegia may have been higher in the Asia-Pacific region in 1989. Consequently, we reported a more recent, and representative NTSCI incidence rate in the Asia-Pacific region through this study.
Another noteworthy point is the increased proportion of patients presenting cauda equina. In terms of coverage by national health insurance, since cauda equina syndrome is a type of peripheral nerve lesion, there are restrictions on the amount of rehabilitation treatment or treatment period for patients with cauda equina syndrome, compared with patients with spinal cord injury, which is central nerve injury. However, since the proportion of patients with cauda equina syndrome is steadily increasing, continuous awareness and appropriate medical policy are needed for those patients.
This present study has two major strengths. First, it was a population-based study covering the entire Korean population. This was possible because Korea is one of the few countries in the world that provide life-long coverage by national health insurance for the entire population. As NTSCI is not caused by traumatic accidents, such as automobile or industrial accidents,834 the majority of patients with NTSCI in Korea would be included in the NHIS data. Second, this is the first study that reported the incidence of NTSCI on a national scale in Korea. Although several previous studies have reported the incidence of NTSCI in Korea, the results were not on a national scale.232435 It is important to measure the incidence of NTSCI on a national scale in order to provide a rationale for health care policies for patients with NTSCI.
There are several limitations to this study. First, because this is the first study that reported the incidence of NTSCI on a national scale in Korea, further studies are needed to validate the present results. The method used in this study could be applied in other studies to obtain comparative estimates. Second, since NHIS data are insurance data, clinical data, such as patients’ symptoms or severity, were not included. Third, some patients with non-symptomatic or mildly symptomatic NTSCI who did not visit a hospital or clinic may not be included in these data. However, since we analyzed a long follow-up period of 14 years, it is highly likely that even initially asymptomatic patients would have been included when the symptoms worsened over time. Fourth, a follow-up study is needed on the effect of these epidemiological changes on the medical costs or medical resource utilization.
In conclusion, this is the first population-based study of NTSCI epidemiology over 14 years in Korea using nationwide data. The incidence of NTSCI increased significantly during the study period both in men and women. Specifically, significant increases were observed in the proportion of older adults, patients with paraplegia or cauda equina, and patients with degenerative diseases. As Korea is one of the most rapidly aging countries in the world, it is necessary to minimize permanent disability through rehabilitation treatment in older patients as well as to prevent NTSCI. Therefore, there is a need for a medical policy to provide high-quality and sufficient rehabilitation treatment to NTSCI patients.
 XML Download
XML Download