

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Female sexual dysfunction is a complex disease that can cause serious personal distress and is a prevalent disorder among women worldwide.12 Female sexual dysfunction is traditionally defined as sexual difficulties involving desire, arousal, pain or discomfort, and orgasm.34 The integral sexual function can only be achieved by satisfying the multi-sexual responses in various aspects including mental, physical, and relational factors. If the factors are disturbed in women, no matter how minor, it can be difficult to achieve full sexual functioning.
As the lower part of the uterus and the ceiling of the vagina, the cervix is a key organ in a woman’s sexuality for structural, functional, and symbolic reasons. Many researchers have focused on the physiologic role of the cervix in sexual function and have argued that the cervix may play a distinct role in sexual function during vaginal intercourse because it is rich in blood vessels, innervated by the uterosacral plexus, and forms the upper barrier of the vagina.5 In a similar context, several studies investigated whether total removal of the cervix during hysterectomy, a very common surgery in obstetrics and gynecology, alters female sexual function compared to preservation of the cervix. However, the results remain controversial.67891011
Loop electrosurgical excision procedure (LEEP) is the most commonly performed gynecological procedure for diagnosis and treatment when suspicious precancerous lesions are found on a Papanicolaou (Pap) smear, human papillomavirus (HPV) test, colposcopy, or punch biopsy of the cervix.121314 LEEP may impair the vascular supply and innervation of the cervix, causing pain during intercourse or negatively affecting a woman’s sexual function.
The purpose of this study was to investigate the effect of LEEP, which induces structural changes in the cervix and is used for treating a suspicious premalignant lesion, on the sexual function of Korean women.
METHODS
Study design and population
To analyze changes in sexual dysfunction by cervical conization, we conducted a questionnaire survey of sexual dysfunction among patients who visited our clinic for LEEP. Eligible participants were sexually active women 20 years of age or older with abnormal Pap smear or cervical punch biopsy results and required LEEP. Patients with severe sexual dysfunction due to trauma or surgery or who were unable to have sexual intercourse due to serious physical diseases were excluded. Patients who could not respond to the questionnaire due to communication problems or psychological disorders or did not consent to the questionnaire were also excluded. Sexual dysfunction and distress were evaluated using the Korean version of the Female Sexual Function Index (FSFI) and the Female Sexual Distress Scale (FSDS) as self-reported questionnaires. Medical history including underlying diseases, HPV test results, menopausal status with hormonal therapy, and pathological result of LEEP and socio-demographic information such as age, body mass index (BMI), marital status, parity, smoking, drinking, occupation, and educational status were also collected. Questionnaire surveys were conducted twice, before and six to twelve months after LEEP.
FSFI
The FSFI is one of the most used validated questionnaires for evaluating female sexual dysfunction. In this study, the Korean version, of which the reliability and validity have been verified, was used.15 The survey consists of six domains (sexual desire, arousal, lubrication, orgasm, global satisfaction, and pain) and nineteen items. Total FSFI scores range from 2 to 36, and the total score is sum of the individual domain scores multiplied by each domain factor. Lower scores indicate more severe sexual dysfunction. Women with a total score of less than 26.55 were defined as patients with sexual dysfunction.1617 To evaluate sexual difficulty in each domain, the cutoff of the desire domain was defined as less than 2.4 points, and the cutoff of other domains was defined as less than 3.6 points.1819
FSDS
The FSDS is a 20-item scale used for evaluating sexually related personal distress in women.20 The total scores range from 0 to 80 (each item is scored from 0 to 4 points), with higher scores indicating greater sexual distress. In this study, a validated Korean version of the FSDS was used. The optimal cutoff score was 20, and scores above it indicated individual stress related to sexual function and activity.21
Statistical methods
Statistical analyses were performed using SPSS statistical software (version 26.0 for Windows; SPSS Inc., IBM® Corp., Armonk, NY, USA). The normality of distribution was examined using the Kolmogorov-Smirnov test. The Wilcoxon signed-rank test and McNemar’s test were used to compare the FSFI and FSDS scores, and the proportion of patients with certain FSFI and FSDS scores before and after LEEP. A one-sample t-test was used for numerical variables and a χ2 test or binomial test was used for categorical variables to compare baseline characteristics among study samples according to the number of survey completions. To identify the risk factors related to sexual dysfunction and distress, a univariate analysis of potential risk factors was performed and only variables significant at the 0.05 level were included in the subsequent multivariate logistic regression model. All statistical tests were two-tailed, and statistical significance was defined as P < 0.05.
Ethics statement
This was a prospective cohort study conducted at Ewha Womans University Mokdong Hospital from November 2015 to January 2018. The study protocol was approved by the Institutional Review Board (IRB) of Ewha Womans University Mokdong Hospital (IRB No.2015-09-007-001). Informed consent was submitted by all subjects when they were enrolled.
RESULTS
Study population
A total of sixty-two women consented to participate in the study and received the pre-LEEP questionnaire. One woman was excluded from the study because more than 60% of the questionnaire responses were blank. Thirty-seven women did not want to answer the post-LEEP questionnaire or failed to follow up after treatment. Twenty-four women completed both questionnaires before and after LEEP and were included in the final analysis. The proportion of patients who answered both questionnaires was 40.3%. Table 1 shows the socio-demographics and clinical characteristics of sixty-one patients who responded to the questionnaire more than once. The mean age of the patients was 41 years and nearly half (47.5%) of participants had a histological diagnosis of cervical intraepithelial neoplasia (CIN) III by LEEP. One patient who underwent a cesarean subtotal hysterectomy in the past was included in the final analysis because the cervix was preserved. Another patient was diagnosed with microinvasive squamous cell carcinoma after LEEP and underwent cold-knife conization to preserve fertility after performing additional imaging examinations for disease status and metastasis. The patient was finally diagnosed with cervical cancer stage IA1 and was excluded from the second questionnaire. An additional analysis was performed to determine whether the women who were finally included (n = 24) showed statistically similar basic characteristics, FSFI and FSDS scores before LEEP to the total participants (n = 61), and there were no significant statistical differences (Supplementary Table 1).
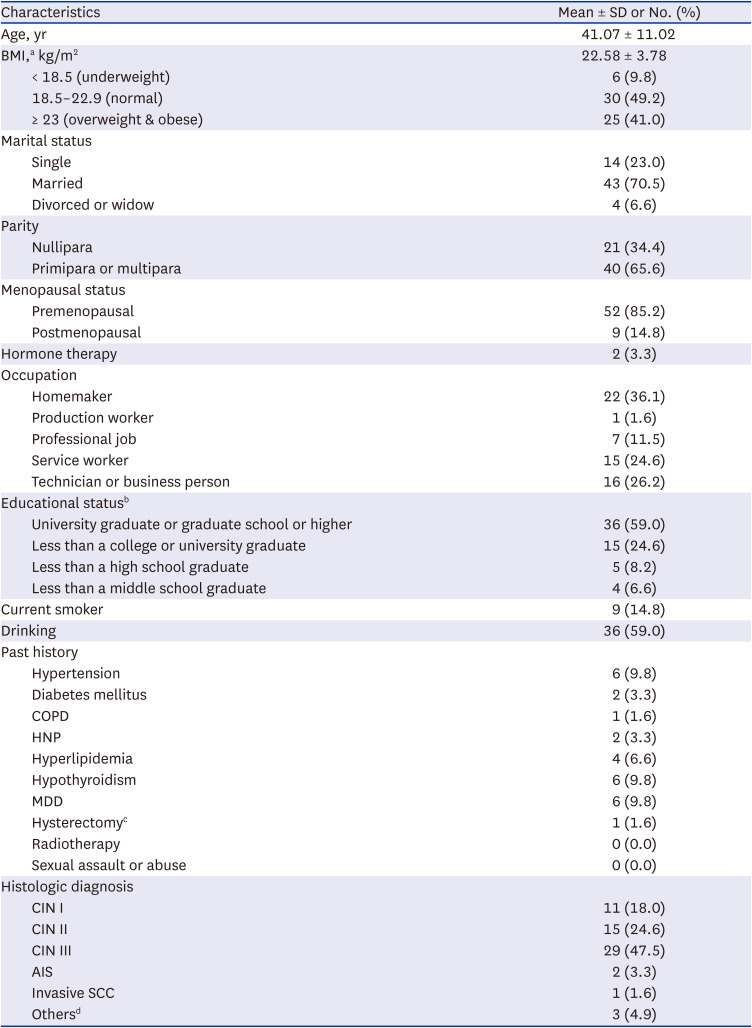
Table 1
Socio-demographic and clinical characteristics of the sixty-one women who responded to the questionnaire at least once
SD = standard deviation, BMI = body mass index, COPD = chronic obstructive pulmonary disease, HNP = herniated nucleus pulposus, MDD = major depressive disorder, CIN = cervical intraepithelial neoplasia, AIS = adenocarcinoma in situ, SCC = squamous cell carcinoma.
aBMI classification according to Asia-Pacific guidelines.
bOne had no data available.
cOne underwent cesarean subtotal hysterectomy.
dOthers included two cases of cervicitis and one cervical polyp.
![]()
Assessment of LEEP-related changes in sexual dysfunction and sexual distress
Of the total participants (n = 61) 64.5% of the patients met the diagnostic criteria for female sexual dysfunction by the FSFI before LEEP. Of the twenty-four patients who completed both questionnaires before and after LEEP, female sexual dysfunction was reported by 62.5% and 66.7%, respectively.
Changes in total FSFI scores were not significant after LEEP (23.1 vs. 22.4, P = 0.399, Table 2). Based on the cutoff for each subdomain of the FSFI, the increase in incidences of sexual dysfunction by LEEP were not significant (P > 0.05, Table 2). LEEP-related changes in FSDS scores were not statistically significant (P = 0.670, Table 2) and the number of women experiencing sexual distress (FSDS ≥ 20) was not significantly increased after LEEP (P = 0.687, Table 2).
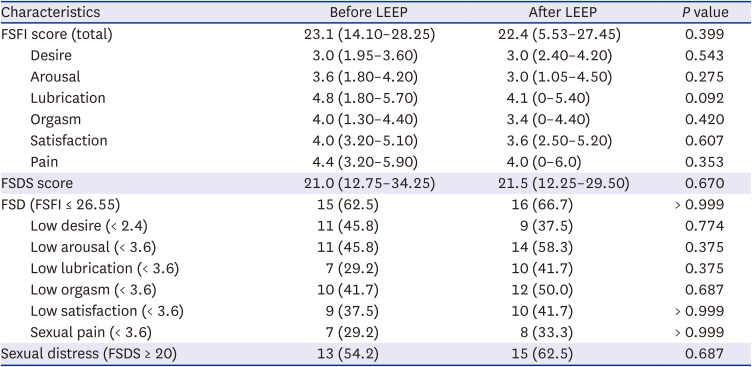
Table 2
Changes in scores of FSFI & FSDS scores and rates of diagnosis before and after LEEP in twenty-four patients
Values are presented as median (interquartile range) or number (%). Data were analyzed using the Wilcoxon signed-rank test and McNemar’s test. Changes in total FSFI & FSDS scores were not significant after LEEP. Changes in the number of patients with sexual dysfunction and sexual distress according to the cutoff of FSFI & FSDS were not statistically significant.
FSFI = Female Sexual Function Index, FSD = female sexual dysfunction, FSDS = Female Sexual Distress Scale, LEEP = loop electrosurgical excision procedure.
![]()
To analyze whether the status of the disease affects sexual dysfunction in women, the FSFI and FSDS scores were classified according to the final pathological results (benign or CIN I/II vs. CIN III or adenocarcinoma in situ) of LEEP. As a result, LEEP-related changes in FSFI and FSDS scores according to disease status were not statistically significant (P > 0.05, Table 3). Similarly, FSFI and FSDS scores after LEEP were not statistically altered by other factors related to patients’ data such as BMI, marital status, parity, menopausal status (P > 0.05, Supplementary Table 2).

Table 3
Changes in FSFI and FSFD scores by LEEP according to final pathological outcomes (n = 24)
Values are presented as median (interquartile range). Data were analyzed using the Wilcoxon signed-rank test.
FSFI = Female Sexual Function Index, FSDS = Female Sexual Distress Scale, LEEP = loop electrosurgical excision procedure, CIN = cervical intraepithelial neoplasia, AIS = adenocarcinoma in situ.
aBenign diseases included one case of cervicitis and one cervical polyp.
![]()
Logistic regression analysis was conducted to identify risk factors related to pre-LEEP sexual dysfunction for all patients who completed the questionnaire at least once. Univariate analysis showed that there was a significant association between sexual dysfunction and age, BMI, parity, and occupational status (P < 0.05, Supplementary Table 3). Among these variables that showed significant association by univariate analysis, multivariate analysis demonstrated that age (odds ratio [OR], 1.191; 95% confidence interval [CI], 1.051–1.349) and occupational status (service worker vs. homemaker, OR, 0.108; 95% CI, 0.012–0.937) were independent predictive variables for female sexual dysfunction (P < 0.05, Supplementary Table 3).
DISCUSSION
The aim of this study was to investigate the effects of LEEP, which induces partial structural changes in the cervix, on the sexual function of Korean women.
First, our results showed that LEEP itself did not significantly affect a woman’s sexual functioning and did not exacerbate sexual distress. These results are similar to the findings of other recent studies on the effects of LEEP on female sexual dysfunction. Michaan et al.22 studied sexual functional changes in 55 women before and after cervical conization. They reported no significant differences in the FSDS-revised, FSFI, and Hospital Anxiety and Depression Scale scores before and after conization (P > 0.05), and the procedure did not affect either physical or psychological sexual function. Hellsten et al.23 investigated women’s psychosexual problems between LEEP and non-LEEP groups using the State-Trait Anxiety Inventory Form Y and a psychosexual questionnaire. They found decreases in “spontaneous interest” or “frequency of intercourse” in sexual functioning for two years in women with abnormal Pap smear results. However, these changes were not affected by LEEP. In contrast, Inna et al.24 studied female sexual function changes in 89 patients before and after LEEP using a self-developed questionnaire. They reported significant changes after LEEP in overall sexual intercourse satisfaction, vaginal elasticity, and orgasm satisfaction (P < 0.05). Although there is no clear explanation for the difference from our results, differences in assessment tools for female sexual dysfunction may be a contributing factor.
Similar to the reports on LEEP, several studies have reported conflicting results on the changes in female sexual function depending on whether or not the cervix was preserved during hysterectomy.6891011 These conflicting findings suggest that the role of the cervix on female sexual function remains debatable. Unfortunately, there are not many studies on sexual dysfunction in Asian women, and studies on sexual dysfunction related to cervical procedures are insufficient. Our study results suggest that minor cervical damage inducing partial structural changes, such as LEEP, did not affect sexual dysfunction in Korean women.
Second, our data showed a high prevalence of female sexual dysfunction of more than 60% before and after LEEP. The prevalence of sexual dysfunction in our study was higher than the general prevalence (46.7%, 95% CI, 42.3–51.1%) in Korean women reported by Song et al.25 Michaan et al.22 found that many patients with cervical dysplasia experienced sexual dysfunction (49% and 59%, P = 0.388), sexual distress (53% equally, P > 0.999), and anxiety (49% and 47%, P > 0.999) before and after cervical conization. Ma et al.26 reported that women with CIN had a higher prevalence of FSD compared to healthy controls (66.7% vs 43.3%, P = 0.011) and significant impairment in the arousal domain. These findings suggest that female sexual dysfunction may be more closely related to an already diagnosed disease state than to structural changes in the cervix. In an actual clinical setting, many women diagnosed with cervical dysplasia or in need of LEEP had a common concern about persistent infections and the transmission of HPV to partners. The patients were also afraid of progressing to cancer and wondered if they could continue their sex lives. In particular, the higher the grade of the cervical disease, the greater the concern about sexual activity. These psychological states might be one of the factors considerably affecting female sexual functioning. Hence, we analyzed whether the frequency of sexual dysfunction further increased according to the disease state of the cervix through the pathological results of LEEP, but unfortunately no significant results were found.
We additionally analyzed the possible clinical risk factors associated with sexual dysfunction in women requiring LEEP. In general, age is a known major factor for sexual dysfunction and individual general health status, disease status, and sociodemographic conditions are risk factors for sexual dysfunction.252728293031 According to our results of multivariate analysis, age and occupational status were risk factors for female sexual dysfunction.
Few studies have been conducted on the relationship between female sexual function and the role of the cervix, in particular, in Asian women. This prospective research study was one of the few studies to investigate the effect of LEEP on sexual function in Korean women. This study has the strengths of evaluating female sexual dysfunction and sexual distress using validated tools, the FSFI and FSDS. However, this study has several limitations. First, the number of women participating in the study was small and the follow-up survey of some patients failed. This may have been due to the cultural background which makes women feel ashamed or reluctant to share sexual problems and experiences. To make up for this limitation, we analyzed whether there were statistical differences between the total 61 participants and the 24 women who answered the second questionnaire after LEEP. As a result, no statistical differences were observed in the basic demographics and FSFI and FSDS scores prior to LEEP. Second, since this study used a self-reported questionnaire and the follow-up period was short, there may have been recall bias. In addition, anxiety and depression tests related to emotional and psychological sexual function were not performed in our study. It is necessary to encourage patients to participate in research and respond to continuous follow-up surveys and conduct a large population study using various investigative scales in the future.
In conclusion, a significant proportion of women with CIN complain of sexual dysfunction and distress before and after LEEP. The procedure itself, which causes structural changes in the cervix, may not be associated with negative effects on sexual function.
 XML Download
XML Download