

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Korea Disease Control and Prevention Agency (KDCA) approved of providing a fourth dose of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine (Pfizer mRNA vaccine, Moderna mRNA vaccine or Novavax protein vaccine) for immunocompromised individuals starting from February 14, 2022. Afterward, the vaccination program was extended to individuals over the age of 60 starting from April 14, 2022 and to those aged 50 to 59 and those with underlying diseases starting from July 18, 2022.1 All of these groups were advised to receive their vaccination at least four months after their third dose. These vaccination guidelines of South Korea are similar to those of Israel, which was the first country to implement a fourth vaccination program. However, there was a difference in that the South Korean vaccination guidelines did not include any directions for healthcare workers (HCWs).23
According to studies conducted in countries that have already implemented quaternary vaccines through a national initiative, the fourth dose of SARS-CoV-2 vaccine appears to be helpful in reducing the severity and mortality rate among immunocompromised and elderly people.45 A recent multicenter cohort study of HCWs in Israel reported a breakthrough infection rate of 6.9% for those who received four doses and 19.8% for those who received three doses.6 Based on these results, Cohen et al.6 contended that a fourth dose of vaccine for HCWs could help maintain the function of the healthcare system during the pandemic. However, the South Korean healthcare system is different to those of European countries and the United States. The guidelines for a fourth dose in South Korean HCWs need to be clarified.
We examined the real-world effectiveness of the third dose of vaccine in preventing coronavirus disease 2019 (COVID-19) among South Korean HCWs over eight months, and we simultaneously analyzed the change in titers of neutralizing antibody against the omicron variant (B.1.1.529).
METHODS
Study design and participants
From November 23 to December 24, 2021, a total of 2,133 HCWs at Soonchunhyang University Bucheon Hospital received BNT162b2 as their third COVID-19 vaccine dose (booster vaccination). Among them, 43 HCWs volunteered to participate in the current study. All participants had no history of COVID-19 infection and no suspected symptoms at the time of study enrollment.
Blood samples of participants were taken three times: one month, four months and eight months after the third dose of vaccination. The specimens were stored in the biobank of Soonchunhyang University Bucheon Hospital, a member of the Korea Biobank Network. The samples were analyzed using a GenScript SARS-CoV-2 surrogate virus neutralization test (sVNT) kit (Genscript Biotech Corporation, Piscataway, NJ, USA), which was also used in our previous study.7 Participants were given a self-administered questionnaire. The data gathered via the questionnaire included the following information: sex, age, occupation in the hospital, date of vaccination, types of vaccine received, history of COVID-19 infection, confirmed date of COVID-19 infection, and healthcare facilities visited for symptom care after COVID-19 infection.
During the study period, the omicron variant was predominant in South Korea, and we investigated the SARS-CoV-2 infection rate after the third dose. COVID-19 infection was only confirmed by reverse transcriptase-polymerase chain reaction (RT-PCR) testing with nasopharyngeal swabs. Although the variant could not be identified by PCR testing, the detection rate of omicron in South Korea was 99–100% during the time of PCR testing in our study8; therefore, we defined participants with positive outcomes as SARS-CoV-2 (presumed omicron variant) infected participants. For further analysis, we divided the subjects into SARS-CoV-2 (presumed omicron variant)-infected and uninfected groups. First, sVNT inhibition score eight months after the third dose were compared between SARS-CoV-2 (presumed omicron variant)-infected and uninfected groups. Then, the sVNT score at one month and four months after the third dose were compared between the two groups. Additionally, we plotted and compared the patterns of change in sVNT values over the eight months following the third dose.
Serological assays
To evaluate neutralizing activity against the B.1.1.529 (omicron variant), an ELISA-based sVNT was used. The B.1.1.529 spike receptor binding domain protein has the following amino acid changes: G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, G496S, Q498R, N501Y, Y505H and T547K. Further details on the serological assays used can be found in a previous study.7
Statistical analysis
Statistical analyses were performed using the software GraphPad Prism (version 9.3.1) and R (version 4.0.2). All measurements and data analysis results are presented as means ± standard deviations (SDs), medians, interquartile ranges (IQRs), ranges for continuous variables and frequencies (percentages) for categorical variables. When comparing two or more independent groups, the nonparametric Kruskal–Wallis test was used for continuous variables while independent two-sample t-tests or chi-square tests were used for categorical variables. Repeated-measures analysis of variance (ANOVA) was used to compare the continuous variables among two or more dependent groups. All tests used were two-tailed, with P < 0.05 considered statistically significant.
RESULTS
Baseline characteristics of the participants
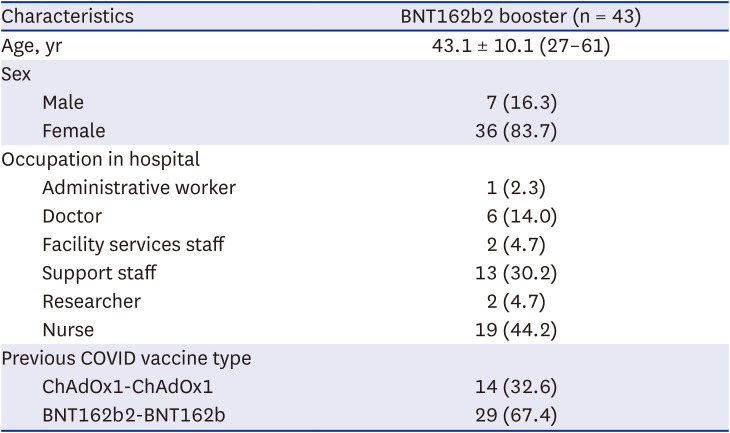
A total of 43 HCWs were enrolled in this study. The median follow-up period was 246 days (Q1/Q3 = 220.0/246.5). The mean age was 43.1 ± 10.1 (range, 27–61) years old, and the proportion of women was 83.7%. While all participants had received a third dose of BNT162b2 vaccine, 67.0% of participants had received a homologous booster (BNT162b2-BNT162b2-BNT162b2), and 33.0% had received a heterologous booster (ChAdOx1-ChAdOx1-BNT162b2) (Table 1). Out of these 43 HCWs, 19 (44.0%) were nurses, 13 (30.0%) were support staffs, and six (14.0%) were doctors.
Table 1
Demographic and clinical characteristics of the study subjects at baseline
Vaccine effectiveness for the omicron
Among the total 43 participants, 28 (65.1%) were confirmed to be infected with the SARS-CoV-2 virus. 18 were diagnosed in the Soonchunhyang Bucheon hospital and 10 in the public health center by performing COVID-19 PCR tests. The mean period from administration of the third dose to confirmation of the SARS-CoV-2 (presumed omicron variant) infection was 101.8 ± 30.0 days (mean ± SD). Among the SARS-CoV-2 (presumed omicron variant)-infected participants, nine (32.1%) had received a heterologous booster and 19 (67.9%) had received a homologous booster. There was no significant difference in effectiveness against the SARS-CoV-2 (presumed omicron variant) between the two booster regimens (P > 0.99). The number of infections within 120 days following the booster was 22 (78.6%). No cases of reinfection among the infected were identified.
All 28 participants infected with the SARS-CoV-2 (presumed omicron variant) had only mild symptoms. Half of them (14 of 28) did not receive any hospital care, and the other half improved with only outpatient treatment. No one presented with severe conditions such as admission to the ICU, acute respiratory distress syndrome (ARDS) or death in hospital.
Comparison of serology results between the omicron-infected and uninfected groups
Eight months after the third dose, the SARS-CoV-2 (presumed omicron variant)-infected group showed significantly higher sVNT inhibition than the uninfected group (P < 0.001) (Table 2). The median sVNT inhibition (%) scores were 30.7% (Q1/Q3 = 14.7/56.5) for uninfected subjects and 91.3% (Q1/Q3 = 80.5/96.2) for infected subjects. Presumed protective rates against SARS-CoV-2 (presumed omicron variant) was 90% in the infected group, which was significantly different than the 13% observed in the uninfected group (P < 0.001).
Table 2
Serology results 8 months after the third-dose (booster) vaccination
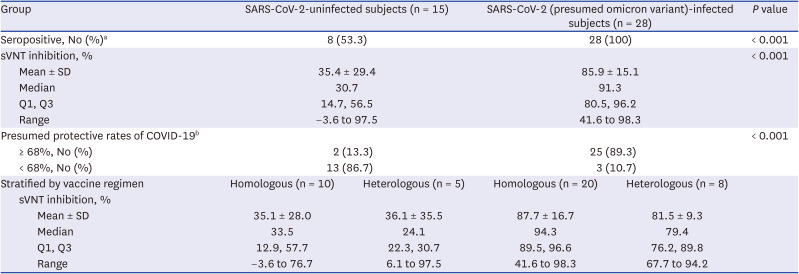
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, sVNT = surrogate virus neutralization test, SD = standard deviation, COVID-19 = coronavirus disease 2019.
aClassified as positive and negative with a 30% cutoff according to the guidelines defined in the GenScript SARS-CoV-2 sVNT kit.
bsVNT inhibition value ≥ 68% is suggested to indicate enough protection against COVID-19 infection.
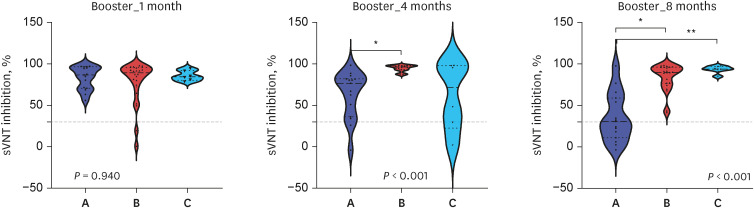
The SARS-CoV-2 (presumed omicron variant)-infected group was divided into two subgroups for further analysis, depending on whether they were infected within or after 120 days following administration of the third dose (booster vaccination). A month after the third dose (median, 28.0 days; Q1/Q3 = 26.5/28.0), no significant difference in sVNT inhibition was found between the SARS-CoV-2 (presumed omicron variant)-infected (median for ≤ 120 days, 89.3%, median for > 120 days, 84.4) and uninfected groups (median, 86.71%; P = 0.94) (Table 3, Fig. 1). Four months after receiving a third dose (median, 133.0 days; Q1/Q3 = 117.5/133.5), significantly higher sVNT inhibition values were observed in participants who were infected ≤ 120 days after administration of the third dose (mean ± SD, 94.6 ± 4.0%; median, 96.1%; Q1/Q3 = 93.0/97.8) than in the uninfected participants (mean ± SD, 63.0 ± 28.6%; median, 76.5%; Q1/Q3 = 43.6/81.8) and in participants who were infected more than 120 days after administration of the third dose (mean ± SD, 61.7 ± 41.3%; median, 71.6%; Q1/Q3 = 34.1/97.1) (P < 0.001). HCWs infected less than 120 days after booster vaccination and those infected more than 120 days after showed similar patterns, with sVNT inhibition rates lowered before infection and increased uniformly after infection.
Table 3
Comparison of serology results between SARS-CoV-2 (presumed omicron variant)-infected and uninfected subjects after third-dose (booster) vaccination
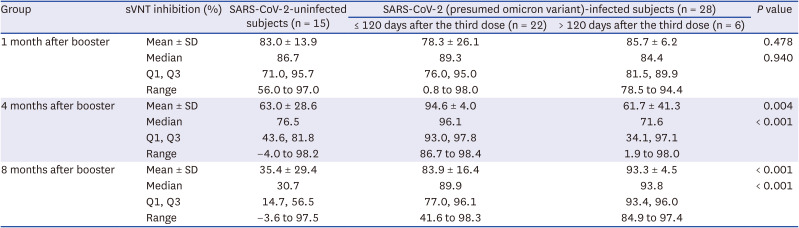
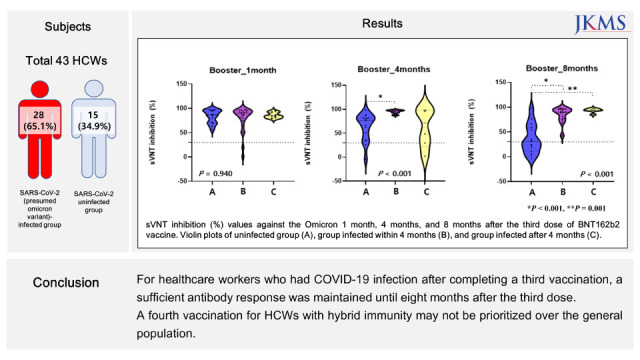
Fig. 1
sVNT inhibition (%) values against the omicron 1 month, 4 months, and 8 months after the third dose of BNT162b2 vaccine. Violin plots of uninfected group (A), group infected within 4 months (B), and group infected after 4 months (C). The P value at the bottom of each graph was found using the Kruskal–Wallis test.
sVNT = surrogate virus neutralization test.
Asterisks (*) indicate statistically significant differences between the compared groups (*P < 0.001, **P = 0.001).
The patterns of change across the three repeated measurements of sVNT inhibition values over the 8-month follow-up period after the third dose were compared between the infected and uninfected groups. For uninfected participants, the sVNT inhibition values notably declined over the study period, such that the value one month after the third dose (83.0 ± 13.9) was greater than the values four months (63.0 ± 28.6) and eight months (35.4 ± 29.4) after the third dose. For infected participants, the sVNT inhibition score remained stable over the study period, such that the score one month after the third dose (uninfected state) was similar to the score 136.6 ± 29.2 days after infection (85.9 ± 15.1 vs. 81.0 ± 20.5).
DISCUSSION
Omicron (B1.1.529) is a variant of SARS-CoV-2 first identified in South Africa on November 24, 2021.9 Omicron is currently prevalent worldwide and continues to mutate into subvariants. Since August 2021, booster or additional doses of vaccines have not been tailored to the new variants of SARS-Cov-2. Although many studies have shown that these vaccines are still helpful in reducing the severity of the disease,2101112 many still question the benefits of additional vaccinations in immune-competent people that had already received pre-existing vaccines.1314
The present study demonstrated that neutralizing antibody titers against the omicron after a third vaccine dose, measured by sVNT inhibition score, tended to gradually decrease over the 8-month follow-up period in healthy South Korean HCWs. However, it is worth noting that 79% of the infected group were infected within the four months following administration of the third dose, during which the immune protection was expected to be sufficient. In addition, the mean period from the third dose to infection in the infected participants was 101.8 ± 30.0 days, and the median value was 97.5 days (Q1/Q3 = 84.8/117.5), while the median follow-up period after the third dose was 246 days (Q1/Q3 = 220.0/246.5). This implies that most infections occurred within a relatively narrow time window, which may be attributable more to the widespread nature of the omicron variant in the community than to the subjects’ humoral immunogenicity at individual levels.
Our study also exhibited a rapid decline of neutralizing antibody % inhibition against omicron in uninfected participants at the 8-month of follow-up; however, the sVNT value tended to be stable in infected participants. The recent resurgence of COVID-19 in South Korea, which has a very high vaccine coverage rate,15 is mainly among previously uninfected individuals,16 and the second wave of the infection is likely to be due to decreased vaccine effectiveness over time. This result suggests the need for a fourth dose of vaccine, in line with previous evidence for the improvement of the SARS-Cov-2 antibody response after a booster dose in uninfected HCWs.17 However, the clinical and practical benefits of more than three doses of vaccine in terms of hybrid immunity, which is defined as the immune protection in individuals who have had one or more doses of a COVID-19 vaccine and experienced at least one SARS-CoV-2 infection before or after the initiation of vaccination, are still questionable.18
The sVNT inhibition score (94.6 ± 4.0, 93.3 ± 4.5) of those infected with SARS-CoV-2 (presumed omicron variant) were higher than the score measured one month after the third-dose vaccination (81.0 ± 20.5) (Table 3). Additionally, it was shown that the sVNT inhibition score of the infected participants remained around 85.9 ± 15.1 even after a mean follow-up period of 136.6 ± 29.2 days since infection (Table 2). This suggests that hybrid immunity might be superior to the current vaccine in terms of neutralizing antibody production capacity and durability. On the other hand, there is some opinion that vaccine induced immunity to omicron variant may be relatively low because current vaccines have been developed for the wild type.19 Future studies on the immunity generated after receiving a bivalent vaccine containing omicron variant antibodies will help to understand this. Our study followed up with participants for about four months after infection, but one epidemiological study in children and adolescents who were previously infected with SARS-CoV-2 has reported that natural immunity protected against re-infection for at least 18 months.20
Recently, interest in hybrid immunity has been increasing.21 Goldberg et al.22 showed that hybrid immunity in individuals who received a single dose of vaccine plus infection was associated with a level of protection similar to that of three doses of vaccine. Zar et al.23 suggested that hybrid immunity formed with one vaccine after infection, including omicron, produced stronger immunogenicity and protection than two doses in a naïve subject. An epidemiological study in Qatar showed that hybrid immunity is effective in preventing re-infection with COVID-19, including omicron, and that protection against severe outcomes such as hospitalization or death was strong regardless of the variants.24 From this point of view, our study included two groups: one with hybrid immunity from an infection after three doses and the other with vaccine induced immunity without previous infection. The degree and duration of immunity these patient groups exhibit against future omicron surges are yet to be known. In fact, as the number of people infected after vaccination or vaccinated after infection increases, research on hybrid immunity is expected to be helpful in planning future vaccination programs.
During the COVID-19 pandemic, most countries around the world have followed the guidelines of the WHO or countries with advanced healthcare systems. However, universal application of these guidelines to countries with different healthcare systems can be impractical and inefficient.25 As suggested by Cohen et al.,6 a fourth dose of vaccine for HCWs may prevent the decline in the effectiveness of the third dose and further outbreaks, thereby contributing to sustainable functioning of healthcare systems during the pandemic. From this point of view, the healthcare system has not been substantially disrupted by the pandemic thus far, and hybrid immunity has demonstrated its enduring protective effect; thus, it would be undesirable to recommend a fourth dose to all HCWs in South Korea.
This study has several limitations: 1) the study was conducted with a relatively small number of participants from a single institution, 2) each patient’s immunity was not comprehensively examined, and only humoral immunity was assessed due to cost and facility constraints, 3) the study did not consider subvariants of omicron as potential causes of secondary resurgence, and 4) neutralizing antibody titers were not directly measured, and sVNT inhibition score was utilized as an alternative. Despite these limitations, the present study addresses a timely and practical question about the necessity of a fourth booster vaccination for South Korean HCWs.
The sVNT inhibition (%) scores remained high until 8 months for subjects who had COVID-19 infection after completing a third dose, so a fourth vaccination for HCWs with hybrid immunity may not be prioritized over the general population. In order to cope with rapidly changing mutations, additional research on hybrid immunity as well as the development of customized vaccines will be needed.
 XML Download
XML Download