

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As coronavirus disease 2019 (COVID-19) spread, the World Health Organization (WHO) declared that the global crisis over the new coronavirus was a pandemic on March 11th, 2020.12 To prevent the spread of infection, lockdowns were implemented around the world.34 Lockdown due to COVID-19 has had several impacts in the field of orthopedics. The first is the disruption of routine protocols and usual treatment pathways in elective and emergency services. Second, medical accessibility of patients with chronic diseases such as osteoporosis was reduced. Third, the number of orthopedic trauma patients decreased. Therefore, the incidence of hip fractures in elderly, the management and clinical outcomes of these patients were inevitably affected in various aspects.5
Several studies already have investigated the changes of incidence, length of hospital stay (LOS), and mortality in hip fracture patients before and after the COVID-19 pandemic. However, these studies reported different results.67891011 These differences might be related with the proportion of COVID-19 patients, the severity of COVID-19 infection, and the difference in access to medical care due to lockdown among countries.391213 In addition, most studies were single-center short-term comparative research studies, which might have selection bias614 and might not reflect the changing patterns before and after the pandemic. To date, no study reported the effect of COVID-19 on hip fractures in a society where lockdown was not implemented.615 Since the COVID-19 outbreak in Daegu in February 2020, South Korea did not enforce a lockdown and only restricted large-scale rallies and demonstrations. Even though COVID-19 patients were isolated, there were no restrictions on the delivery of medical care service except for patients with fever and/or respiratory distress.
Therefore, we investigated whether COVID-19 changed the incidence rate (IR) of hip fracture, LOS and in-hospital mortality rate of hip fracture patients, and surgical treatment method of hip fractures in South Korea, where lockdown was not implemented.
METHODS
Study subjects
This retrospective nationwide study identified subjects from the Korean National Health Insurance Review and Assessment Service (HIRA) database from January, 2011 to December, 2020. HIRA collects data from claims submitted by healthcare providers for reimbursement under the nationwide healthcare insurance system, which covers the entire South Korean population.16 The information in the data set included all inpatient and outpatient medical claims data, including diagnostic codes and treatment procedure codes. Therefore, medical claims data for all hip fractures that occurred during the period from January 2011 to December 2020 in South Korea were identified.
Elderly hip fracture cohort
Eligibility criteria for elderly hip fracture patients were 1) admission to an acute care hospital (index admission) with diagnostic codes of femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fracture (ICD-10 S721); 2) undergoing typical surgeries, including internal fixation (open reduction, closed pinning), hemiarthroplasty, total arthroplasty, or conservative treatment (hip spica splint, traction); and 3) age > 65 years at the time of hip fracture. Incidence date (index date, time zero) of hip fracture was defined as the date of admission to the acute care hospital that fulfilled eligibility criteria. Subsequent hip fracture was defined as a fracture that occurred at least 6 months after the index date (6-month washout period).
Statistical analysis
The IR was defined as the total number of newly diagnosed hip fractures in a year divided by the mid-year population. IRs were expressed as the number of hip fractures per 100,000 person-years. A generalized estimating equation model with Poisson distribution and logarithmic link function was used to estimate adjusted annual percent change (APC) of incidence rate and 95% confidence intervals (CIs). Using claims data from 2011 to 2019, APC in events, such as incidence rates of hip fracture and mean LOS, were investigated and expected values (counterfactual) for 2020 were estimated. Afterwards, the relative differences between counterfactual and observed 2020 values were estimated (interrupted time series analysis).
Baseline characteristics were identified at time zero. Included covariates were age group, sex, residential area, Charlson Comorbidity Score (CCS), fracture type, surgery and anesthesia, LOS, presence of preoperative admission in long-term care hospital, and calendar year of the hip fracture. Each subject’s number of comorbidities was assessed by diagnostic codes during 3 years before the time zero using the Quan ICD-10 coding algorithm of the CCS.17 The presence of CCS disease-constituting categories was defined by at least 2 outpatient visits or 1 admission upon the primary or first secondary diagnosis. All statistical analyses were conducted using SAS Enterprise Guide version 7.15 (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant.
RESULTS
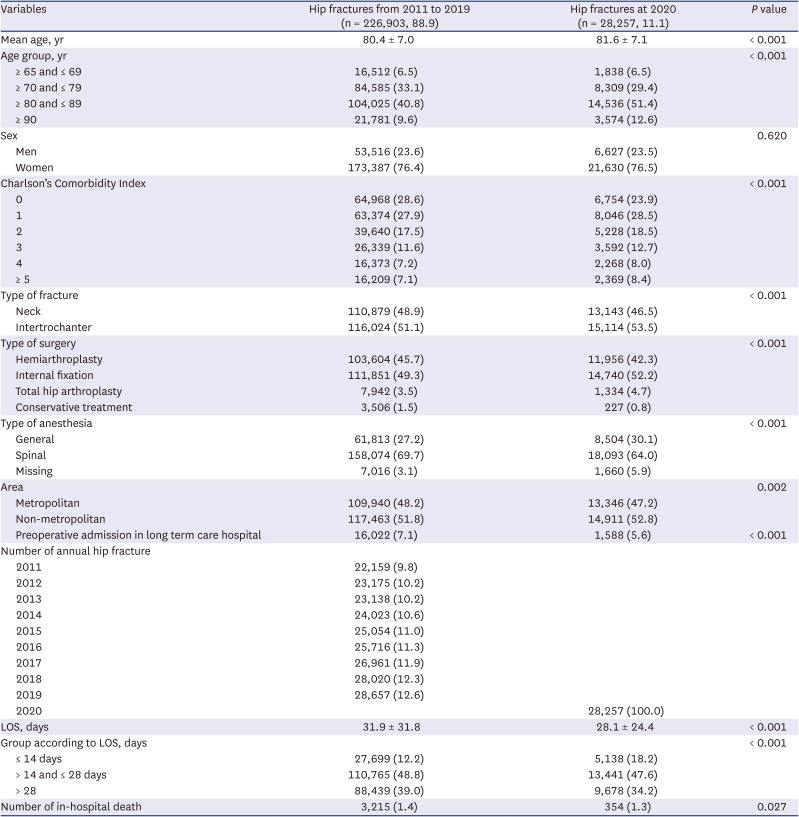
From January 1, 2011 to December 31, 2020, 310,444 patients were hospitalized for hip fractures. Of these, 54,735 patients were excluded (21,328 patients for previous cancer history, 33,407 patients were under 65 years of age). This left 255,709 elderly hip fracture patients, which were subjects of this study. These patients were divided into 2 groups: 226,903 (88.9%) in the pre-COVID hip fracture group (pre-COVID group: hospitalized from 2011 to 2019) and 28,257 (11.1%) in the COVID hip fracture group (COVID group: hospitalized in 2020) (Table 1).
Table 1
Demographic factors for included patients
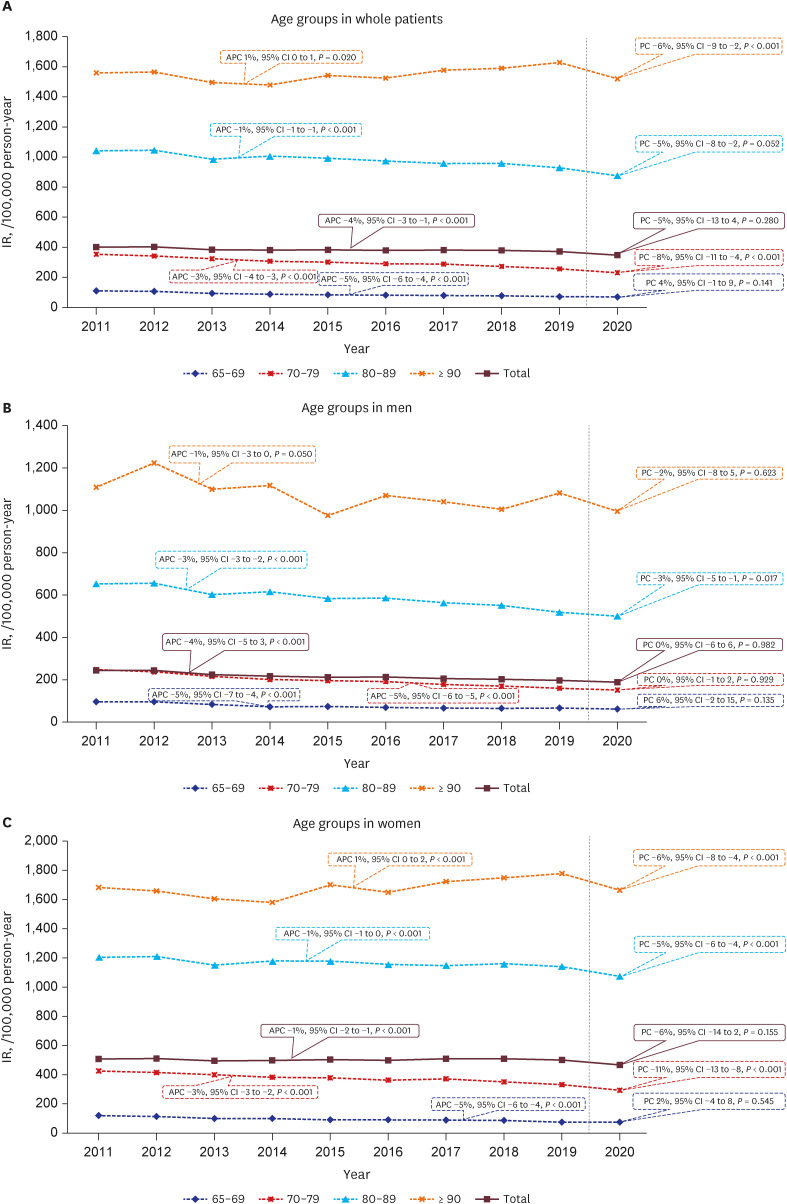
The IR of hip fractures in 2020 was smaller by 5% (percent change [PC], −5%; 95% CI, −13 to 4; P = 0.280) than the expected IR considering the trend in the annual IRs of hip fractures from 2011 to 2019 (APC, −4%; 95%CI, −3 to −1, P < 0.001), but the difference was not statistically significant (Fig. 1A, Supplementary Table 1). However, in the subgroup-analysis by age, the hip fracture IR in 2020 was smaller by 8% (PC, −8%; 95% CI, −11 to −4; P < 0.001) in the 70–79 year group and by 6% (PC, −6%; 95% CI, −9 to −2; P < 0.001) in the ≥ 90 year group than the expected values. In the 80–89 age group, the hip fracture IR in 2020 was smaller by a marginal significance (PC, −5%; 95% CI, −8 to −2; P = 0.052). In men, only the 2020 IR in the 80–89 year group was smaller by 3% than the predicted value (P < 0.05). In women, the 2020 IRs in all age groups over 70 years were smaller than the predicted value (P < 0.05) (Fig. 1B and C).
Fig. 1
These graphs show the results of interrupted time series analysis for annual IRs of hip fractures according to age (A) and sex (B, C).
IR = incidence rate, APC = annual percentage change, PC = percentage change, CI = confidence interval.
The annual in-hospital mortality rate decreased from 2011 to 2019 (APC, −5%; 95% CI, −6 to −3; P < 0.001). However, the in-hospital mortality rate in 2020 was insignificantly larger (PC, 5%; 95% CI, −8 to 19; P = 0.461) than the expected value (Fig. 2A, Supplementary Table 2).
Fig. 2
These graphs show the results of interrupted time series analysis for annual in-hospital mortality rates (A) and mean LOS in hip fractures (B).
LOS = length of hospital stay, APC = annual percentage change, PC = percentage change, CI = confidence interval.
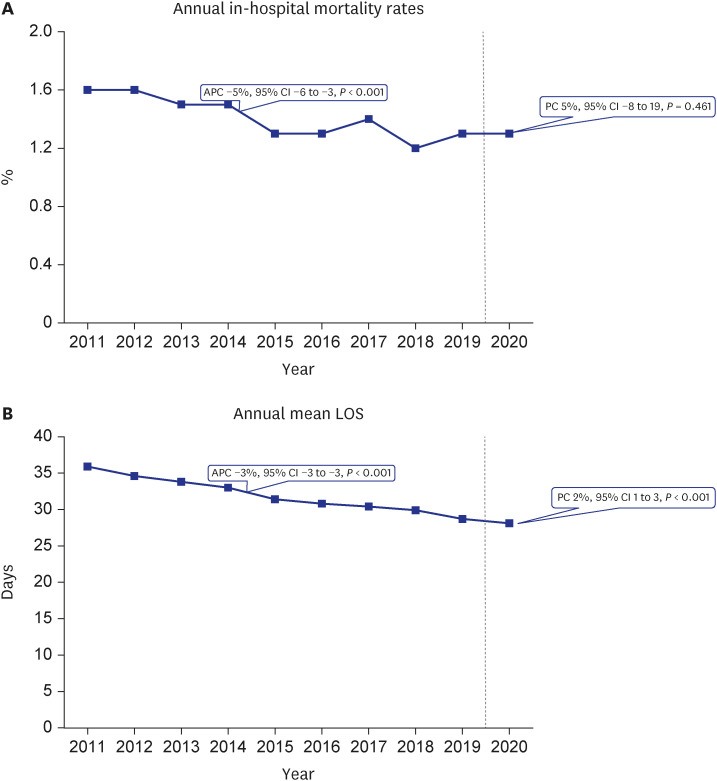
The annual mean LOS decreased from 2011 to 2019 (APC, −3%; 95% CI, −3 to −3; P < 0.001). The mean LOS in 2020 was larger by 2% (PC, 2%; 95% CI, 1 to 3; P < 0.001) than the expected value (Fig. 2B, Supplementary Table 2).
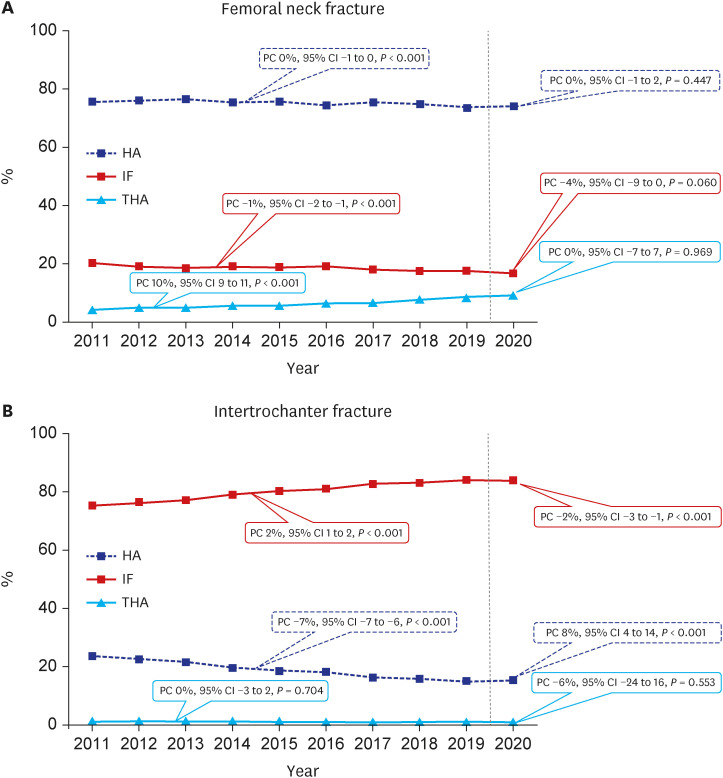
The changes in the proportion of surgery type in femoral neck fracture in 2020 did not differ from the predicted values considering the changes in the pre-COVID period (P > 0.05) (Fig. 3A, Supplementary Table 3). However, among the surgery type in 2020 for intertrochanteric fractures, the proportion of internal fixation was smaller by 2% (PC, −2%; 95% CI, −3 to −1; P < 0.001) than the predicted value, and the proportion of hemiarthroplasty was larger by 8% (PC, 8%; 95% CI, 4 to 14; P < 0.001) than the predicted value.
Fig. 3
These graphs show the results of interrupted time series analysis for annual proportions of surgery type in femoral neck fracture (A) and intertrochanter fracture (B).
HA = hemiarthroplasty, IF = internal fixation, THA = total hip arthroplasty, PC = percentage change, CI = confidence interval.
DISCUSSION
In this study, we evaluated the effect of COVID-19 on elderly hip fractures in South Korea where lockdown restriction was not implemented. We observed the following findings. First, the IR of hip fractures did not decrease in 2020. However, in women over 70 years of age, the hip fracture IR notably decreased. Second, in 2020, there was no increase in in-hospital mortality rate, but a 2% increase in LOS. Third, in 2020, there was no significant change in the proportion of surgical methods for femoral neck fractures, but proportion of internal fixation decreased, and proportion of hemiarthroplasty increased for intertrochanteric fractures.
The rise in the psychological distress level caused by the COVID-19 outbreak is a phenomenon that occurs anywhere in the world.181920 Lockdown along with this COVID-19-related fear and anxiety restricted physical activities as well as health care access of the elderly.3 This may exacerbate chronic medical conditions and may affect the incidence of hip fractures. However, there is disagreement as to whether the incidence of hip fracture is reduced even in studies analyzing data that can be representative of the population. In the analysis of hip fracture patients over 60 years of age registered in the National Hip Fracture Database, Johansen and Inman12 confirmed that the incidence of hip fracture reduced in some units but not in the pooling data. da Silva et al.9 found that the incidence of hip fracture patients over 60 years of age decreased in 2020 compared to 2019 in the analysis of the Brazilian public health care system. Brent et al.8 reported that hip fracture incidence in 2020 decreased by 15% compared to that in 2019 in the analysis of the Irish Hip Fracture Database. Because the lockdown period differed in each country and there are differences in ethnic, region and medical policy, the various results of these studies should not be simply compared and should not be interpreted as general trends in COVID pandemic. Because prior studies simply compared hip fracture incidence between 2019 and 2020, and they did not consider the past trend in hip fracture incidence, it seems inappropriate to conclude that the IR of hip fracture decreased after COVID pandemic.
This is the first study to report that there was no significant change in elderly hip fracture incidence in during the COVID pandemic in a country where lockdown was not implemented.
In this study, we compensated for shortages of previous studies by comparing actual IR of elderly hip fractures during the pandemic with projected IR based on IRs of pre-COVID-19 period. Our findings are similar to those of previous studies which reported that the incidence of low energy trauma did not decrease during the COVID-19 pandemic.122122 Even in the pandemic period of an infectious disease, sufficient medical resources should be spared for are used for hip fracture patients as well as infection patients.
Hip fractures are associated with high morbidity and mortality rates.6 A notable finding in our study was that hip fracture incidence was lower in women than in men in age groups over 70 years. This gender difference could be explained by that male hip fracture patients have more comorbidities and a higher average American Society of Anesthesiologists classification than their female counterparts.23 Therefore, in our study, the incidence of male hip fracture patients did not decrease significantly considering the past incidence trend, which is thought to be because male hip fracture occurs in more ill patients at a high risk of hip fracture. da Silva et al.,9 reported that the incidence of hip fracture during the COVID-19 pandemic was markedly decreased in the southeast region of Brazil with a high proportion of female population, and that the incidence of hip fracture in women especially decreased. Pieh et al.24 investigated gender-specific mental health and physical activity during the COVID-19 pandemic period and reported that women had poor mental health status such as depression, anxiety, and insomnia, which was associated with low physical activity.22 Visser et al.25 noted that fear of infection in older adults during the COVID-19 pandemic period reduced their daily activities. Pluskiewicz et al.22 reported that low physical activity could reduce the incidence of osteoporotic fractures. Therefore, it is considered that the decrease in physical activity caused by COVID-19 occurs particularly clearly in women over 70 years of age, and the incidence of hip fracture might decrease.
Reportedly, the mortality rate in COVID-19 negative hip fractures patients varied from 7.1–53.6%.212627 In addition, comparative studies of mortality rates of hip fracture with COVID-19 negative before and after the COVID-19 pandemic reported no significant increase in the mortality rate.813
Ultimately, the most important factor influencing the mortality rate of hip fracture patients during the COVID-19 pandemic period seems to be the presence and severity of COVID-19 infection. Among the hip fracture patients included in our study, there were few COVID-19 positive patients, and the in-hospital mortality did not change significantly after the pandemic.
In our study, the LOS increased by 2% contrary to the decrease of LOS in studies from other countries.7212829 This is probably because South Korea’s quarantine policy to actively detect infected patients might have reduced the fear COVID-19 could be transmitted during the hospitalization.
In our study, the proportion of internal fixation in the treatment of femoral neck fracture did not change. When considering the choice of surgical method in elderly patients with femoral neck fracture, the type of fracture is most important. Because these patients require early weight bearing after the operation, internal fixation is indicated in limited situations such as non-displaced or valgus impacted fractures. The internal fixation is simpler and less time consuming than hip arthroplasty and if indicated, surgeons choose the internal fixation irrespective of COVID-19.
On the other hand, among the surgical treatment methods for intertrochanteric fracture patients, the proportion of hemiarthroplasty increased, and the proportion of internal fixation decreased during the COVID-19 period. In a comparative study between surgical methods for unstable intertrochanteric fractures, Tu et al.30 reported that although hemiarthroplasty requires more operation time and more intraoperative blood loss than internal fixation, patients could ambulate earlier and had less implant related complications. In a meta-analysis for the clinical results after hemiarthroplasty versus internal fixation in intertrochanteric fractures, hemiarthroplasty had lower rates of failure and reoperation.31 In our study, hemiarthroplasty was performed more frequently during the pandemic than before. This trend might be related with the wide use of hemiarthroplasty in the intertrochanteric fracture.3031
There are several limitations in this study. First, since only claims data from 2011 to 2020 could be obtained, long-term changes could not be analyzed. Second, because the number of hip fracture patients with COVID-19 was too small, we could not analyze the mortality rate of hip fracture patients with COVID-19.
In 2020, the IR of hip fractures did not decrease significantly, and in-hospital mortality rate did not increase significantly compared to the expected rates, which were projected based on the HIRA hip fracture database from 2011 to 2019. Only LOS increased slightly.
 XML Download
XML Download