

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mild cognitive impairment (MCI) refers to a cognitive syndrome presenting with subjective memory complaints by the patient or caregiver and with documented objective cognitive impairment for the individual’s age and education level.1 In particular, amnestic MCI (aMCI) is diagnosed when the main manifestation is memory impairment. aMCI is considered the prodromal stage of dementia caused by Alzheimer’s disease (AD).2 Although clinical trials for AD treatment have been previously conducted in patients with mild-to-moderate dementia, they have gradually shifted to target patients in earlier stages. Therefore, early and appropriate diagnosis of aMCI is clinically important.
aMCI is diagnosed on the basis of objective cognitive impairment documented through neuropsychological (NP) tests. Clinicians and researchers prefer NP tests that are sufficiently sensitive and take as little time as possible to distinguish patients with MCI from individuals with subjective cognitive decline (SCD) or dementia. However, most of the conventional cognitive tests have several limitations. Screening tests such as the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) can be performed in a short time, but their specificity for diagnosing MCI is low. On the other hand, while comprehensive NP tests, such as the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) test and the Alzheimer’s Disease Assessment Scale Cognitive Section (ADAS-cog), are the gold standard for identifying object memory impairment in aMCI and provide scores for each cognitive domain in relation to the patient’s age and level of education, they take a long time. Therefore, participants are often exhausted by the time they complete the test.
Another issue with conventional NP testing is that it is mostly based on pencil-and-paper tests. Therefore, these tests require expert examiners and a longer time to score and report the test results. In addition, pencil-and-paper tests offer only the final score and show limitations in monitoring the participants’ reaction time and cognitive processes in producing the final score. The digital version of NP tests, on the other hand, can address these issues and can potentially be used in telemedicine and may be coupled with future digital devices.34 A previous study described the Inbrain Cognitive Screening Test (Inbrain CST), a tablet computer-based NP test that can be administered within 30 minutes and can generate not only the total score but also cognitive domain scores.5 It could also discriminate among SCD, MCI, and dementia stages with verified test-retest reliability and showed a significant correlation with the results of a comprehensive NP test called the Seoul Neuropsychological Screening Battery (SNSB), which usually takes 1 to 2 hours. Additionally, in a large-scale study investigating the cognitive function improvement effect of cognitive training, the Inbrain CST was shown to be useful for follow-up assessments.6 However, the diagnostic performance of this test in differentiating aMCI from cognitively unimpaired has not been evaluated. Therefore, in this study, we investigated the performance of the Inbrain CST in diagnosing aMCI and compared its performance to that of the Korean version of CERAD test (CERAD-K), a comprehensive and pencil-and-paper NP test.
METHODS
Participants
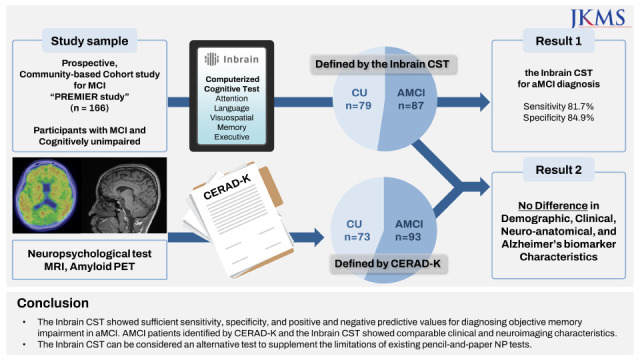
A total of 166 participants were included in this cross-sectional study. The participants were recruited as part of a prospective, community-based cohort study for MCI (PREcision medicine platform for mild cognitive impairment on multi-omics, imaging, evidence-based R&BD; PREMIER) and had visited the Center for Dementia in Gangnam, Bucheon, Incheon, Dongtan, Gijang, Dongtan, or Haewoondae, South Korea. Individuals who were cognitively unimpaired (CU) or had aMCI were included in the PREMIER cohort. The Centers of Dementia are public facilities that focus on integrated dementia management by providing services, including early screening, dementia prevention education, cognitive rehabilitation programs, and treatment support. All participants were assessed using the CERAD-K, which is a comprehensive NP test. Experienced neurologists reviewed all clinical information about the participants and divided them into CU and aMCI groups.
The criteria for CU were as follows: 1) normal cognitive function defined by all the scores of the four episodic memory tests (word list memory, word list recall, word list recognition, and constructional praxis recall tests) in the CERAD-K above −1.5 standard deviation (SD) of the age, sex, and education-based norm78; and 2) normal activities of daily living with or without subjective memory complaints.
The criteria for aMCI, which were based on Pertersen’s criteria,1 were as follows: 1) memory complaint corroborated by an informant; 2) objective memory impairment relative to age, education, and sex; 3) essentially preserved general cognitive function; 4) largely intact functional activities; and 5) no dementia. Objective memory impairment was defined by a performance score of 1.5 SD below the respective age-, education-, and sex-specific normative means for at least one of the four memory scores of episodic memory tests included in the CERAD-K NP battery, namely word list memory, word list recall, word list recognition, and constructional praxis recall tests.78 Of all the 166 participants, 162 underwent apolipoprotein genotyping, and a review of past medical history was missing in one participant due to follow-up loss.
Tablet computer-based CST
The Inbrain CST was administered on a 12-inch tablet PC running Microsoft Windows 10. It consists of seven neuropsychological tests assessing five cognitive functions: the Visual Span Test included forward and backward tasks used to assess attention; the Difficult Naming Test and semantic (fruits)/phonemic (Korean alphabet digeut) word fluency test assessed language; the Block Design Test assessed visuospatial function; the time orientation questions and Word Place Association Test assessed memory; and the Korean-Trail Making Test-Elderly version evaluated executive function. Age-, education-, and sex-specific normative values for each cognitive domain were provided by the manufacturer based on a previous study of 480 cognitively normal, community-dwelling, older adults.5
Measurement of hippocampal volume and cortical thickness on magnetic resonance imaging (MRI)
Seventy-six participants (61 aMCI and 15 CU) underwent brain MRI scans. T1-weighted MRI scans were obtained on a 3.0 T magnetic resonance scanner (Siemens Skyra, Siemens Medical Solutions, Erlangen, Germany), and high-resolution anatomic magnetization-prepared rapid gradient-echo images were obtained with the following parameters: sagittal slice thickness, 1.0 mm with 16.7% overlap; no gap; repetition time, 2,300 ms; echo time, 2.01 ms; flip angle, 9°; 1-mm isotropic voxels; and 192 slices. Image processing was performed using FreeSurfer 5.1.0 (Athinoula A. Martinos Center at the Massachusetts General Hospital, Harvard Medical School; http://surfer.nmr.mgh.harvard.edu/). First, we constructed the cortical surface and the outer and inner surface meshes. The outer and inner meshes were isomorphic and identical in terms of connectivity and height. We adopted the manifold harmonic transform (MHT) to map the cortical thickness from the surface onto the frequency domain to remove noise.910 The high-frequency components of the transformed cortical thickness were regarded as noise by the MHT and were eliminated. This filtering of high-frequency components can remove noise and reduce the dimensionality of cortical thickness. For normalization, hippocampal and parahippocampal volumes were calculated as the sum of the right and left hippocampal or parahippocampal volumes divided by the estimated total intracranial volume. AD signature cortical thickness was measured as the average volume of the cortical thickness in the regions of interest: entorhinal, inferior temporal, middle temporal, and fusiform (summation of cortical thickness ROIs/8).11
Amyloid positron emission tomography (PET) scans
Of the participants who were enrolled through the seven centers (see Participants section), all 76 patients who visited the Bucheon center underwent amyloid PET-computed tomography (CT) scans, which involved [18F]-flutemetamol imaging using a Biograph 128mCT unit (Siemens Medical Solutions, Knoxville, TN, USA). Ninety minutes after a bolus injection of 370 MBq [18F] flutemetamol, the patients underwent a low-dose CT scan followed by a 20-minute (i.e., four frames of 5 minutes) PET scan. The scans were carefully checked for movement, and frames were summed to acquire a static (20-minute) image for each patient. The scans were visually examined and dichotomously assessed as either amyloid-positive or amyloid-negative by a nuclear medicine specialist who had undergone a training program for visual interpretation of [18F] flutemetamol images.
Statistical analysis
We evaluated the diagnostic performance of the Inbrain CST for identification of aMCI by comparing the findings with those of CERAD-K. Considering the diagnosis of aMCI based on CERAD-K as the gold standard, we assessed the overall accuracy, sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios of the Inbrain CST. Statistical analyses were performed using the Rex package (Rex: Excel-based statistical analysis software, version 3.0.3; RexSoft Inc., Seoul, Korea) and R (version 3.6.0; R Foundation for Statistical Computing, Vienna, Austria). Sensitivity/specificity, positive/negative likelihood ratios, positive/negative predictive values, overall accuracy, and 95% confidence intervals (CIs) were estimated. Sensitivity and specificity were compared using the McNemar test, whereas positive/negative likelihood ratios were compared with a regression model approach, and positive/negative predictive values were compared with a generalized score statistic, all of which were implemented in the Rex package. We determined the characteristics of aMCI patients as defined by CERAD-K and the Inbrain CST. The clinical and neuroimaging variables of the two groups were statistically compared using Rex software. Group comparisons were performed using t-tests for continuous variables and χ2 tests for categorical variables.
RESULTS
Clinical characteristics of the participants
Of the 166 participants, 93 were diagnosed with aMCI while 73 were CU. The average age of the aMCI group was 77.02 years, and the average number of years of education was 6.46 years. Thirty-six of the 162 participants (22.2%) were apolipoprotein E ε4 carriers, including 22/90 (24.4%) participants with aMCI, and 14/72 (19.4%) CU participants. Amyloid PET scans revealed positive results in 52/76 (68.4%) of the total participants, including 46/61 (75.4%) of those with aMCI and 6/15 (40.0%) CU participants (Table 1).
Table 1
Clinical characteristics of aMCI defined by different neuropsychological tests
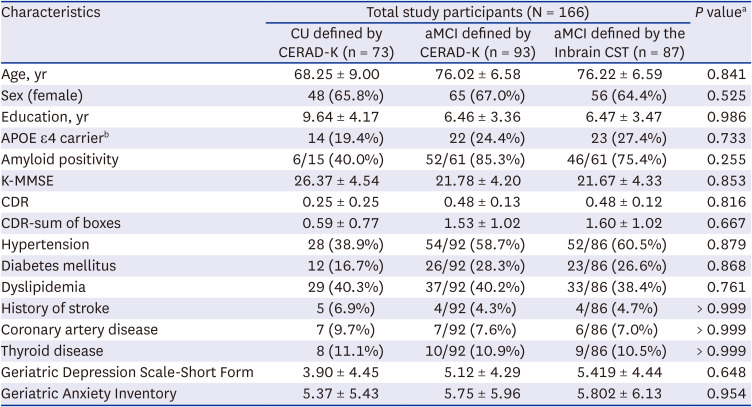
Data are expressed as mean with standard deviation or number with percentages in parentheses.
CU = cognitively unimpaired, aMCI = amnestic mild cognitive impairment, CERAD-K = Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease test, CST = cognitive screening test, K-MMSE = Korean version of the Mini-Mental State Examination, CDR = Clinical Dementia Rating.
aaMCI defined by CERAD vs. aMCI defined by Inbrain CST.
bThe apolipoprotein E genotyping was conducted in 138 participants.
Diagnostic performance of CST for aMCI in comparison with that of CERAD-K
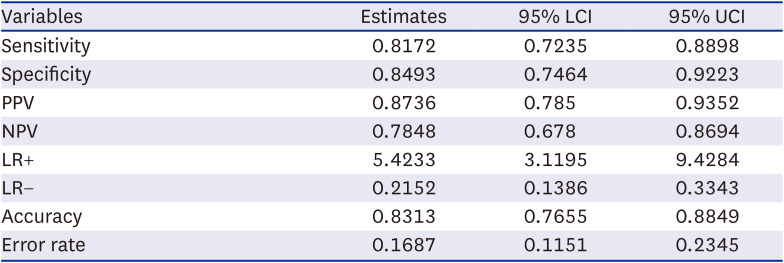
When objective memory impairment was defined as an Inbrain CST memory domain score of less than −1.0 SD of the reference scores for the same age and years of education, the sensitivity of the Inbrain CST for aMCI diagnosis was 81.7%, and its specificity was 84.9%. Positive and negative predictive values were 87.4% and 78.5%, respectively (Table 2), and the positive and negative likelihood ratios were 5.4233 and 0.2152, respectively. The diagnostic accuracy was 83.1%, and the error rate was 16.9%.
Table 2
Diagnostic performance of the Inbrain CST for identifying aMCI
Comparison of clinical and neuroimaging characteristics between individuals with aMCI defined by CST and CERAD-K
The clinical and neuroimaging characteristics of 93 patients with aMCI as defined by the CERAD-K and 87 patients with aMCI as defined by the Inbrain CST were compared (Table 1). Age, sex, education, APOE e4 carrier status, amyloid positivity, MMSE score, clinical dementia rating (CDR), CDR-sum of boxes (CDR-SB), depression and anxiety scale score, and underlying medical conditions were not significantly different between the two groups. Among participants who underwent brain MRI, the hippocampal and parahippocampal volumes and AD signature cortical thickness, which can be considered neuroimaging biomarkers of AD, were not different between the two groups (Table 3).
Table 3
Neuroimaging characteristics of aMCI defined by different neuropsychological tests

Neuroimaging results were available for 76 patients that comprised 61 MCI and 15 CU participants. Data are expressed as the mean ± standard deviation.
aMCI = amnestic mild cognitive impairment, CERAD-K = Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease test, CST = cognitive screening test, eTIV = estimated total intracranial volume, AD = Alzheimer’s disease.
We obtained amyloid PET in 76 participants (61 aMCI and 15 CU), and 52 participants showed positive scans. Among the 61 patients with aMCI defined by CERAD who underwent amyloid PET, 52 (85.3%) showed amyloid positivity. In aMCI defined by the Inbrain CST group, 61 patients had amyloid PET and 46/61 (75.4%) revealed positive results. Only four of the participants with amyloid PET positivity had discrepant diagnosis; two patients were diagnosed with aMCI only by the Inbrain CST, while the other two were diagnosed with aMCI only by CERAD-K. The results of two diagnostic tests were congruent for the remaining 48 patients (46 aMCI, 2 CU).
DISCUSSION
In this study, CERAD-K was used as the gold standard NP test to define objective memory impairment, and the Inbrain CST showed adequate sensitivity and specificity for diagnosing aMCI. The validity and test-retest reliability of the Inbrain CST have been proven in a previous study,5 and this test has been used as a follow-up tool in a large-scale clinical trial for a cognitive intervention.6 Therefore, it can be considered useful for diagnosis and follow-up of aMCI.
The Inbrain CST, a tablet-based NP test, takes 30 min to complete, requiring less time than comprehensive pencil-and-paper-based NP tests that can take more than an hour. For instance, participants are required to concentrate on the tests for 30–40 minutes in CERAD-K and for 1.5–2 hours in SNSB. In addition, unlike test batteries that require a skilled examiner, even a less experienced accessor can perform the examination according to the voice/screen instructions installed in the Inbrain CST. The post-test workload is also lower because the scores and percentiles for each cognitive domain are automatically calculated. This digital assessment system can be used online, and the virtual cognitive assessment can be especially beneficial in situations such as the coronavirus disease pandemic. Taken together, these findings indicate that the Inbrain CST has potential to be used by public health institutions nationwide.
The Inbrain CST also has several strengths with regard to test reliability and accuracy. The accuracy of the Inbrain CST for detecting aMCI was 83% in comparison with that of CERAD-K. In the Inbrain CST validation study that has been previously reported,5 the Inbrain CST differentiated aMCI from SCD with a sensitivity of 0.808 and a specificity of 0.762, which are comparable to our findings of sensitivity and specificity of 0.817 and 0.849, respectively. The accuracy of a cognitive test for detecting cognitive impairment is essential, because differentiating aMCI from CU depends on the presence of objective cognitive dysfunction. As the diagnostic performance of the Inbrain CST was comparable to that of CERAD-K, the Inbrain CST can be considered a cost-effective approach.
The frequencies of amyloid positivity were comparable between the patients with aMCI defined by Inbrain CST and those with aMCI defined by CERAD-K (46/61 [75.4%] for aMCI defined by the Inbrain CST vs. 52/61 [85.3%] for aMCI defined by CERAD-K). Among the 52/72 participants with a positive result on amyloid PET scans, each of the two tests, CERAD-K and the Inbrain CST, defined 46/52 patients as aMCI. The diagnosis of aMCI versus CU using the Inbrain CST and CERAD-K was congruent in all except four participants; two were diagnosed as aMCI by CERAD-K but CU by the Inbrain CST, while the other two were vice versa. These findings suggest that the Inbrain CST is also considerably effective in detecting aMCI due to AD confirmed by the biomarker, amyloid PET scan. These agreements between the tests, despite the shorter length of the Inbrain CST, may be partly attributable to the fact that the memory task in the Inbrain CST is based on associative memory that binds item and place information. This association is known to be related to the functioning of the hippocampus and medial temporal lobe,12 which are the most vulnerable and initially affected areas in AD.13
The participants who underwent amyloid PET scan in our study were 76.1-years-old on average, and the amyloid positivity was 68.4%, which is relatively higher than the reported frequency.1415 Even 6 of 15 (40.0%) CU participants also showed positive amyloid scans. Although this study is a prospective and community-based cohort study, we recruited participants from the centers of dementia across South Korea who volunteered for dementia evaluation; thus, these participants might have had more cognitive concerns than the general population. In other words, we cannot completely rule out the possibility that our CU participants had SCD, and the amyloid positivity of SCD defined by amyloid PET scan was reported as 10–76% at age 70 years.1617 Our recruitment setting might also have affected the higher than expected amyloid PET positivity among the patients with aMCI. Moreover, because the diagnosis of MCI was defined using rather stringent criteria, i.e., scores of memory tasks lower than -1.5 SD by CERAD, the frequency of positive amyloid PET scan might have been higher than in previous reports where the objective memory impairment was set at −1.0 SD.
In our study, aMCI was defined as an Inbrain CST memory score less than −1.0 SD relative to the participant’s age and education and a CERAD-K memory score less than −1.5 SD. Currently, the cut-off values for the normal range when defining objective memory dysfunction in NP tests vary among NP batteries and cohort studies. CERAD-K adopted a threshold of −1.5 SD relative to the individual’s age, education level, and sex,7 while SNSB adopted a threshold of −1.0 SD relative to the participant’s age and education, as previously reported in a nationwide Clinical Research Center for Dementia of South Korea (CREDOS) study.18 In the ADNI cohort, MCI was defined as abnormal memory function documented by delayed free recall of Story A from the Wechsler Memory Scale Revised Logical Memory II subtest. Assignment of either early or late MCI was based on scores below −1.5 SD or from −1.5 to −1.0 SD, respectively.19 When the researchers set the cut-off value of significant memory deficit for diagnosis of aMCI, the balance between the sensitivity and specificity shifted based on whether they adopted values 1.0 to 2.0 SD below the norm.20 The progression rate, biomarker, and functional status differed between the early and late MCI.212223 Considering the importance of detecting MCI patients for prevention of dementia progression, the establishment of the cut-off as −1.0 SD, as in Inbrain CST, can be considered appropriate in terms of surveillance of MCI.
In conclusion, the Inbrain CST showed sufficient sensitivity, specificity, positive and negative likelihood ratios, and positive and negative predictive values for diagnosing objective memory impairment in aMCI. In addition, the clinical and neuroimaging characteristics of patients identified as showing aMCI on the basis of CERAD-K and the Inbrain CST were similar. Therefore, the Inbrain CST can be considered an alternative test to supplement the limitations of existing pencil-and-paper NP tests.
 XML Download
XML Download