

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epidemiological studies have suggested particulate matter as an environmental risk factor for accelerated cognitive decline1 and dementia,2 which may be attributed to brain cortical atrophy and/or cerebral small-vessel disease. A growing body of studies have demonstrated the effects of particulate matter exposures on brain imaging markers such as white matter hyperintensities (WMH),34 cortical volume,567 and cortical thickness.89
It is now established that chronic systemic inflammation plays a key role in the neurotoxicity of particulate matter,10 but there is scarce evidence on whether chronic systemic inflammation modifies the effect of particulate matter exposure on brain imaging markers. A study demonstrated that higher long-chain omega-3 polyunsaturated fatty acid (which has anti-inflammatory properties) attenuated the effect of particulate matter exposure on total white matter volume.11 This finding is important because chronic systemic inflammation has a potential to be a target in preventing the neurotoxicity of particulate matter exposure.
C-reactive protein (CRP), an acute-phase protein, is a marker of chronic low-grade systemic inflammation.1213 Some studies have demonstrated that individuals with higher CRP level are at a greater risk of a decline in heart rate variability (as a proxy for dysfunction of the autonomic nervous system) associated with particulate matter exposure, as compared with those with lower CRP level.1415 This is aligned with that the key mechanism behind the cardiovascular effect of particulate matter is chronic inflammation,16 which is also one of the mechanisms behind the neurotoxic effect of particulate matter.10 However, no study so far has focused on CRP as an effect modifier of the association between particulate matter exposure and the central nervous system.
Hence, the present study aimed to investigate whether CRP level modifies the effects of particulate matter exposures on brain imaging markers (cortical thickness and WMH).
METHODS
Study participants
This cross-sectional study was embedded in a multi-center community-based cohort study, the Environmental Pollution-Induced Neurological EFfects (EPINEF) study. Fifty-year-old or older adults dwelling in four cities (Seoul, Incheon, Wonju, and Pyeongchang) in the Republic of Korea were recruited via local advertisements. The survey centers were located in Seoul, Incheon, and Wonju (covering Pyeongchang as well). All participants did not report any history of dementia, movement disorder, or stroke. We used a standardized survey protocol, which consisted of questionnaires, anthropometric and blood pressure measurements, blood tests (with ≥ 12-hour fasting blood samples), and the Mini-Mental State Examination (MMSE). Further details of the survey protocol were described elsewhere.17 A total of 1,711 individuals signed up to participate in the EPINEF study during the baseline survey period between August 2014 and March 2017. According to their enrollment order, participants were asked to undergo brain 3 Tesla magnetic resonance imaging (MRI) scans (n = 998). After excluding those with missing values, data from 874 participants were used in this study. These study participants had significantly higher education levels and PM concentrations compared with those who did not undergo brain MRI scans, but mean age and MMSE score did not significantly differ (Supplementary Table 1).
Particulate matter exposures
We used national prediction data constructed by universal kriging modelling of particulate matter regulatory monitoring data between 2001 and 2016, using 322 geographic variables (classified as demographic characteristics, land use, physical geography, transportation facilities, emissions, vegetation, altitude, and traffic variables).18 The universal kriging model was composed of mean component (including summary predictors estimated by partial least squares of 322 geographic variables) and variance component (considering spatial correlation, spatial variability, and nonspatial variability). These prediction data were linked to the survey data on the basis of each participant’s residential address. The median duration of residence was 15 years. The level of exposure to particulate matter ≤ 10 µm in diameter (PM10) was defined as a five-year average concentration of PM10 prior to the year of enrollment. The level of exposure to particulate matter ≤ 2.5 µm in diameter (PM2.5) was defined as a one-year average concentration of PM2.5 in 2015 (due to the availability of data from 2015).
Brain cortical thickness and WMHs
All survey centers obtained brain 3D-T1-magnetization-prepared rapid gradient-echo images as per a standardized MRI protocol. The FreeSurfer version 6.0 pipeline (http://surfer.nmr.mgh.harvard.edu/) was used to estimate cortical thicknesses (unit: mm) in the following predefined cortical areas: frontal, temporal, parietal, occipital, cingulate, and insular lobes. We calculated a global cortical thickness by averaging these six regional cortical thicknesses for each participant. Intracranial volume (unit: mm3) was measured using the same method. The survey centers in Incheon and Wonju additionally collected T2-weighted fluid-attenuated inversion recovery images, from which total, periventricular, and deep WMH volumes (unit: mm3) were calculated using an automated method as previously described.192021
High sensitivity CRP
The level of high sensitivity CRP (hs-CRP, unit: mg/L) was obtained by immunoturbidimetric assay. Individuals with a markedly high level of hs-CRP (> 10 mg/L) were excluded from the analysis (n=18 in men; n = 8 in women) in order to rule out the impact of possible acute infection at the time of blood sampling.22 Because there was no standard cutoff level of hs-CRP indicating a high risk of brain cortical atrophy, participants were categorized as those with higher and lower than median (0.69 mg/L in men and women combined; 0.69 mg/L in men; 0.68 mg/L in women) hs-CRP levels.
Statistical analysis
To investigate whether the associations between PM and brain imaging markers differs by the level of hs-CRP, we first created the higher (≥ median) and lower (< median) hs-CRP groups out of the entire study population. We then performed linear regression analyses to estimate the effects of PM10 (per 10 µg/m3 increment) and PM2.5 (per 1 µg/m3 increment) on a global cortical thickness in the entire study population as well as in each of the two hs-CRP groups. We also estimated the effects of PM10 (per 10 µg/m3 increment) and PM2.5 (per 1 µg/m3 increment) on total, periventricular, and deep WMH volumes. To account for highly skewed distribution of the WMH data, each of the three WMH volumes was dichotomized as higher (≥ median) and lower (< median) values. We performed logistic regression analyses in the entire study population, as well as in each of the two hs-CRP groups. Given that chronic systemic inflammation is strongly related to cardiometabolic health,2324 we a priori selected the following covariates: demographics (age, sex, years of education), history of cardiometabolic disease (hypertension, diabetes mellitus, and angina or myocardial infarction), cardiometabolic risk behaviors (smoking status [never, former, or current smoker], alcohol consumption [currently drinking or not], and engagement in vigorous exercise [yes or no]), and cardiometabolic risk biomarkers (systolic blood pressure, diastolic blood pressure, fasting blood glucose level, and total cholesterol level). Survey year and intracranial volume were also adjusted for in line with our previous study.8 Significance of the hs-CRP group difference was tested and expressed as p for interaction.25 A significant difference between the hs-CRP groups means that the level of hs-CRP is an effect modifier in the association between PM and a brain imaging marker. Taking possible sex differences in brain imaging markers into account,26 sex-stratified analyses were additionally conducted.
All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA). Two-sided P < 0.05 was set as statistical significance.
RESULTS
Gray matter cortical thickness
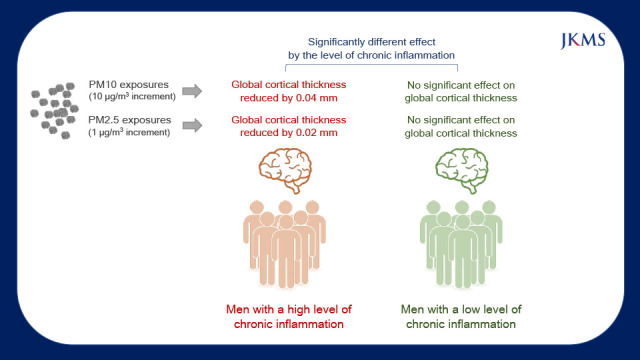
A total of 874 participants (392 men and 482 women) were included in the analyses of global cortical thickness (Table 1). Overall, the mean (standard deviation) value of age was 67.5 (6.4) years, and that of MMSE score was 27.3 (2.6). The mean (standard deviation) value of global cortical thickness was 2.45 (0.08) mm. Characteristics of the participants by the level of hs-CRP are shown in Supplementary Table 2. None of the associations of PM10 (β = −0.003; 95% confidence interval [CI], −0.014 to 0.008) and PM2.5 (β = 0.002; 95% CI, −0.005 to 0.009) with global cortical thickness was statistically significant in the entire study population, as well as both in the higher (≥ 0.69 mg/L) and lower (< 0.69 mg/L) hs-CRP groups (Table 2). Among men, the higher hs-CRP group had significantly reduced global cortical thicknesses associated with PM10 (β = −0.039; 95% CI, −0.063 to −0.016; P for interaction = 0.015) and PM2.5 (β = −0.023; 95% CI, −0.040 to −0.006; P for interaction = 0.006). Among women, none of the differences in the associations between the higher and lower hs-CRP groups was statistically significant.
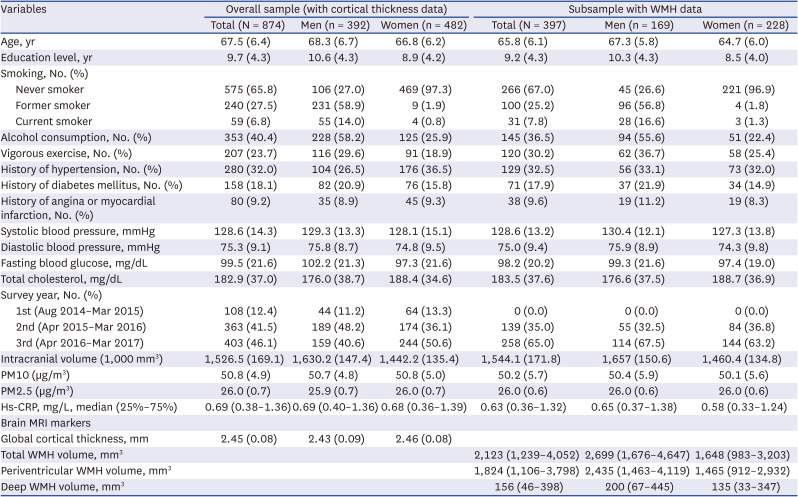
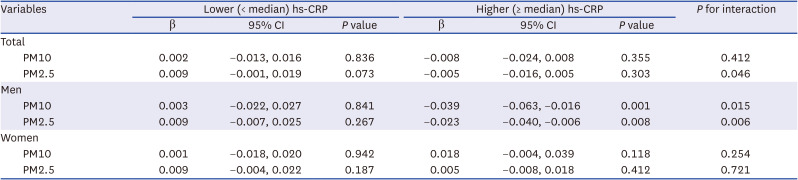
Table 1
Characteristics of study participants
Values are expressed as mean (standard deviation), unless otherwise is specified. Participants with cortical thickness data included those with WMH data.
WMH = white matter hyperintensity, PM10 = particulate matter 10 µm or less in diameter, PM2.5 = particulate matter 2.5 µm or less in diameter, hs-CRP = high sensitivity C-reactive protein.
![]()
Table 2
Associations between particulate matter exposures and global cortical thickness, stratified by the level of hs-CRP
Beta coefficients (per a 10 µg/m3 increment in PM10 or a 1 µg/m3 increment in PM2.5) were estimated from generalized linear models, adjusting for age, sex (in the total model only), years of education, smoking status, alcohol consumption, vigorous exercise, hypertension, diabetes mellitus, angina or myocardial infarction, systolic blood pressure, diastolic blood pressure, fasting blood glucose level, total cholesterol level, survey year, and intracranial volume.
hs-CRP = high-sensitivity c-reactive protein, CI = confidence interval, PM10 = particulate matter 10 µm or less in diameter, PM2.5 = particulate matter 2.5 µm or less in diameter.
![]()
WMHs
A total of 397 participants (169 men and 228 women) were included in the regression analyses of WMH (Table 1). Overall, the mean (standard deviation) value of age was 65.8 (6.1) years, and that of MMSE score was 28.0 (1.9). The median (25–75%) value of total WMH volume was 2,123 (1,239–4,052) mm3. Characteristics of the participants by the level of hs-CRP are shown in Supplementary Table 3. A 10 μg/m3 increase in PM10 was significantly associated with higher volumes of total WMH (odds ratio [OR], 1.78; 95% CI, 1.07–2.97) and periventricular WMH (2.00; 1.20–3.33) (Fig. 1). A 1 μg/m3 increase in PM2.5 was significantly associated with the higher (than median) volume of periventricular WMH (OR, 1.66; 95% CI, 1.08–2.56). These associations did not significantly differ between the lower and higher hs-CRP groups (Table 3). After stratification by sex, none of the associations of PM10 and PM2.5 with total, periventricular, and deep WMH volumes significantly differed between the lower and higher hs-CRP groups.
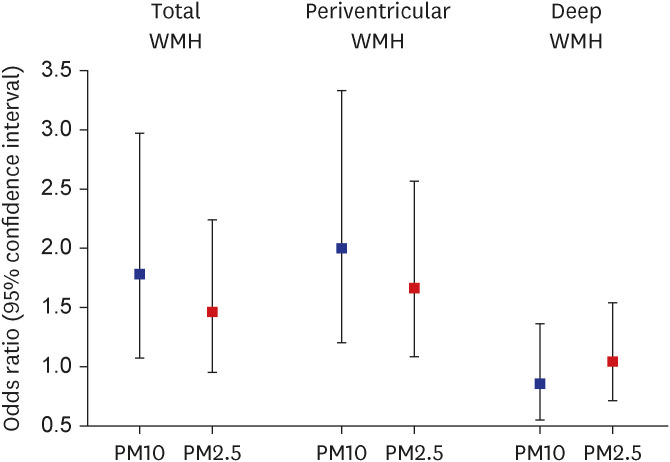
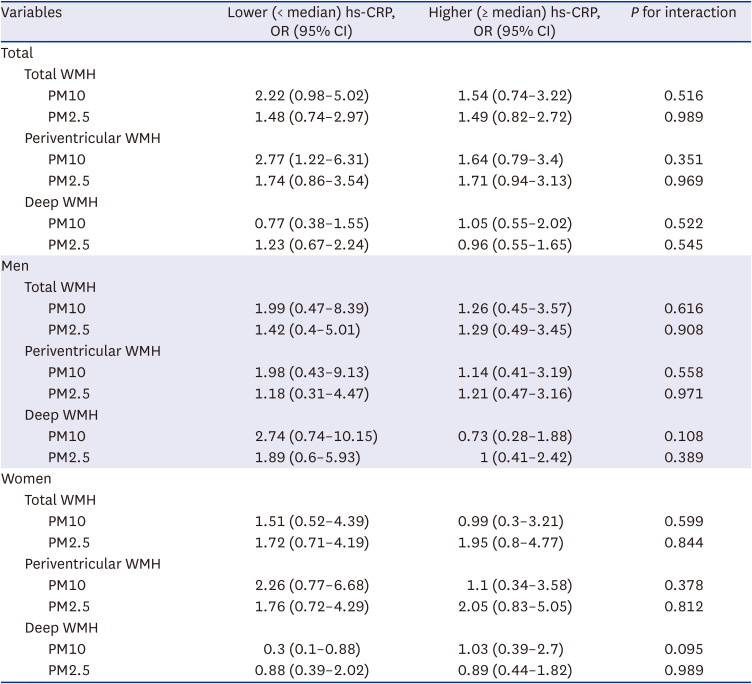
Fig. 1
Associations between particulate matter exposures and white matter hyperintensity volumes. Odds ratios of having the higher (≥ median) volume of WMH (per a 10 µg/m3 increment in PM10 or a 1 µg/m3 increment in PM2.5) were estimated from logistic regression models, adjusting for age, sex, years of education, smoking status, alcohol consumption, vigorous exercise, hypertension, diabetes mellitus, angina or myocardial infarction, systolic blood pressure, diastolic blood pressure, fasting blood glucose level, total cholesterol level, survey year, and intracranial volume.
WMH = white matter hyperintensities, PM10 = particulate matter 10 µm or less in diameter, PM2.5 = particulate matter 2.5 µm or less in diameter.
![]()
Table 3
Associations between particulate matter exposures and white matter hyperintensity volumes, stratified by the level of hs-CRP
ORs of having the higher (≥ median) volume of WMH (per a 10 µg/m3 increment in PM10 or a 1 µg/m3 increment in PM2.5) were estimated from logistic regression models, adjusting for age, sex, years of education, smoking status, alcohol consumption, vigorous exercise, hypertension, diabetes mellitus, angina or myocardial infarction, systolic blood pressure, diastolic blood pressure, fasting blood glucose level, total cholesterol level, survey year, and intracranial volume.
Hs-CRP = high-sensitivity c-reactive protein, OR = odds ratio, CI = confidence interval, WMH = white matter hyperintensity, PM10 = particulate matter 10 µm or less in diameter, PM2.5 = particulate matter 2.5 µm or less in diameter.
![]()
DISCUSSION
The present study is the first study to investigate whether the level of hs-CRP modifies the effects of particulate matter exposures on global cortical thickness and WMH volumes on brain MRI. One of the main findings was that PM10 and PM2.5 exposures were significantly associated with a reduced global cortical thickness in men with the higher level of hs-CRP, but not in men with the lower (than median) level of hs-CRP. The difference between these two hs-CRP groups was statistically significant. Another main finding was that particulate matter exposures were significantly associated with higher volumes of total and periventricular WMH, with no evidence of effect modification by the level of hs-CRP.
Evidence on the modifying role of chronic systemic inflammation in the neurotoxicity of particulate matter is scarce in human studies. A recent epidemiological study demonstrated that a high level of long-chain omega-3 polyunsaturated fatty acid (reducing oxidative stress and systemic inflammation) attenuated the adverse effect of PM2.5 on white matter volume.11 While this previous study only included women, our study involved both sexes and did not observe significant effect modification by hs-CRP among women. Although the previous study and ours cannot be directly compared because a high level of long-chain omega-3 polyunsaturated fatty acid does not necessarily mean a low level of systemic inflammation, the discrepancy is likely to be attributed to different characteristics of study populations (e.g., relatively low levels of hs-CRP in Asian populations).27 Regarding the sex difference in the effect modification by hs-CRP in our study, it can be argued that smoking status may have contributed to the significant effect modification by hs-CRP among men only (because 97% of women were never smokers). However, in our additional analyses constraint to never smokers, we found similar results to the overall analyses (Supplementary Table 4). Moreover, the sex difference we observed is supported by animal studies, suggesting that less expression of the enzyme paraoxonase 2 (which has anti-inflammatory properties) may lead to a greater level of lipid peroxidation and inflammation in response to air pollution exposures in the male (versus female) brain.2829 The possible susceptibility to the neurotoxicity of particulate matter in men warrants further studies in humans and animals.
This study demonstrated that particulate matter exposures were associated with gray matter atrophy in men with the higher level of hs-CRP (a marker of systemic inflammation), but not in those with the lower level. In vitro and in vivo studies have indicated that systemic inflammation can deteriorate blood-brain barrier integrity,3031 which can be damaged by particulate matter exposures as well.32 Given that blood-brain barrier disruption contributes to neurodegeneration,33 our findings indicate that particulate matter exposures may induce gray matter neurodegeneration under systemic inflammatory conditions. It is also reasonable to suggest that chronic systemic inflammation may increase susceptibility to gray matter atrophy attributable to particulate matter exposures, particularly in men.
The relationship between exposure to particulate matter and WMH has been investigated in only a few studies. A study including the elderly without dementia or stroke showed no significant association between PM2.5 and a WMH volume.3 A study of individuals with mild cognitive impairment or early dementia found that an increase in PM2.5 was associated with a lower WMH volume.4 A recent analysis of UK Biobank demonstrated that the association between PM2.5 and a WMH volume was statistically significant in individuals participating in vigorous physical activity, but not in the entire cohort.34 The present study adds more granular data to the existing evidence by distinguishing periventricular WMH and deep (subcortical) WMH, which may involve different cerebrovascular pathologies. Studies have shown that periventricular WMH are related to hemodynamic changes (e.g., reduced cerebral blood flow and cerebrovascular reactivity),3536 whereas deep WMH are indicative of long-term ischemic lesions.37 A study also exhibited divergent predictors for periventricular WMH (age and arterial pressure) and deep WMH (body mass index).38 In the present study, particulate matter exposures were positively associated with WMH in the periventricular area, but not in the deep area. This regional difference may be the clue to the absence of effect modification by chronic systemic inflammation in the association between particulate matter and WMH. Small-vessel disease is categorized as cerebral amyloid angiopathy and hypertensive arteriopathy. Evidence suggests that cerebral amyloid angiopathy (in the cortical region) is related to systemic inflammation, whereas hypertensive arteriopathy (frequently in the periventricular area) is more strongly associated with vascular inflammation than systemic inflammation.39 Although we did not address cerebral amyloid angiopathy and vascular inflammation, our findings at least imply that particulate matter exposures, regardless of the status of systemic inflammation, might accelerate vascular aging and induce hemodynamic changes or hypertensive arteriopathy in the brain vasculature. Further, considering that clinical studies have shown that periventricular WMH (but not deep WMH) is associated with reduced executive function and speed processing,404142 periventricular WMH might partly explain cognitive impairment associated with particulate matter exposures.
There are several limitations to be acknowledged. First, because hs-CRP is a non-specific marker of inflammation, the level of hs-CRP might not necessarily reflect the chronic status of systemic inflammation. To address this issue, individuals with hs-CRP > 10 mg/L (indicating acute infection or inflammation) were excluded. Second, the prediction data of PM2.5 concentrations used in the present study was one-year average concentrations of PM2.5 in 2015, due to the unavailability of nationwide air quality monitoring data before 2015. This means that we considered variation in PM2.5 concentrations only by geographical location for one year while disregarding temporal variations in PM2.5 concentrations. Third, the sex-stratified analyses for WMH yielded null findings possibly due to insufficient statistical power. Thus, it may be premature to conclude that chronic inflammation does not modify the association between particulate matter exposures and WMH among men and women, respectively. Future studies with larger sample size are required. Last, there could be unmeasured confounders. For example, this study did not consider apolipoprotein ε genotype, which is closely linked to the risk of the development and progression of Alzheimer’s disease.43 In healthy individuals, the apolipoprotein ε4 allele has been reported to affect brain morphology, but some studies did not observe this linkage.44
In summary, the present study showed that men with a high level of chronic inflammation exhibited brain cortical thinning associated with particulate matter exposures. This suggests that men with a high level of chronic inflammation may be susceptible to brain structural changes attributable to particulate matter exposures. Particulate matter exposures were also associated with a greater volume of WMH, but we found no evidence of effect modification by the level of chronic inflammation.
 XML Download
XML Download