

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus is a common human opportunistic commensal capable of causing a wide spectrum of conditions that range from asymptomatic colonization to life-threatening systemic infections, including bacteremia and sepsis.12 Despite the development of novel antibiotics, the overall mortality rates from S. aureus bacteremia (SAB) remain between 20% and 30%,345 owing to increasing antimicrobial resistance and the emergence of more virulent strains.67
S. aureus alpha-toxin (AT) or alpha-hemolysin, a highly potent exotoxin encoded by hla, has been recognized as an important virulence factor for more than a century.89 Upon binding to its receptor ADAM10 (a disintegrin and metalloprotease domain-containing protein 10) on the surface of various target cells (such as red blood cells, platelets, immune cells, pneumocytes, keratinocytes, and vascular endothelial cells), AT heptamerizes and inserts into the cell membrane to form pores, which results in cell lysis, inflammation, immune modulation and tissue damage.781011 Hyperexpression of AT has been associated with the enhanced virulence of strains such as USA300 and ST93,1213 and inhibition of AT by active or passive immunization has demonstrated protective effects in various animal models of infection.1415161718 Moreover, previous serological studies with S. aureus-infected patients reported that high anti-AT antibody (Ab) titers were suggestive of a lower risk of sepsis, and patients with low anti-AT Ab titers tended to have a higher rate of endovascular infection.31920 Although much of the current evidence suggests that anti-AT Abs play a protective role against invasive S. aureus infection, only a limited number of studies have focused on anti-AT Abs in SAB.
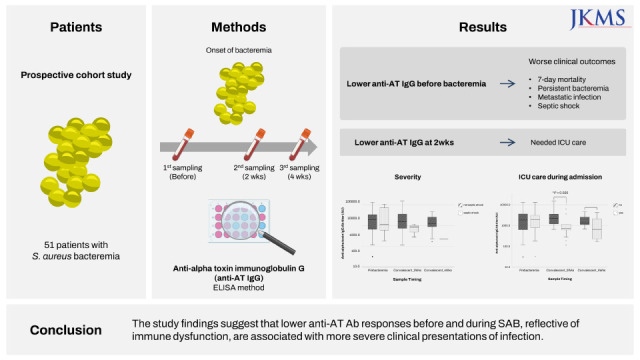
Therefore, in this study, we aimed to determine whether serum anti-AT immunoglobin G (IgG) levels during SAB are associated with clinical outcomes and infection severity. The findings of this study will provide insight to help improve the treatment of patients with SAB.
METHODS
Study subjects and samples
A total of 51 patients with SAB (age > 18 years) from a prospective SAB cohort at a tertiary-care hospital in South Korea (Seoul National University Bundang Hospital, Seongnam) were enrolled in the study from July 2016 to January 2019. Residual peripheral blood samples were collected to measure anti-AT IgG levels at different time points during SAB: pre-bacteremia (D-5 to D-1), 2 weeks (D14), and 4 weeks (D28) after bacteremia. The day on which the first S. aureus-growing blood culture was performed was defined as Day 0.21 Potential study subjects were identified prospectively by screening blood culture results for the growth of S. aureus, and clinical blood samples (which are routinely banked at 4°C for 5–7 days before disposal) at the study institution were identified and collected for further analysis.
We excluded the patients with suspected contamination and polymicrobial infection, those with a white blood cell count of less than 4,000/μL, and patients who received immunosuppressive treatment within the preceding 3 months. Additionally, patients for whom no residual blood samples were available and those who declined participation in the cohort or study were excluded.
The following clinical data were collected: demographic characteristics, primary site of infection, intensive care unit (ICU) admission during the current hospitalization episode, Charlson’s comorbidity-weighted index scores,22 Pitt bacteremia scores,23 sequential organ failure assessment scores,24 place of SAB acquisition (community-acquired [CA] or community-onset [CO] or hospital-onset [HO] bacteremia), health care contact history,25 SAB-related mortality, antimicrobial therapy, and methicillin resistance of isolated S. aureus. SAB-related mortality was defined as death within 30 days of SAB onset in the absence of other evident causes of death.26 Patients who grew S. aureus in blood cultures for more than 4 consecutive days despite appropriate treatment were defined to have persistent bacteremia.2728 SAB patients who did not meet criteria for uncomplicated bacteremia according to practice guidelines were defined to have complicated bacteremia.29
One hundred patients without symptoms or signs of infection, admitted for other clinical reasons (ex. cardiovascular procedure) during the study period at the study institution, were enrolled as non-SAB controls, matched for age group and sex, and their residual blood samples were collected.
Measurement of anti-AT IgG using semi-quantitative enzyme-linked immunosorbent assay (ELISA)
Serum was frozen at −70°C until use. Anti-AT IgG concentrations in serum were measured using an ELISA. Briefly, 96-well plates (Nunc MaxiSorp; Thermo Fisher Scientific, Waltham, MA, USA) were coated with 1 μg/mL recombinant S. aureus AT (Cat#RPC20267; Biomatik, Ontario, Canada), diluted in phosphate-buffered saline (PBS), and incubated overnight at 4°C. The plates were washed three times in PBS with 0.05% Tween-20 and then blocked with 0.05% skim milk in PBS for 2 hours at 26°C. The blocked plates were washed again, and 100 μL aliquots of sera from patients with SAB (1:100 dilution in PBS with 0.05% Tween-20) was added to each well, followed by incubation at 26°C for 2 hours. After further washing, alkaline phosphatase-conjugated recombinant protein A/G (Cat#32391; Thermo Fisher Scientific) was diluted in dilution buffer, added to the wells, and the plates were incubated at 26°C for 2 hours. The plates were washed again, and 100 μL p-nitrophenyl phosphate (Cat#N9389; Sigma-Aldrich, St. Louis, MO, USA) was added to each well, followed by incubation for 30 minutes at 26°C in the dark. The reaction was stopped by adding 25 μL 3M sodium hydroxide to each well. The optical density at 405 nm (OD405) was measured using a BioTek EPOCH2 microplate reader (Agilent, Santa Clara, CA, USA). Mouse monoclonal anti-staphylococcal AT Ab (Cat#0210-001; IBT Bioservices, Rockville, MD, USA) diluted in PBS was used as reference: 100 μL of a 1:100 dilution was assigned the value of 1,000 AU, and anti-AT IgG levels for samples were calculated based on comparative OD measurements.30 Data were analyzed using GraphPad Prism v. 8 software (GraphPad Software, San Diego, CA, USA) using a 4-parameter logistic curve fit model without weighting. All assays were performed in duplicate, and data are presented as the mean of two independent measurements for each sample.
S. aureus isolates and hla gene by polymerase chain reaction (PCR)
S. aureus isolates from the first positive blood culture were collected for all participants and stored at −70°C until further use. All isolates were tested for the presence of hla by PCR amplification as previously described,31 using the following forward and reverse primers: Hla-PCR-F1, 5’-TGTCTCAACTGCATTAT TCTAAATTG-3’ and Hla-PCR-R1, 5’-CATCATTTCTGATGTTATCG GCTA-3’.
Statistical analysis
Statistical analysis was primarily performed using IBM SPSS Statistics v. 22.0 software (IBM Corp., Armonk, NY, USA) and plotted using IBM SPSS Statistics or GraphPad Prism v. 6.01 software. Linear mixed modeling (LMM) was performed using R v. 2.10 (R Foundation, Vienna, Austria). Depending on the type of distribution, data are presented as the mean ± standard deviation (SD), median ± interquartile range (IQR) or range, and proportions, as appropriate. Categorical variables were compared using χ2 and Fisher’s exact tests, while continuous variables were compared using independent t-tests and Mann-Whitney U tests.
Longitudinal analyses of anti-AT IgG levels were performed using LMM adjusted for sex, age range, and severity of infection (by means of septic shock development). A two-tailed P value of < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board at Seoul National University Bundang Hospital (B-1507-308-302). Informed consent was waived for patients with SAB who were discharged or died within 2-weeks of SAB onset, but all other participants, including healthy volunteers, provided written informed consent, as appropriate.
RESULTS
Clinical and microbiological characteristics
During the study period, 378 patients with SAB were identified. After excluding 107 patients following the exclusion criteria, 271 were considered eligible. Subsequently, 157 patients for whom no blood samples were available and 63 who declined to participate in the study were excluded. Finally, 51 patients consented to participate in the study (Fig. 1). The age of the participants ranged from 24 to 90 years (mean ± SD, 68.8 ± 16.2 years), and 58.8% (30/51) of the study population was male. Methicillin-resistant S. aureus was isolated from the blood cultures of 52.9% (27/51) of patients, and SAB-related mortality was 25.5% (13/51). HO SAB accounted for 78.4% (40/51) of cases, and 25.5% (13/51) were from a central venous catheter (Table 1). All S. aureus isolates were confirmed to harbor hla. A comparison of the clinical characteristics of the enrolled and excluded patients is summarized in Supplementary Table 1.
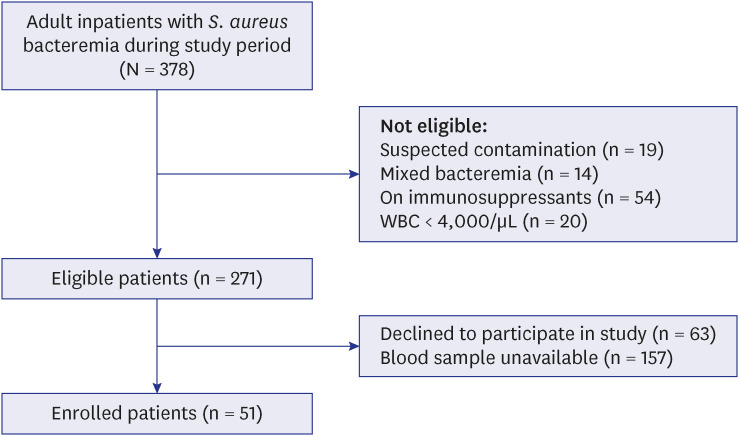
Table 1
Clinical characteristics of the patients with SAB (n = 51)
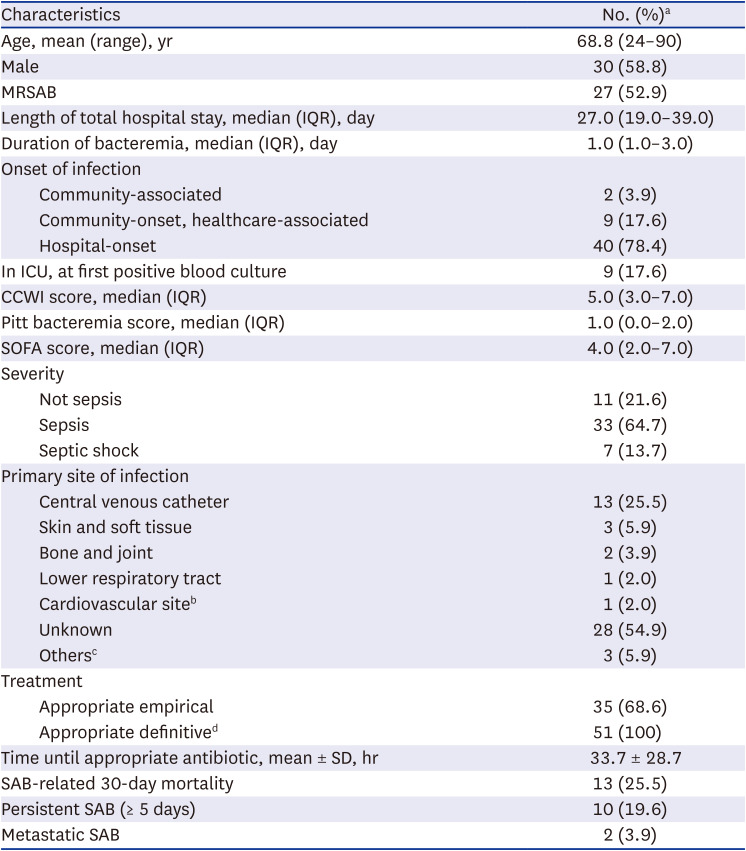
SD = standard deviation, MRSAB = methicillin-resistant Staphylococcus aureus bacteremia, IQR = interquartile range, ICU = intensive care unit, CCWI = Charlson’s comorbidity-weighted index, SOFA = sequential organ failure assessment, SAB = Staphylococcus aureus bacteremia.
aUnless otherwise specified; bVascular graft infection; cIntraabdominal (2), and urinary tract infection (1); dTreatment with susceptible antibiotics.
Pre-bacteremia anti-AT IgG levels in patients with SAB and non-infectious controls
Sera from patients with SAB were analyzed pre-bacteremia (range D-5 to D-1, median D-3) and on D14 and D28 post-bacteremia. Anti-AT IgG levels measured by ELISA varied widely among participants and were not significantly different between pre-bacteremic patients with SAB and non-infectious controls (Supplementary Fig. 1, Supplementary Table 2).
Anti-AT IgG levels associated with SAB severity and clinical outcomes
Pre-bacteremic anti-AT IgG levels tended to be lower in patients with worse clinical outcomes, although the association was not statistically significant. Patients who died within 7 days of developing SAB had lower anti-AT IgG levels than those who survived beyond 7 days (median [IQR], 623.5 [459.1–623.5] vs. 1,939.3 [653.5–3,622.6] AU, P = 0.225). Patients with persistent SAB had lower anti-AT IgG levels than those with transient SAB (1,355.9 [695.5–2,338.3] vs. 2,012.0 [608.9–4,205.5] AU, P = 0.393). Similarly, patients with metastatic infections had lower anti-AT IgG levels than patients without metastatic infections (865.4 [625.5–865.4] vs. 1,939.2 [652.7–3,622.6] AU, P = 0.357). Furthermore, patients who progressed to septic shock had lower anti-AT IgG levels than those who did not suffer septic shock (1,105.3 [459.1–9,547.1] vs. 1,885.6 [639.5–3,459.4] AU, P = 0.883) (Table 2).
Table 2
Anti-AT Ab levels in SAB patients at different time points during bacteremia according to clinical outcomes
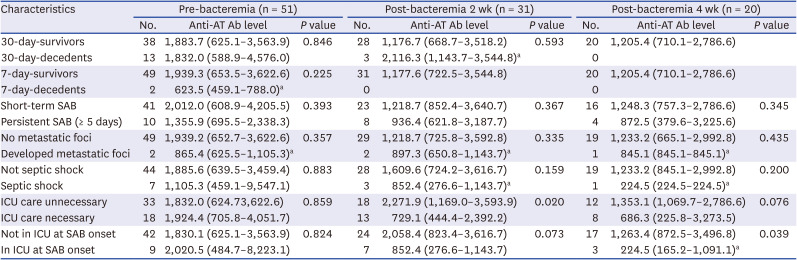
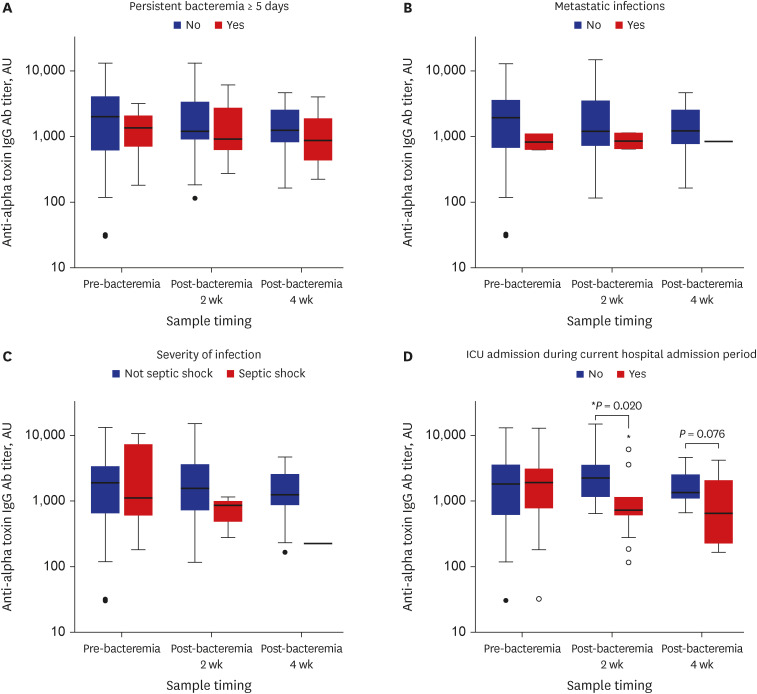
Levels of anti-AT IgG in patients with SAB during the bacteremia duration (pre-bacteremia [D-5 to D-1], n = 51; post-bacteremia [D14, n = 31; D28, n = 20]) analyzed by LMM showed no significant association with clinical outcome nor SAB severity. However, anti-AT IgG levels in patients with SAB who required ICU admission were significantly lower on D14 (P = 0.020) and tended to be lower on D28 (P = 0.076) post-bacteremia than in patients who did not require ICU care (Table 2). Similarly, anti-AT IgG levels in patients who were admitted to the ICU at SAB onset tended to be lower on D14 and D28 post-bacteremia (P = 0.073 and P = 0.039, respectively) than in patients admitted to general care (Table 2, Fig. 2). For comparison, anti-AT IgG levels among different clinical outcome groups in patients with HO SAB are summarized in Supplementary Table 3.
Fig. 2
Anti-AT IgG Ab levels in patients with Staphylococcus aureus bacteremia at different time points during bacteremia duration (pre-bacteremia and 2- and 4-weeks post-bacteremia) according to clinical outcomes: (A) persistent bacteremia ≥ 5 days (n = 10), (B) development of metastatic foci (n = 2), (C) progression to septic shock (n = 7), (D) requiring intensive care unit care (n = 18). Lower and upper box boundaries represent 25th and 75th percentiles, respectively; lines inside the box represent median; lower and upper error lines are 10th and 90th percentiles, respectively; filled circles show data falling outside 10th and 90th percentiles.
AT = alpha-toxin, Ab = antibody, IgG = immunoglobin G, ICU = intensive care unit.
*P < 0.05.
DISCUSSION
AT has been recognized as a major virulence factor in numerous animal models of invasive S. aureus infection,14161832 and the protective role of anti-AT Abs has been suggested by prior observational studies.31920 However, evidence of anti-AT Abs in patients with SAB remains limited.31 Therefore, in this study, we assessed anti-AT IgG levels in serum before and after SAB onset to examine the association between anti-AT Ab responses with severity and clinical outcomes of SAB. The results demonstrated that SAB patients with complicated bacteremia tended to have lower anti-AT IgG levels, and patients with severe infection who required ICU care had significantly lower anti-AT IgG levels on D14 and D28 post-bacteremia than patients for whom general care was sufficient.
Previous studies exploring Ab responses against S. aureus have shown that healthy individuals exhibit highly variable anti-staphylococcal Ab levels (including anti-AT IgG)30333435 and that Ab responses upon S. aureus infection differ considerably among individuals.1920333435 Dryla et al.33 suggested that the heterogeneity of Ab levels in healthy adults may be influenced by early childhood exposure to S. aureus, based on variable Ab levels reported among children. Moreover, a previous study reported the transient nature of serum Ab levels during S. aureus septicemia.19 Similarly, a recent study by Meyer et al.35 proposed that highly variable Ab responses within the general population reflect individual histories of encounters with S. aureus and are likely to be affected by colonization with S. aureus. In addition, Meyer et al.35 reported that factors such as age, sex, body mass index, elevated serum glucose levels, and smoking status, which are likely to affect adaptive immunity, were correlated with anti-staphylococcal Ab responses. Likewise, patients with SAB in the current study displayed a wide range of pre-bacteremic anti-AT IgG levels (Supplementary Fig. 1) and exhibited heterogenous anti-AT IgG responses during bacteremia (Supplementary Fig. 2), which likely reflects the complexity of the systemic immune response to S. aureus.
Most evidence suggesting that anti-AT Abs play a protective role against SAB is derived from observational studies assessing acute and convalescent sera during S. aureus infection.319203136 Colque-Navarro et al.19 reported that septic patients with initially low anti-AT IgG titers tended to have lower Ab responses during bacteremia than those with higher initial Ab levels, and also showed that patients with rising anti-AT IgG titers were less likely to develop complicated sepsis. In a prospective study involving 96 patients with invasive S. aureus infections, Jacobsson et al.20 reported that patients with fatal outcomes presented lower initial Ab levels. Similarly, a study exploring pre-existing anti-AT Abs in 100 patients with SAB reported that patients who developed sepsis had significantly lower IgG levels against S. aureus exotoxins, including AT than those who did not develop sepsis.3 Consistent with these findings, the results of the current study also demonstrated that patients with SAB with lower pre-bacteremic anti-AT IgG levels tended to have poor prognoses (7-day mortality) or developed complications such as persistent bacteremia, metastatic infection, or septic shock. The lack of statistical significance in these results may be explained by the wide range of anti-AT IgG levels displayed by participants, small study population size, and even smaller number of patients who developed complications during SAB. In addition, although all S. aureus isolates harbored hla, bacterial strain-specific factors such as AT production might also have played a role. Indeed, an association between bacterial typing groups (agr and pulsed-field gel electrophoresis groups) and Ab responses has been reported,20 and patients infected with AT-expressing strains tended to have higher Ab levels during SAB,31 despite the highly conserved nature of AT among diverse S. aureus isolates.3738
Regarding Ab responses during SAB, Meyer et al.35 estimated that 6% of the general population had low anti-AT Ab responses and anticipated that these individuals would have a tendency to develop more severe manifestations during S. aureus infection. Concurring with this hypothesis, patients with SAB in the current study who tended to have poor prognoses or develop complications displayed lower anti-AT IgG levels during convalescence than those with better prognoses. In particular, patients with SAB who clinically deteriorated to medical conditions requiring ICU care had significantly lower anti-AT IgG levels during the convalescent phase than patients with SAB who remained in general care, which likely reflects a dysregulated humoral immunity in these patients.20
AT is a highly conserved major virulence factor of S. aureus, which can elicit a neutralizing humoral response in the host upon exposure.7 As previously mentioned, patients with higher anti-AT Ab levels were more likely to present with less severe disease than patients with lower anti-AT Ab levels in several studies, and active or passive vaccination against AT has been successful in many animal models of S. aureus infections, which all support the importance of AT as a target for immunoprophylaxis.8 However, recent studies exploring anti-AT Abs in human cases of S. aureus infection have reported conflicting results. For example, Sharma-Kuinkel et al.31 did not find a correlation between anti-AT Ab levels and patient outcomes in a study of 200 high-risk patients with SAB. Furthermore, a recent phase II clinical trial assessing the efficacy of suvratoxumab (a monoclonal anti-AT Ab) against ventilator-associated pneumonia caused by S. aureus failed to show statistically significant results.39 This lack of statistical significance may be due to highly variable individual immune responses to AT in different clinical conditions, supported by the fact that AT can target a wide range of host immune cells, resulting in complex pathogenesis.8
Our study has several limitations. First, the study was planned as a prospective cohort study rather than an interventional study, resulting in a lack of control over all study procedures. Only patients for whom pre-bacteremia blood samples were available and who consented to participate were included in the study; thus, the population size was small. Furthermore, patients with SAB in critically ill conditions were less likely to be enrolled, leading to relatively small numbers of patients with unfavorable clinical results compared to that in previous studies.2140 However, the clinical characteristics of the enrolled patients did not differ significantly from the excluded ones. For SAB patients who were diagnosed immediately after admission (CO or CA SAB patients), the exact onset time of SAB could only be assumed on clinical grounds only (Supplementary Table 4). Therefore, it is possible that the pre-bacteremia samples were taken after bacteremia onset, which might have led to bias. However, anti-AT IgG levels in HO SAB patients among different clinical outcome groups showed similar trends as in all enrolled patients. In addition, clinical blood samples in the convalescent phase were unavailable for all participants, and a limited number of participants had measured anti-AT IgG levels on D14 and D28 post-bacteremia. Thus, the number of enrolled patients with SAB and obtained blood samples may have been insufficient to show the effects of anti-AT Abs on SAB outcomes. However, as anti-staphylococcal Ab responses are known to be influenced by various factors and are highly heterogeneous, we believe our study findings are largely comparable to those reported in previous studies. Finally, the current study did not analyze bacterial factors, including AT toxigenicity, agr type, and inoculum dose, which could have affected immune responses and clinical outcomes of SAB.
In conclusion, lower anti-AT IgG levels before and during SAB may be associated with more severe clinical presentations, suggesting that passive immunization might be beneficial for these patients. The study findings may help improve treatment outcomes of SAB by providing insight into the function of protective anti-AT Abs during infection with S. aureus.
 XML Download
XML Download