

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to population-based studies, the prevalence of irritable bowel syndrome (IBS) is > 10% and on the rise, particularly in Asian countries.1234 Based on studies conducted on residents in South Korea, the prevalence of IBS is similar to that in other countries, (at 8-9.6%).15 The health-related quality of life in patients with IBS is low.6 Patients with IBS report more psychiatric symptoms including anxiety and depression, compared to healthy individuals.7 They also cause a large economic burden due to the excessive consumption of medical resources caused by inadequate measures to control the symptoms.8
According to the Rome IV definition revised in 2016, IBS is defined by abdominal pain recurrent at least once per week for three consecutive months, and is associated with at least two of the following symptoms: abdominal pain associated with defecation, changes in the frequency of defecation, and changes in the defecation pattern.4 IBS has recently been defined as a chronic gastrointestinal functional disease characterized by recurrent abdominal pain, abdominal distension, loose stools, and diarrhea or constipation without structural abnormalities, biochemical abnormalities, or excessive inflammation.9 Nevertheless, while the Rome criteria have been used for diagnosis, each country or continent has formulated individual guidelines for treatment, since the Rome criteria are based on Western patients in English-speaking countries.101112131415 For the rational diagnosis and treatment of IBS, the opinions of domestic experts were collected, and the article “Guidelines for the Treatment of Irritable Bowel Syndrome,” suitable for the medical situation in Korea was published in 2011.16 The clinical treatment guidelines were revised mainly for primary care doctors in 2018.17
Accordingly, the IBS and Intestinal Function Research Study Group of the Korean Society of Neurogastroenterology and Motility (KSNM) conducted a survey to analyze and examine the current status of clinical treatment for IBS, based on the expected differences in doctors' perceptions of IBS and clinical treatment patterns. Considering the revised Rome IV criteria and improved clinical guidelines in South Korea, this study aimed to investigate the understanding of doctors, and their therapeutic practices.
METHODS
Target population and methods
From October 2019 to February 2020, a survey was conducted among doctors working in primary, secondary, and tertiary healthcare institutions. The physicians surveyed were randomly selected by members of the KSNM and the Korean Society of Gastroenterology (KSG). We randomly sent e-mails or messages with a guidance note about this study and the link to the NAVER questionnaire platform. In medicine, levels of care refer to the complexity of the medical cases doctors treat and the providers’ skills and specialties. Levels are divided into the following categories: primary, secondary, and tertiary care. Primary care means day-to-day health-care given by a health care provider; its provider acts as the first contact and principal point of continuing care for patients within a healthcare system. Secondary care refers to care provided at a general hospital, and tertiary care refers to care provided at a university teaching hospital. Considering the Korean healthcare system, the difference was analyzed by dividing care into tertiary healthcare institutions and primary and secondary healthcare institutions.
The questionnaire comprised items on general characteristics, diagnosis, colonoscopy, and treatment, a total of 37 items. (Supplementary Data 1) General characteristics comprised 7 items including the type of institution, location, specialty and experience; diagnosis characteristics comprised 3 items; colonoscopy comprised 4 items; and treatment comprised 23 items.
Data analysis
Data were analyzed using IBM Statistics SPSS 25.0 (IBM Corp., Armonk, NY, USA). The general characteristics of the survey participants were analyzed in terms of frequency and percentage (%). To examine the difference according to the size (type of practice), the frequency and percentage (%) were presented, a χ2 test was performed, and the statistical significance was reviewed with P less than 0.05.
RESULTS
Characteristics of respondents
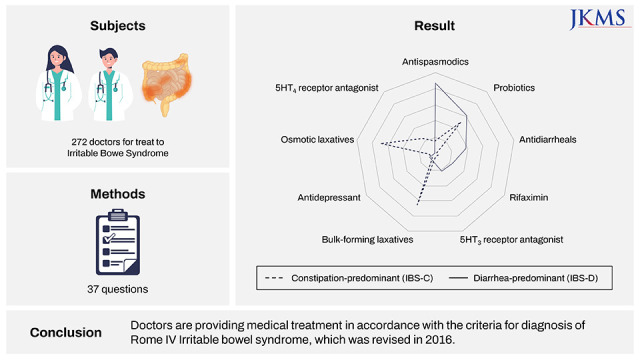
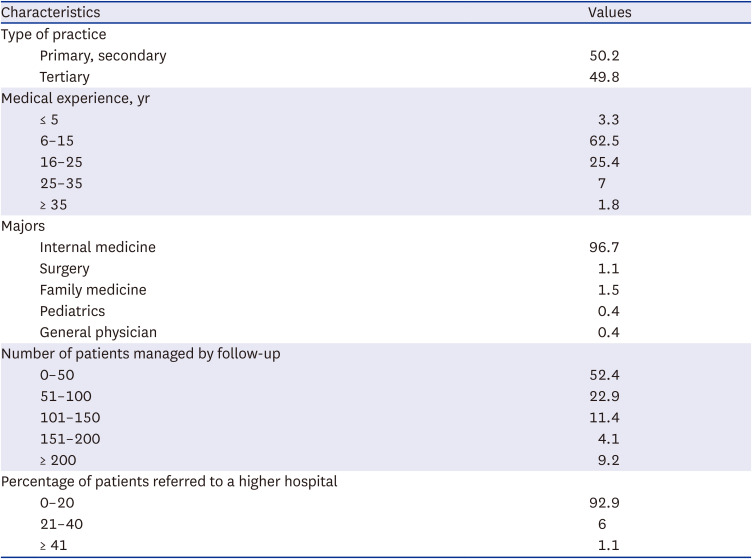
Two hundred and seventy-two doctors completed the questionnaire. The baseline characteristics are presented in Table 1. Regarding the type of practice, 50.2% of the respondents worked at primary and secondary healthcare institutions, and 49.8% worked at tertiary healthcare institutions. All respondents were gastroenterologists or specialists of functional gastroenterology affiliated with the KSNM or KSG. Regarding medical experience, 62.5% had 6–15 years of experience, and most participants (96.7%) specialized in internal medicine. Most respondents (52.4%) had managed 0–50 patients with IBS by follow-up at the time of response; physicians in internal medicine managed 51–100 patients on average. In 91.9% of the cases, 0–20% of patients with IBS who visited the clinic were referred to a tertiary medical institution.
Table 1
Characteristics of the doctors who responded to a questionnaire-based survey on the diagnosis and treatment of irritable bowel syndrome (N = 272)
Diagnosis of IBS
Seven questions were related to the diagnosis of IBS (Table 2). Regarding the diagnostic criteria, 51% (n = 136) of the respondents defined IBS as a chronic digestive functional disease characterized by repetitive abdominal pain and swelling, soft stools, and diarrhea or constipation without structural and biochemical abnormalities, and excessive inflammation; 30% (n = 80) of the respondents defined IBS as a chronic and complex disease with complex symptoms such as abdominal pain, discomfort, and bloating, with changes in bowel habits for at least six months; 19% (n = 51) of the respondents defined IBS as a functional bowel disease with abdominal pain and changes in bowel movements without organic abnormalities. Accordingly, 82% (n = 221) of the respondents recognized IBS according to the new diagnostic criteria for IBS revised in 2016. There were no statistically significant differences in the groups regarding the type of practice (P = 0.199).
Table 2
Diagnosis of irritable bowel syndrome by type of practice, as per the results of a questionnaire-based survey of physicians working at primary, secondary, and tertiary healthcare institutions
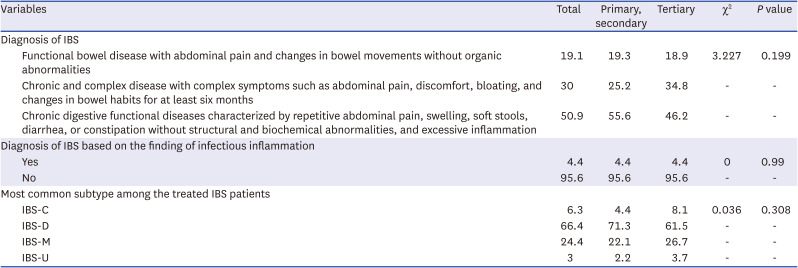
Regarding the most common subtype among patients with IBS, the following responses were obtained: diarrhea-predominant subtype (IBS-D), 66% (n = 180) respondents; mixed subtype (IBS-M), 24% (n = 66) respondents; constipation-predominant subtype (IBC-C), 6% (n = 17) respondents; and unsubtyped IBS (IBS-U), 3% (n = 8) respondents.
Table 3 shows the results of colonoscopy-related analysis of patients with IBS. Twenty-eight percent (n = 75) of respondents answered that colonoscopy was performed in 41–60% of patients with IBS; the other responses were as follows: 21% (n = 57) of the respondents, 61–80% of IBS patients, and 21% (n = 56) of the respondents, ≥ 81% of patients with IBS. There was a statistically significant difference according to the level of healthcare institutions (P < 0.001), and the rate of colonoscopy was high in tertiary healthcare institutions. The reasons for performing colonoscopy for IBS included the following: 38% (n = 102) of respondents selected, ‘ineffective treatment with medication’; 32% (n = 85) of respondents selected, ‘changes in bowel habits in patients aged 50 or older’; and 31% (n = 82) of respondents selected, ‘others’. There was a statistically significant difference according to the level of healthcare institutions (P = 0.005). In primary and secondary healthcare institutions, most participants (45%, n = 60) answered ‘ineffective treatment with medication.’ The response ‘changes in bowel habits in patients aged 50 years or older’ was more commonly obtained from respondents working at tertiary healthcare institutions (40%, n = 54).
Table 3
Percentage of patients with irritable bowel syndrome who underwent colonoscopy and the main reason for conducting the colonoscopy by type of practice, as per the results of a questionnaire-based survey of doctors from primary, secondary, and tertiary healthcare institutions
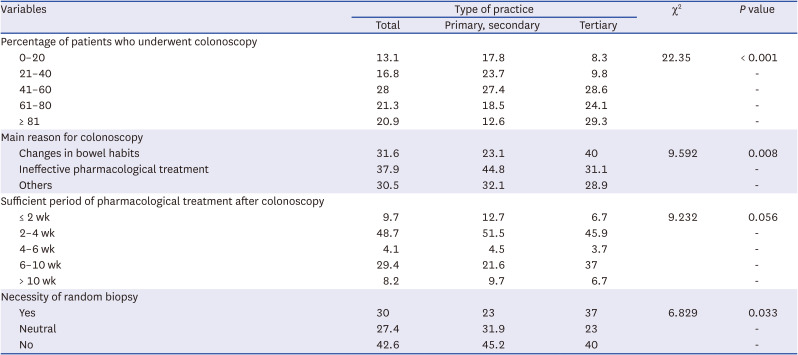
Regarding the period of sufficient pharmacological treatment after colonoscopy, 49% (n = 131) of respondents reported a treatment period of 2–4 weeks or longer. Depending on the type of practice, the rate of answering ‘within 4 weeks’ was higher at primary and secondary healthcare institutions compared to tertiary healthcare institutions by approximately 11.6%, and that of answering ‘6 weeks or longer’ was lower by approximately 12.4%, though no statistically significant difference was identified (P = 0.056).
Regarding the necessity of random biopsy, the most frequently provided answer was ‘no’ (45.6% of the respondents). There was a statistically significant difference in the number of respondents who reported the necessity of random biopsy according to the type of practice (P = 0.033); this number was higher among respondents who worked at tertiary healthcare institutions than among those who worked at primary and secondary healthcare institutions.
Non-pharmacological treatment of IBS
Low FODMAP (fermentable oligo-, di-, and mono-saccharides, and polyols) diet
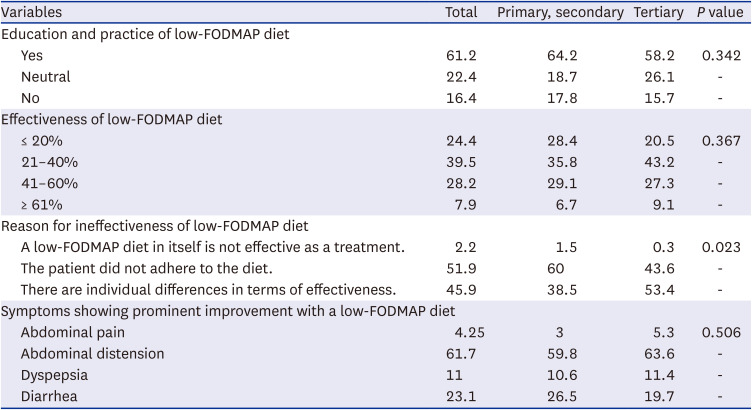
Table 4 presents data on the items on a low-FODMAP diet. When queried on whether they educated and recommended patients with IBS to adhere to a low-FODMAP diet, 61% (n = 164) respondents gave a positive answer. The rate of effectiveness of a low-FODMAP diet was reported as mostly 21–40%, (with an average of 35). Respondents reported the following as the symptoms that showed prominent improvement with a low-FODMAP diet: abdominal distension (62%) and diarrhea (23%). Insufficient adherence to the diet was cited as the reason for the ineffectiveness of a low-FODMAP diet by 52% (n = 139) of respondents, whereas ‘individual differences’ was cited as the reason by 46% (n = 123) of respondents. The rate of citing ‘insufficient adherence to the diet’ as a reason was 16.4% higher at primary and secondary healthcare institutions compared to tertiary healthcare institutions; the rate of citing ‘individual differences’ as the reason was 14.9% lower in primary and secondary healthcare institutions.
Table 4
Responses pertaining to questions on a low-FODMAP diet, by type of practice
Physical activity
As Table 5 shows, there was no statistically significant difference between the groups (P = 0.197), regarding whether the doctors recommended patients with IBS to increase their level of physical activity; 66% (n = 170) of respondents answered ‘Yes’ to this question.
Table 5
Responses to a query on the recommendation to increase physical activity in patients with irritable bowel syndrome, by type of practice

| Variables | Total | Primary, secondary | Tertiary | χ2 | P value | |
|---|---|---|---|---|---|---|
| Increase in physical activity is recommended | ||||||
| Yes | 64.9 | 62.5 | 67.4 | 3.245 | 0.197 | |
| Neutral | 24.4 | 28.7 | 20 | - | - | |
| No | 10.7 | 8.8 | 12.6 | - | - | |
Pharmacological treatment of IBS
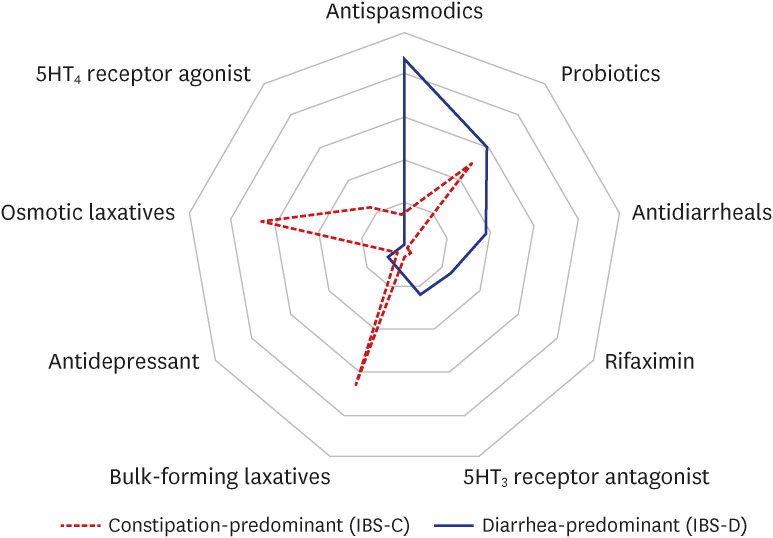
Regarding the number of drug types used in combination as the first-line pharmacological treatment, the responses were as follows: one type, 4% (n = 11) of respondents; two types, 42% (n = 114) respondents; three types, 45% (n = 123) of respondents; and four types, 9% (n = 24) of respondents. IBS is often treated using a combination of two or three types of drugs to improve abdominal pain and regularize bowel habits. Therefore, the choice and combination of drugs are likely to vary according to the IBS subtype and symptom severity. The first-line choice of IBS treatment illustrated in Fig. 1. In each IBS pattern, the farther the line from the center, the more its treatment is used.
Treatment for patients with IBS-C
Table 6 shows the item allowing multiple answers regarding the drugs used as the first-line treatment. Depending on the type of practice, the use of the serotonin type 4 receptor agonist was statistically and significantly higher in tertiary healthcare institutions (P = 0.001), whereas the use of serotonin type 3 receptor antagonists and probiotics was statistically and significantly higher in primary and secondary healthcare institutions (P = 0.030).
Table 6
Responses pertaining to the treatment provided to patients with irritable bowel syndrome, by type of practice
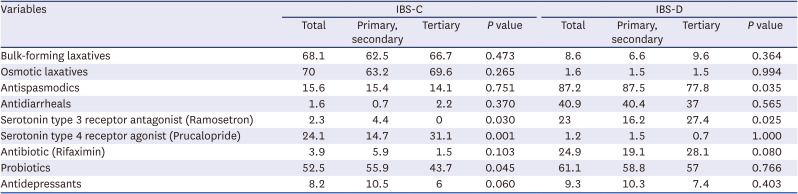
Bulk-forming laxatives, osmotic laxatives, and serotonin type 4 receptor agonist (prucalopride) were cited as effective for alleviating the symptoms of IBS-C by 58% (n = 158), 78% (n = 213), and 80% (n = 215) of respondents, respectively. Regarding preferred bulk-forming laxatives, 65% (n = 175) of respondents preferred calcium polycarbophil, whereas 34% (n = 91) of respondents preferred psyllium husks. Regarding osmotic laxatives, 58% (n = 157), 31% (n = 85), and 10% (n = 26) of respondents preferred magnesium hydroxide, lactulose, and polyethylene glycol, respectively. Depending on the type of practice, the preference for polyethylene glycol was statistically and significantly higher at tertiary healthcare institutions, whereas the preference for lactulose and magnesium hydroxide was statistically and significantly higher at primary and secondary healthcare institutions (P = 0.001).
Treatment for patients with IBS-D
Table 6 shows, the item that allowed multiple answers for the drugs used as the first-line treatment for patients with IBS-D. The use of antispasmodics and probiotics was the main treatment of IBS-D. Antispasmodics were mainly used in primary and secondary healthcare institutions (P = 0.035). Depending on the type of practice, the use of antispasmodics was statistically and significantly higher at primary and secondary healthcare institutions, whereas the use of a serotonin type 3 receptor antagonist was statistically and significantly higher at tertiary healthcare institutions (P = 0.025). The use of loperamide as an antidiarrheal, ramosetron as the serotonin type 3 receptor antagonist, and rifaximin as an antibiotic was reported as being effective for alleviating the symptoms of IBS-D by 71% (n = 194), 77% (n = 205), and 56% (n = 150) of respondents, respectively. Answers for the dose and period rifaximin administration varied: 200 mg, three times a day for one week, 34% (n = 92) respondents; 200 mg three times a day for two weeks, 35% (n = 95) respondents; 400 mg, three times a day for one week, 13% (n = 36) respondents; and 400 mg, three times a day for two weeks, 17% (n = 45) respondents. A statistically significant difference was observed according to the type of practice (P < 0.001). In primary and secondary healthcare institutions, the administration of 200 mg three times a day for one week was reported by 51.1%, and the administration of 400 mg three times a day for two weeks was reported by 30.1% of the respondents; a one-week regimen was most commonly administered, despite the differences in doses. In tertiary healthcare institutions, the administration of 400 mg three times a day for one week was reported by 40.7%, and that of 400 mg three times a day for two weeks was reported by 28.1% of the respondents; the administration of 400 mg was primarily reported, despite differences in the period of administration.
In IBS-constipation predominant subtype, osmotic laxatives and bulk-forming laxatives were mostly used and effective (Table 6). In IBS-diarrhea predominant subtype, antispasmodics and probiotics were mainly used.
Other treatments
Antispasmodics
Regarding the effectiveness of antispasmodics in alleviating symptoms in patients with IBS, 84% (n = 229) respondents gave a positive answer. For the item allowing multiple answers for preferred drugs, trimebutine maleate, tiropramide, otilonium bromide, pinaverium bromide, cimetropium bromide, hyoscine (scopolamine) butylbromide, alverine citrate, phloroglucinol, fenoverine, and mebeverine was selected by 79% (n = 214), 59% (n = 159), 39% (n = 106), 29% (n = 79), 21% (n = 56), 15% (n = 41), 12% (n = 33), 11% (n = 29), 5% (n = 13), and 1% (n = 2) of respondents, respectively.
Probiotics
Regarding the item on the IBS symptoms that were alleviated by the use of probiotics, 68% (n = 186) of respondents cited abdominal distension and hard stools.
Antidepressants
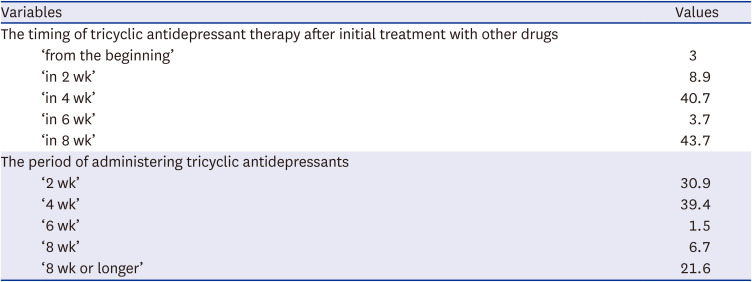
Three questions in the survey assessed the focus on psychological symptoms in the medical history of patients with IBS. Regarding the item on whether the administration of tricyclic antidepressants was effective in alleviating IBS-related pain, 72% (n = 195) of respondents gave a positive answer. Table 7 shows the timing of tricyclic antidepressant therapy after initial treatment with other drugs, and the period of administering tricyclic antidepressants. The most frequently obtained answers for the timing of administration after the initiation of pharmacological therapy were ‘in four weeks’ and ‘in eight weeks.’ The most frequently obtained answer for the period of administering tricyclic antidepressants was ‘Two or Four weeks.’ A statistically significant difference was observed according to the type of practice (P < 0.001), and the administration period was most frequently within four weeks; among those from primary and secondary healthcare institutions, 45.5% cited two weeks and 38.1% reported four weeks, whereas among those from tertiary healthcare institutions, 41% cited four weeks, and 29.9% reported eight weeks or longer.
Table 7
The timing of tricyclic antidepressant therapy after initial treatment with other drugs and the period of administering tricyclic antidepressants (N = 272)
DISCUSSION
As there is no specific biological marker for IBS that can be used to objectively diagnose and treat IBS, this condition is differentiated from other functional digestive diseases based on the symptoms reported by the patient and changes in bowel habits; the effectiveness of treatment is also evaluated in the same manner. Although the Rome IV criteria are diagnostic, the process of drawing an objective diagnosis based on the subjective symptoms experienced by patients may differ for each doctor.
Doctors with various specializations participated in the survey, though a particularly high participation rate was observed for internal medicine specialists (97%, n = 263 respondents). The survey was conducted at primary, secondary, and tertiary healthcare institutions throughout the country to investigate the overall status of the diagnosis and treatment of IBS. Doctors of 80.9% defined IBS according to the new Rome IV criteria revised in 2016 as a chronic and complex disease with complex symptoms such as abdominal pain, discomfort, bloating, and changes in bowel habits for at least six months, or as a chronic digestive functional disease characterized by repetitive abdominal pain and swelling, soft stools, and diarrhea or constipation without excessive inflammation and structural or biochemical abnormalities.
According to the guidelines for the treatment of IBS in Korea, colonoscopy is recommended for patients aged 50 years or older, patients with a family history of colorectal cancer, or patients with warning symptoms.1718 The results of the survey indicated that approximately 70.6% of the doctors performed colonoscopy in more than 40% of patients suspected of having IBS. Colonoscopy was performed in cases with indications as described by specific guidelines (37.9%), and in cases of ineffective treatment with medication (38.6%). Colonoscopy was also performed at the patient’s request or for a health check-up in 23.5% of the cases. This seems rather high considering that the prevalence of structural abnormalities that can be diagnosed by colonoscopy in patients with IBS is low, and that the rate of colonoscopy in studies conducted in other countries is approximately 11–45%.1920 This may have been due to the relatively high accessibility of colonoscopy in South Korea.
Patients with IBS are treated for a possible cause based on the symptoms they exhibit, or by selecting a drug that improves the symptoms. Various therapeutic methods have been tried such as a low-FODMAP diet, exercise, probiotics, antibiotics including rifaximin, antispasmodics, antidepressants, drugs to control diarrhea and constipation, and transplantation of stool flora. Therefore, healthcare institutions are likely to make various choices depending on the preferred drugs, feedback from patients, availability of drugs, and insurance coverage.
A previous study reported that a low-FODMAP diet improves symptoms by 70% in patients with IBS,21 and a meta-analysis has reported that such a diet helps improve IBS-related abdominal pain and distension.22 In this study, 60% (n = 164) of respondents answered that they educated the patients on the low-FODMAP diet, and recommended adherence to such a diet; 60% (n = 163) of respondents reported that abdominal distension was the symptom that showed the most prominent improvement with a low-FODMAP diet. These results agree with the results of previous studies; however, the results of this study cannot be generalized as they are not based on IBS-related rating scales, and were obtained based on the experience and memory of clinical practitioners. There is a need for a domestic multi-center randomized controlled study on symptomatic improvement in patients with IBS who switch to a low-FODMAP diet.
In patients with IBS-C, osmotic and bulk-forming laxatives were most frequently prescribed to improve constipation as first-line treatment17 In IBS-C patients, bulk-forming laxatives were expected to improve the symptoms, and osmotic laxatives were expected to increase the frequency of defecation. Prucalopride, a serotonin type 4 receptor agonist, selectively acts on the serotonin type 4 receptor to promote intestinal motility, improve the slow bowel function, and shorten the transit time in the gastrointestinal tract by facilitating bowel movements.2324 In this study, 79% (n = 215) of respondents answered that a serotonin type 4 receptor agonist was effective in alleviating the symptoms in patients with IBS-C.
Loperamide, an antidiarrheal drug, was helpful for patients with IBS-D, as indicated by 71% (n = 195) of respondents. Loperamide is a synthetic opioid receptor agonist that acts directly on the intestinal plexus to inhibit intestinal peristalsis and secretion, and is commonly used for treating IBS-D. Ramosetron, a serotonin type 3 receptor antagonist, helped alleviate the symptoms of IBS-D, as indicated by 75% (n = 205) of respondents. Ramosetron acts on the intestinal plexus to prolong the colon transit time, slows the gastric-colon reflex, and reduces rectal sensitivity and postprandial motility to improve bowel movements and reduce the frequency of defecation. It is effective in the treatment of IBS-D, with no difference in effect according to sex. Several studies have revealed that abnormalities in bacterial flora or intestinal inflammation are associated with worsening IBS symptoms.2526 In our study, the use of the serotonin type 4 receptor agonist was statistically and significantly higher in tertiary healthcare institutions (P = 0.001), whereas the use of serotonin type 3 receptor antagonist and probiotics was statistically and significantly higher in primary and secondary healthcare institutions (P = 0.030). The result has suggested a treatment of serotonin type 3 receptor antagonists resulting a global improvement in IBS symptoms and relief of abdominal pain and discomfort, and can be easily used in primary and secondary healthcare institutions.27 The use of rifaximin, a non-absorbable antibiotics, improves abdominal pain and bloating symptoms in patients with IBS other than IBS-C.2829 According to the results of this survey, most doctors responded positively regarding the use of rifaximin for the treatment of patients with IBS-D. Regarding the dose, 69% (n = 187) of respondents (one week: 92 respondents, two weeks: 95 respondents) answered that they administered 200 mg three times a day. The recommended rifaximin dose is 800–1,200 mg per day for 10 days or 1,650 mg per day for two weeks in patients with IBS.30 Most doctors seemed to use it in low doses or only for short periods of time. This might be because the current insurance plan in South Korea only covers rifaximin for treating enteritis and hyperammonemia. Obtaining an insurance license for the use of rifaximin for IBS in the future will be necessary. In addition, sufficient education on the appropriate dose and duration of prescription is required.
A total of 84% (n = 229) of respondents answered that the use of antispasmodics helped relieve symptoms in patients with IBS. Various antispasmodics including non-selective anticholinergic agents (used to block the action of the excitatory neurotransmitter acetylcholine in the gastrointestinal tract), muscarinic receptor blockers, calcium channel blockers, and opioid receptor modulators are very commonly used in the treatment of IBS. Antispasmodics reduce pain by weakening the basal and postprandial contractility of smooth muscles in the gastrointestinal tract of patients with IBS-D.31
The use of probiotics improved abdominal distension and hard stools according to 34% (n = 93) and hard stools 34% (n = 93) of respondents, respectively. As abnormalities in the intestinal flora have been suggested to contribute to the pathophysiology of IBS, probiotics have been used to restore intestinal flora to a normal state. Probiotics improve the condition of the colonic mucosa and restore the intestinal barrier by regulating the intestinal flora. In several studies, probiotics improved the overall symptoms of IBS such as abdominal distension and bloating, compared to the placebo group.3233 Nevertheless, obtaining consistent results is difficult due to the heterogeneity among studies based on the topics examined, the probiotic strains used, and the dosage of probiotics.
Psychiatric problems affect IBS, and depression and anxiety are associated with IBS.3435 If abdominal pain persists and symptoms do not improve despite repeated administration of first-line drugs, antidepressant medication is considered. A previous meta-analysis revealed that the administration of antidepressants improved abdominal pain and IBS scores.3637 It is recommended that a low dose should be administered initially, and the dose should be increased gradually.1217 In this study as well, 71.4% of the participants responded that the administration of tricyclic antidepressants helped relieve IBS-related pain. The use of tricyclic antidepressants was recommended as second line treatment in most guidelines for IBS.1238 Regarding the timing of administration after the initiation of pharmacological therapy, the most frequently obtained answers were ‘in four weeks’ (40% n = 110 respondents) and ‘in eight weeks’ (43%, n = 118 respondents). Nevertheless, approximately 21.3% of the doctors used antidepressants for eight weeks or longer. Tricyclic antidepressants are not expected to have a rapid effect. However, compared to the evaluation of response at 8 or 12 weeks in most studies, tricyclic antidepressants were reported to have only been used for a short period.39 This might be due to the adverse effects of tricyclic antidepressants including dry mouth and acute urinary retention. Selective serotonin reuptake inhibitors (SSRIs), which have fewer adverse effects, may be administered. However, it is difficult to prescribe SSRIs for more than two months, except for diseases treated at mental health departments, due to current insurance regulations in South Korea.
We compared the diagnosis and treatment patterns at primary, secondary, and tertiary institutions. Many differences were observed between the groups by statistical analysis. First, the rate of colonoscopy was high in tertiary healthcare institutions. ‘Ineffective treatment with medication’ as the reason for performing colonoscopy was higher among physicians in primary/secondary institutions, while ‘changes in bowel habits in patients aged 50 years or older’ was higher among physicians in tertiary institutions. During a colonoscopy, the necessity of random biopsy was higher among physicians who worked at tertiary institutions. Second, ‘The patient did not adhere to the diet’ as the reason for ineffectiveness using treatment of low-FODMAP diet was that higher among physicians in primary/secondary institutions, while ‘There are individual differences in terms of effectiveness’ was higher among physicians in tertiary institutions. Third, in the IBS-constipation predominant subtype, the use of serotonin type 3 receptor antagonist (ramosetron) and, probiotics was higher among physicians in primary/secondary institutions, while the use of serotonin type 4 receptor agonists was higher among physicians in tertiary institutions. Fourth, in the IBS-diarrhea predominant subtype, the use of antispasmodics was higher among physicians in primary/secondary institutions, while the use of serotonin type 3 receptor antagonist (ramosetron) was higher among physicians in tertiary institutions.
The study had some limitations. First, this survey was conducted through voluntary participation of doctors working at each healthcare institution. The tendencies of the participating doctors might form a biased opinion, and it may not be possible to represent all domestic doctors treating IBS. The study questionnaire was answered anonymously, and efforts were made to gather opinions sufficiently without being biased by the region or level of healthcare institution, as much as possible. Second, while prescriptions were usually issued based on the name of the product or ingredient, the drugs were indicated by sub-categories of ingredients (e.g., serotonin type 3 receptor antagonist) in the questionnaire, and some respondents may be unfamiliar with this terminology. Third, reflecting the diverse tendencies of the respondents is difficult as the questionnaire was multiple-choice and the classification of the range of questions contained the subjective tendencies of the authors. However, there were numerous categories based on specific ingredient names or product names; therefore the questionnaire may not have indicated representative drugs.
In conclusion, the overall perception of IBS treatment and the clinical treatment patterns of various doctors from primary to tertiary healthcare institutions were analyzed based on the results of the survey. In the IBS-constipation predominant subtype, osmotic and bulk-forming laxatives were mostly used and effective. In the IBS-diarrhea predominant subtype, antispasmodics and probiotics were mainly used. Notable differences were observed between physicians in primary/secondary and tertiary institutions regarding the rate of colonoscopy, the necessity of random biopsy, the reason for the ineffectiveness of low-FODMAP diet, and use of drug therapy in IBS. In South Korea, IBS is mostly diagnosed and treated according to the Rome IV criteria as revised in 2016. Guidelines for the diagnosis and treatment should be continuously updated, and doctors need to be educated in this regard
 XML Download
XML Download