

 PDF
PDF Citation
Citation Print
Print



Carbon monoxide (CO) poisoning was common in Korea in the past because coal briquettes were often used for heating in households. Since the 1990s, CO poisoning has decreased as other fuel sources have replaced coal briquettes.1 According to the Korean Statistical Information Service, the proportion of briquette boilers in Korean household heating systems decreased from 13.2% in 1995 to 4.1% in 2019.2 However, as more people have chosen camping as a recreational activity in recent years, the number of patients visits to emergency department (ED) for CO poisoning by reckless usage of camping supplies, like fuel or heating appliances, has also increased.3 Moreover, CO poisoning has emerged as an significant suicide method in Korea after the suicidal death of a famous actress in 2008, increasing 30-fold between 2006 and 2012.4
CO binds to hemoglobin to form carboxyhemoglobin, which produces various systemic and neurological complications from tissue hypoxia.56 The majority of patients with CO poisoning are classified as mild to moderate in severity; however, severe symptoms such as convulsion and cerebral infarction may also occur, leading to death. Hyperbaric oxygen therapy (HBOT) has been used as a treatment method for CO poisoning to minimize these complications.78 In Korea, as the number of hospitals with hyperbaric oxygen chambers is gradually increasing, HBOT is administered to patients with CO poisoning more frequently, as well as for various other indications.9
There have been several studies on CO poisoning in Korea,1011 but few on the prevalence of CO poisoning and status of HBOT provision based on nationwide data. We investigated the prevalence of CO poisoning and the provision of HBOT from 2010 to 2019, based on the National Health Insurance claims data.
This study analyzed patients who attended hospitals for CO poisoning over 10 years (2010–2019), based on the total population data of approximately 50 million people, along with claims data from the Health Insurance Review and Assessment Service (HIRA). Korea has adopted a single health insurance system led by the government, consisting of the National Health Insurance (approximately 97% of the population) and medical benefits (for the remaining 3%; low-income class).12
The HIRA is an independent Korean government agency that evaluates medical claims data from all medical institutions in Korea. Using this claims data, the authors collected demographic and medical information regarding diagnosis, procedure, and prescription. Because the HIRA data is transmitted anonymously, researchers are not aware of potentially identifiable personal information.
The 7th edition of the Korean Classification of Diseases, which revised the 10th edition of the International Classification of Diseases to match the Korean healthcare system, is used when Korean medical insurance claims are submitted to the HIRA. The database was searched from 2010 to 2019 to retrieve records of patients with codes related to CO poisoning (T58, X47*, X67*, X88*, and Y17*) and HBOT (M058* and M586*). The prevalence rate, according to the age and gender of patients and the province and the number of hospitals providing HBOT, was investigated annually. Population numbers were collected from the national statistics portal by region, year, age, and sex.2
The prevalence of CO poisoning and the provision of HBOT were calculated as the number of cases per 10,000 people. The annual prevalence was calculated as the point prevalence, and the overall prevalence by age, gender, and region was calculated as the period prevalence. Treatment time of HBOT is classified based on the treatment codes: for example, up to 1 hour (M0581, 0586); over 1 hour, up to 2 hours (M0582, 0587); and over 2 hours (M0583, 0588). The M586* code was used until June 2017; since then, the M058* code has been used for HBOT. The duration of HBOT was calculated as the total treatment time over 1 year. Data were analyzed using the SAS software (version 9.4; SAS Inc., Cary, NC, USA).
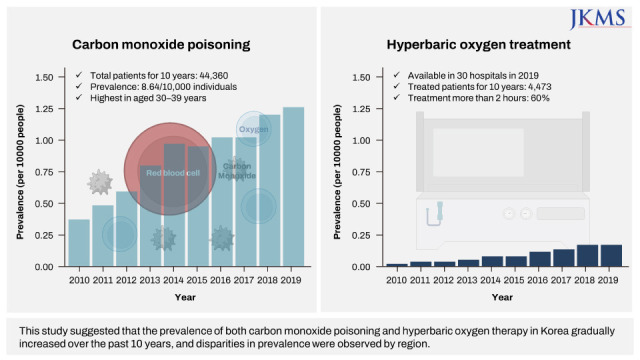
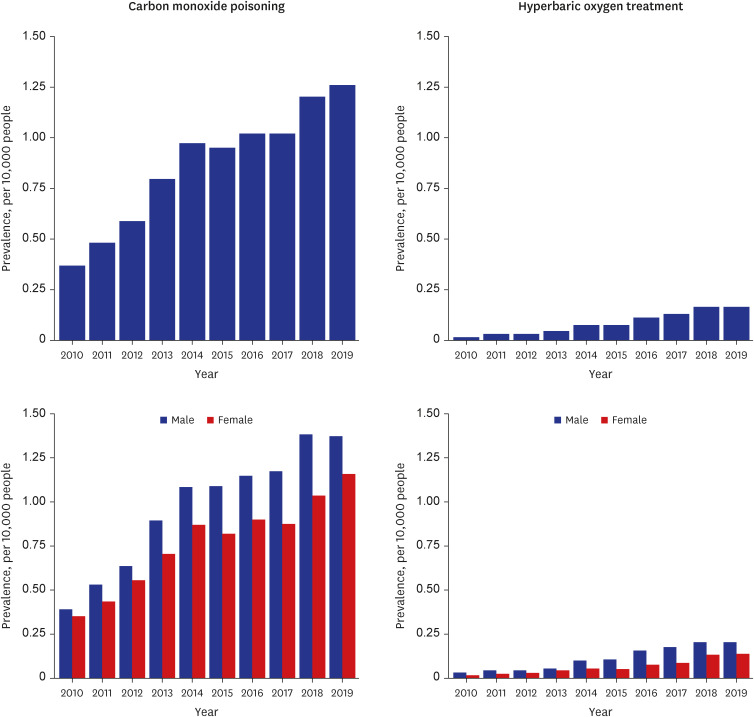
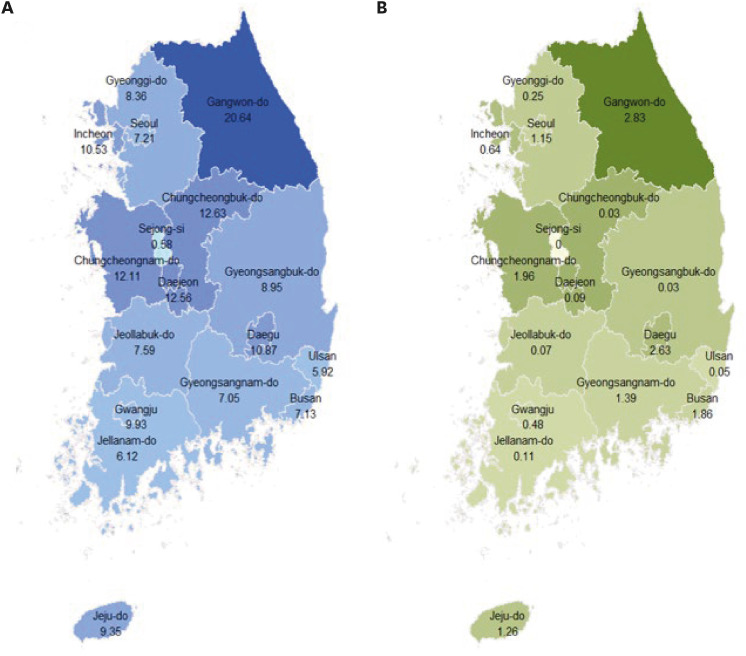
The prevalence of CO poisoning was 8.64 per 10,000 people (9.62 for men and 7.66 for women). The highest prevalence was 11.01 in those aged 30–39 years (13.43 for men and 8.48 for women, Supplementary Table 1). The prevalence by year was 0.37 in 2010 and 1.26 in 2019, showing a gradual increase (Fig. 1). By region, the Gangwon province had the highest period prevalence at 20.64, followed by Chungcheongbuk-do at 12.63 (Fig. 2A). In the previous study,10 Seoul and the Gyeonggi province were found to have the highest number of patients with CO poisoning. However, since these metropolitan areas have large populations, Gangwon had a high period prevalence per population. The reasons for the high prevalence in the Gangwon province can be partly attributed to differences in heating methods and increased outdoor activities, such as camping. Regarding the heating method by region in 2019, the proportion of coal briquette boilers was 3.6% in Gyeonggi, compared with 6.2% in the Gangwon province.2
A total of 4,473 patients (10.1% of CO poisoning) received HBOT over 10 years. The frequency was the highest among individuals aged 30–39 years. Overall, men (63.5%) received more HBOT than women. Comparing the provision of HBOT per population by region, Gangwon and Daegu showed the highest rates (Fig. 2B). In 2019, there were two multiplace and four monoplace HBOT chambers in the Gangwon province, which was the second most widely equipped following Jeju province. In 2010, 15 hospitals claimed the HBOT for patients with CO poisoning; however, the number of hospitals gradually increased to 19 in 2017 and 30 in 2019. In this study, patients who received HBOT only for CO poisoning were included. However, 14,995 patients received HBOT from various indications in 2019, and the number of institutions capable of HBOT at more than 2 atm increased to 50 in 2021.9
The prevalence of CO poisoning was found to be increasing in this study. The CO poisoning has gradually been decreasing in developed countries such as the United States and the United Kingdom,1314 while it still be a public health problem in countries that uncontrolled heating systems like coal stoves and hot water heaters are mainly used.15 The cause of CO poisoning can be classified by intentionality. In Korea, intentional cause has been reported in 35–44% of CO poisoning.1011 A study using the nationwide ED data from 2014 to 2018 reported that 35% of patients with CO poisoning visited to EDs were due to intentional poisoning.10 Another study from 20 EDs from 2011 to 2014 reported that intentional cause accounted for 44% of all CO poisoning cases.11 Suicidal death by CO poisoning started to increase from 0.5/100,000 people in 2008 to 3.2 in 2013 and 3.9 in 2019. As a result, gas poisoning has become the third highest method of suicide since 2013, following hanging and falling. Suicide by CO poisoning is more common in men (80.3%), especially those aged 25–44 years.16 The age-standardized suicide rate (per 100,000 people) for CO poisoning by region were equally highest in Gangwon, Daejeon, and Ulsan (4.8/100,000).17 To prevent suicide by CO poisoning, it is recommended that the quality of burning charcoal should be improved to weaken the toxicity and that mass media guidelines for reporting suicide events of influential people should be followed.18 The charcoal restriction program has shown no effect on suicide reduction by charcoal-burning or overall suicides.19
Since unintentional CO poisoning tends to increase in winter,11 it is estimated that the most common cases are caused by incomplete combustion of heating appliances. In December 2018, high school students were poisoned by CO due to a poorly constructed gas boiler at a pension house in Gangwon province, drawing significant social attention. Mandating CO detectors in residence areas has been found to be cost effective.2021 The odds of CO poisoning were 3.2 times higher (95% confidence interval, 1.5–6.9) among those who had no CO detector than had detector with an alarm.22 In Korea, it has become mandatory to install CO detectors in lodging facilities since August 2020.
This study has some limitations. First, the HIRA data only provided the disease codes and demographic information. Thus, there were no data available on the details of cause of poisoning, intentionality, and clinical progress. Second, the number of patients may have been overestimated when patients were transferred for reasons such as the absence of HBOT equipment. Further studies on the exact causes and factors affecting the prevalence of CO poisoning are required.
This study suggests that there is an increased trend in the prevalence of patients with CO poisoning in Korea, and that the number of patients who received HBOT and hospitals capable of HBOT has also increased. We also found differences in the prevalence of CO poisoning and HBOT provision per population according to the region, and interventions to mitigate these disparities should be conducted in the future.
 XML Download
XML Download