

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Worldwidely, the number of hypertensive patients continues to increase. In the meantime, many antihypertensive drugs have been developed, but the blood pressure (BP) control rate of hypertensive patients is insufficient. Even in previous studies, the risk reduction of cardiovascular complications due to hypertension is still not enough.1 Due to the high prevalence of hypertension and the risk of cardiovascular complications from hypertension, recent hypertension guidelines emphasize stronger and aggressive control of BP.2
Resistant hypertension is a case in which BP is not properly controlled even with three or more antihypertensive drugs, and it is not easy to properly maintain the BP in these patients. It is estimated that 8–30% of hypertensive patients worldwide are the patients with resistant hypertension.3456 These patients are known to be associated with poor BP control, high incidence of hypertension complications such as target organ damage and poor clinical prognosis.7 Moreover, patients with resistant hypertension had a higher cardiovascular mortality risk compared to the other hypertensive patients, regardless of BP control.8 Considering that resistant hypertension is associated with various pathophysiological and demographic factors, it is important to understand the clinical characteristics of these patients and to establish an appropriate treatment strategy according to the patient characteristics.
Previously, differences in clinical features and treatment pattern between men and women in hypertensive patients have been reported. For example, the prescription rate for angiotensin-converting enzyme (ACE) inhibitors in women was lower than in men.9 Dry cough, which could lower drug adherence, is more common in women than in men when taking ACE inhibitors.1011 In LIFE study, losartan had more side effects in women than man, but fewer losartan-induced serious adverse events, suggesting that anti-hypertensive drugs have a gender specific side-effect profile.12 Ultimately, the difference between men and women may affect the cardiovascular outcome. Although recent clinical trials (SPRINT and Hygia) showed no gender-difference in clinical outcomes,1314 there have been limited studies on gender difference in resistant hypertension.
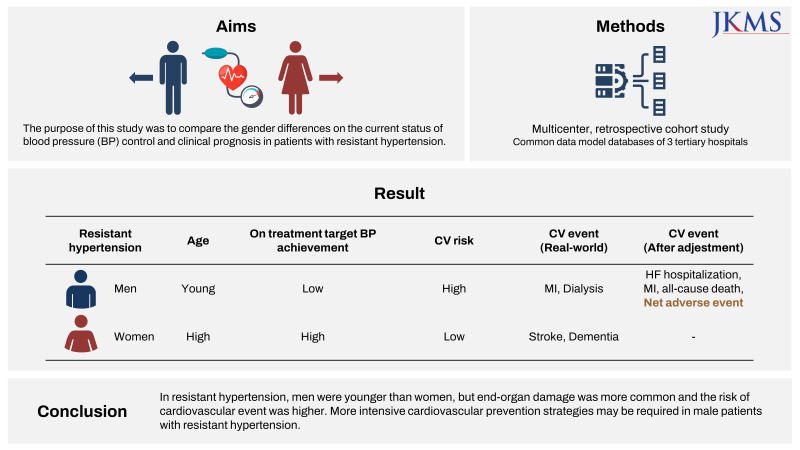
This study analyzed the clinical characteristics and prognosis according to gender in resistant hypertension patients, and further explored the potential factors affecting the prognosis and treatment patterns.
METHODS
Study design and data extraction
This is a multicentered retrospective cohort study of the Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM) database of three tertiary hospitals in Korea. The OMOP-CDM database is a clinical research database built on the basis of electronic health records (EHRs) of medical institutions, and consists of a common database structure, terminology adopted from various standard vocabulary systems, and corresponding concept id codes. The OMOP-CDM database of three tertiary hospitals was stored in Microsoft’s Structured Query Language (SQL) server, and the dataset for this study was extracted through direct query using SQL. The OMOP-CDM concept id information used in this study was provided in Supplementary Table 1.
Study population
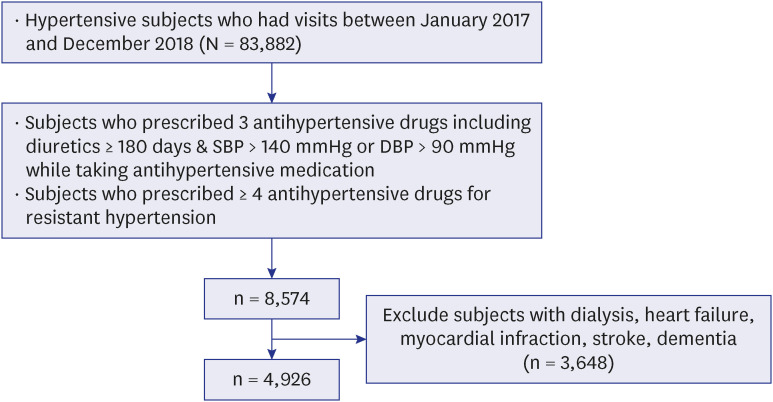
Patients with resistant hypertension who met the following criteria were selected among patients who had visits from January 1, 2017 to December 31, 2018. 1) The patients who were prescribed 3 or more class antihypertensive drugs including diuretics for 180 days or more within the first year, and had high BP with systolic blood pressure (SBP) of 140 mmHg or higher or diastolic blood pressure (DBP) of 90 mmHg or higher while taking 3 or more class antihypertensive medication after the index date, or 2) the patient who were prescribed 4 or more different class antihypertensive drugs for more than 180 days within the first year were included. The index date was the first day of overlapping drug exposure of antihypertensive drugs prescribed for resistant hypertension. Patients diagnosed with dialysis, heart failure (HF), myocardial infarction, stroke, or dementia before the index date were excluded. Finally, 4,926 patients with resistant hypertension were selected for this study (Fig. 1).
Definitions and study endpoints
Diabetes mellitus was defined as taking oral hypoglycemic agents or insulin for more than 180 days, HbA1c ≥ 6.5%, glucose ≥ 126 mg/dL or having diagnosis codes for diabetes mellitus. Dyslipidemia was defined as taking statin or ezetimibe for more than 180 days, serum total cholesterol ≥ 240 mg/dL, low-density lipoprotein-cholesterol ≥ 160 mg/dL, triglyceride ≥ 200 mg/dL, high-density lipoprotein-cholesterol (HDL-C) < 40 mg/dL or having diagnosis codes for dyslipidemia. Chronic kidney disease (CKD) was defined as the estimated glomerular filtration rate < 60 mL/min/1.73 m2 or proteinuria ≥ 1+ in routine urine analysis. Cardiovascular risk was estimated with the Systematic Coronary Risk Evaluation 2 (SCORE2) model and classified into low to moderate, high and very high.15 Target BP achievement was defined as SBP < 130 mmHg and DBP < 80 mmHg in patients younger than 65 years, and SBP < 140 mmHg and DBP < 80 mmHg in patients ≥ 65 years of age.16 Left ventricular hypertrophy (LVH) was defined when one or more of R amplitude in aVL, Sokolow-Lyon criteria, Cornell voltage criteria, and Romhilt-Estes criteria on electrocardiogram was positive. Proteinuria was defined as protein 1+ or higher in routine urine analysis.
HF hospitalization was defined as a case of more than 3 days of hospitalization including emergency room and NT-proBNP ≥ 300 pg/mL measured during hospitalization.17 Myocardial infarction was defined as chest pain or dyspnea during hospitalization and an increase in CK-MB level (> 99th percentile upper reference limit) of 2 or more times. Stroke was defined as diagnosis codes for cerebral infarction. Dementia was defined as diagnosis codes. Net adverse events were a composite of all-caused death, dementia, stroke, myocardial infarction, hospitalization for HF and dialysis.
Statistical analysis
Baseline characteristics are shown as the mean ± standard deviation or number (%). Chi-square test and Student’s t-test were used to compare the categorical variables and continuous variables between gender. To evaluate the difference in on-treatment BPs and control rate during the follow-up period between men and women adjusted for age, we used linear regression. The probabilities for 3-year clinical outcomes were calculated by the Kaplan-Meier curves and compared by log-rank test. Multivariable Cox proportional hazards regression analysis was performed to evaluate the relationship between gender and 3-year clinical outcomes. Age, SBP, DBP, anti-hypertensive medications, diabetes mellitus, dyslipidemia, CKD, alcohol, smoking, laboratory findings were considered as the potential confounding variables. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) program and R program (ver 3.6.1; R Foundation, Vienna, Austria).
Ethics statement
The study was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital (IRB No. 2021AN0450). Written informed consent was waived due to the use of a retrospective study design of anonymized data with minimal risk to study subjects. The study also complied with the Declaration of Helsinki. All data and supporting materials have been provided with the published article.
RESULTS
Baseline demographic and clinical characteristics of resistant hypertension was shown in Table 1. Male patients with resistant hypertension were younger, consumed more alcohol, and smoked more. Baseline SBP did not differ between men and women, but DBP was lower in women (82.8 ± 13.6 vs. 77.0 ± 12.7, P < 0.001). The prescription rate of antihypertensive drugs was compared for renin-angiotensin-system inhibitor, dihydropyridine-calcium channel blocker (DHP-CCB), diuretics, and beta-blocker. The prescription rate for DHP-CCB was higher in men than in women (84.0% vs. 81.1%, P = 0.006) and for other drug classes was not significantly different. In the laboratory test results, men had higher levels of hemoglobin, potassium, creatine, triglyceride, uric acid, glucose, and women had high levels of sodium, total cholesterol, and HDL-C. The cardiovascular risk estimated by SCORE2 score demonstrated that the proportion of patients with low-moderate risk was higher in women, the proportion of patients with high risk was higher in men, and the proportion of patients with very high risk was similar in men and women.
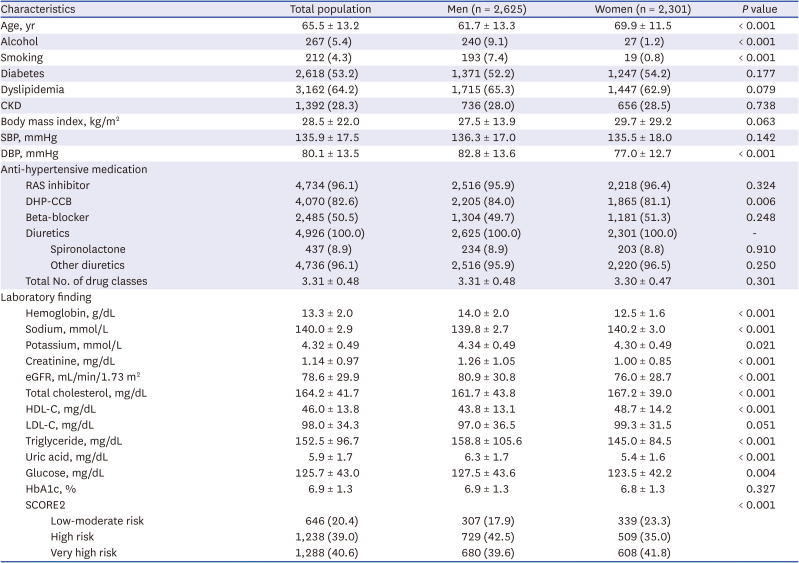
Table 1
Baseline characteristics of patients with resistant hypertension
Values are presented as mean ± standard deviation or number (%).
CKD = chronic kidney disease, SBP = systolic blood pressure, DBP = diastolic blood pressure, RAS = renin angiotensin system, DHP-CCB = dihydropyridine-calcium channel blocker, eGFR = estimated glomerular filtration rate, HDL-C = high-density lipoprotein-cholesterol, LDL-C = low-density lipoprotein-cholesterol, SCORE2 = Systematic Coronary Risk Evaluation 2.
![]()
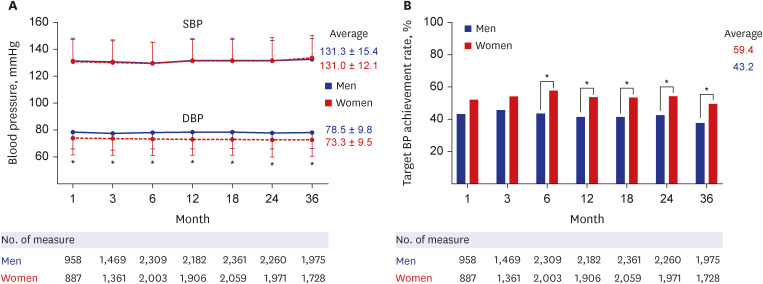
On-treatment BP measurement results were classified into 1, 3, 6, 12, 18, 24 and 36 months after the index date (Fig. 2). Average on-treatment SBP and DBP were 131.2 ± 11.9 mmHg and 76.1 ± 10.0 mmHg in total population. Average on-treatment SBP and DBP were 131.3 ± 11.7 mmHg and 78.5 ± 9.8 mmHg in men and 131.0 ± 12.1 mmHg and 73.3 ± 9.5 mmHg in women, respectively. On-treatment DBP was consistently lower in women than in men (P < 0.001). Thus, target BP achievement rate was significantly lower in men compared to in women (43.2% vs. 59.4%, P < 0.001).
Next, the prevalence and new incidence rates of LVH and proteinuria as subclinical cardiorenal complications were compared between men and women (Table 2). Both LVH and proteinuria showed higher prevalence in men than in women at baseline (27.0% vs. 19.3%, P < 0.001 for LVH; 33.9% vs. 23.4%, P < 0.001 for proteinuria). But their new 3-year incidence rate was similar.

Table 2
Comparison of subclinical cardiorenal complication between men and women
![]()
Table 3 and Fig. 3 shows the clinical results of male and female patients with resistant hypertension during the 3-year follow-up period. The incidence of dialysis and myocardial infarction was significantly higher in men than women (5.6% vs. 4.0%, P = 0.011 for dialysis; 3.4% vs. 2.1%, P = 0.009 for myocardial infarction). The incidence of hospitalization for HF was numerically higher in women than men, but there was no statistical difference (8.8% vs. 9.6%, P = 0.329). The incidence of stroke and dementia was higher in women than men (2.2% vs. 3.2%, P = 0.030 for stroke; 1.2% vs. 3.0%, P < 0.001 for dementia). The incidence of all-cause death was similar between men and women. Thus, the incidence of net adverse event showed no significant difference between men and women.
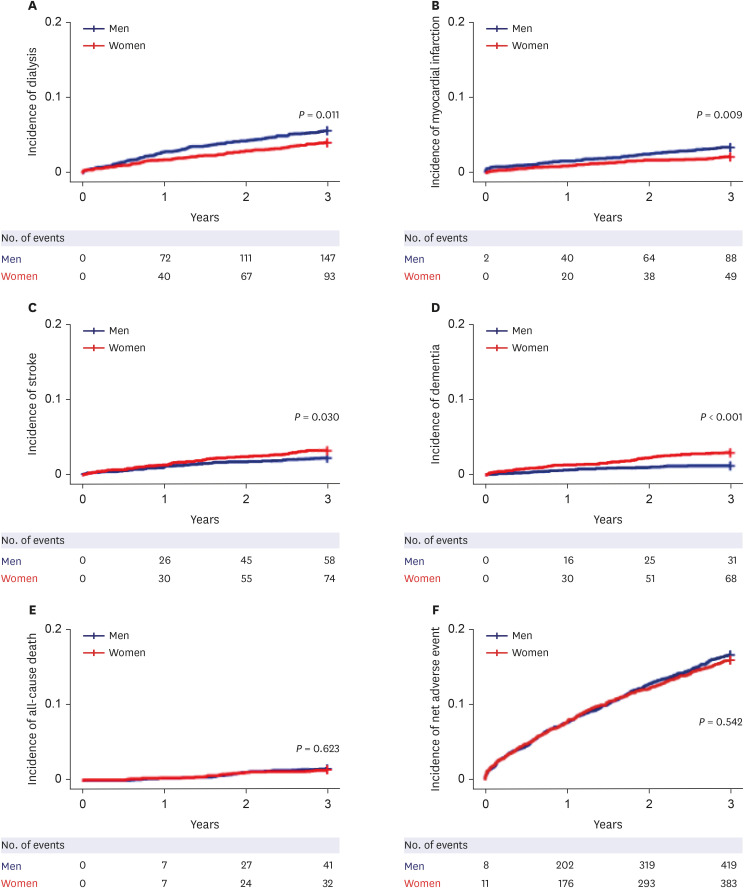
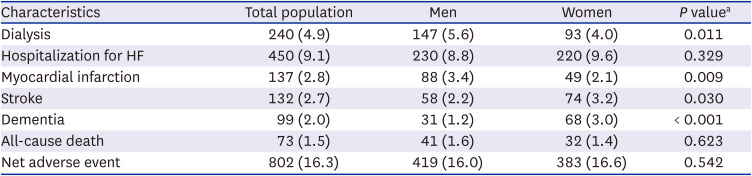
Fig. 3
Kaplan-Meier curves for clinical outcomes. (A) Dialysis; (B) Myocardial infarction; (C) Stroke; (D) Dementia; (E) All-cause death; (F) Net adverse event according to gender.
![]()
Table 3
Three-year clinical outcomes of the patients with resistant hypertension
Values are presented as number (%). Net adverse event is a composite of all-caused death, stroke, dementia, myocardial infarction, hospitalization for heart failure and dialysis.
HF = heart failure.
aP value for the log rank test.
![]()
Finally, multivariable Cox regression analysis was performed (Table 4). After adjusting for age, there was no difference in the risk of stroke and dementia between men and women (model 1). The risk of dialysis, hospitalization for HF, myocardial infarction, all-cause death and net adverse event was higher in men than in women. Similar results were obtained with additional adjustments for on-treatment BP and anti-hypertensive medications (model 2) and cardiovascular risk factors (model 3). Additionally, after adjusting for other potential confounding factors, the risk of hospitalization for HF, myocardial infarction, all-cause death and net adverse event remained higher in men than in women (model 4).

Table 4
Multivariable Cox regression analysis of men’s hazard ratio for clinical outcomes
Values are presented as hazard ratio (95% confidence interval). Net adverse event is a composite of all-caused death, stroke, dementia, myocardial infarction, hospitalization for heart failure and dialysis. Model 1: adjusted for age. Model 2: adjusted for model 1 plus on-treatment blood pressure and anti-hypertensive medication. Model 3: adjusted for model 2 plus alcohol, smoking, diabetes, dyslipidemia and CKD. Model 4: adjusted for model 3 plus body mass index and laboratory findings (hemoglobin, sodium, potassium, creatinine, total cholesterol, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol, triglyceride, uric acid and glucose.
HF = heart failure.
![]()
DISCUSSION
This is the first direct comparison of gender differences in patients with resistant hypertension using the EHR-driven CDM database. The summary of the results of this study is as follows. 1) Male patients with resistant hypertension were younger and had higher cardiovascular risk profile (e.g., SCORE2) than female patients. 2) The target BP achievement rate of male patients was lower than that of female patients, which is thought to be due to the higher DBP in male patients than in female patients. 3) Prevalence of subclinical cardiorenal complication (LVH and proteinuria) was also higher in male patients than in female patients, but the new 3-year incidence was similar among male and female patients. 4) Incidence of myocardial infarction and dialysis was higher in male patients, and incidence of stroke and dementia was higher in female patients. 5) After adjustment, male sex was an independent risk factor for net adverse event, which was driven by HF hospitalization, myocardial infarction and all-cause death, in patients with resistant hypertension (hazard ratio, 1.34; 95% confidence interval, 1.08–1.67).
Gender differences in demographic, lifestyle, and clinical aspects have been reported in resistant hypertension. The proportion of women was higher in patients with resistant hypertension.1819 Female patients with resistant hypertension have been reported to have lower BP control than male patients.18 However, recently, it is known that there is no difference in the BP control rate between men and women when taking antihypertensive drugs.20 In this study, there was no difference in SBP between men and women in the case of resistant hypertension, but the DBP was higher in men than in women. When the BP control rate was defined as the proportion of patients with SBP < 140 mmHg and DBP < 90 mmHg as in the previous studies, there was no gender difference in control rate in this study (74.6% for men vs. 77.1% for women, P = 0.511, data not shown). When the target BP achievement criteria of SBP < 130 mmHg (age < 65 year) or 140 mmHg (age ≥ 65 year) and DBP < 80 mmHg in the recent guidelines were applied, the overall target BP achievement rate was higher in women than in men (43.2% for men vs. 59.4% for women, P < 0.001, Fig. 2).
In the previous pooled analysis of the patients with resistant hypertension from SPRINT and ACCORD trials, an intensive BP target (SBP < 120 mmHg) treatment showed better cerebro-cardiovascular outcome compared to the standard target (SBP < 140 mmHg) treatment.2122 Mean on-treatment DBP of the patient in an intensive treatment arm was less than 70 mmHg. This suggested that intensive BP control would be important even in patients with resistant hypertension. For the patients in this study, further lowering of BP might be necessary in male patients as well as female patients.
End organ damage is the major surrogate for advanced hypertension and associated with poor cardiovascular outcome.23 Representative end organ damages include LVH for the heart and proteinuria for the kidney. Previous study pointed out that the relationship between BP and end organ damage would be bidirectional in resistant hypertension.24 Inappropriate BP control could lead to structural and functional changes including LVH and proteinuria, and hypertension becomes increasingly resistant to treatment.
In addition, end organ damage is closely related to the clinical prognosis. LVH in patients with resistant hypertension is an important predictor of cardiovascular prognosis.25 Previous literature review reported that there was no difference in the prevalence of LVH in hypertensive patients between men and women.2627 The prevalence of LVH according to gender has not been yet reported in resistant hypertension. In this study, the prevalence of LVH was higher in men than in women. Additionally, the incidence of new LVH was not different between men and women. Proteinuria is also an important risk predictor for end-stage renal disease as well as cardiovascular events in patients with resistant hypertension.282930 In addition, the proportion of men with proteinuria increased compared to that without proteinuria in patients with resistant hypertension.282930 Similarly, in this study, the prevalence of proteinuria was higher in men than in women. The incidence of new proteinuria was not different between men and women. In summary, the results of this study suggested that screening and regular check-up for LVH and proteinuria for women as well as men should be important in patients with resistant hypertension because the prevalence of end organ damage is higher in men than in women, but the occurrence of new end organ damage is as high as in women.
Poor cerebro-cardiovascular and renal prognosis in patients with resistant hypertension is well known.193132 Previous studies have shown that men have a poorer clinical prognosis than women in various cardiovascular diseases. However, reports of such gender differences in hypertensive patients are rare. Quan et al.33 reported gender differences in clinical prognosis in more than 900,000 multi-racial hypertensive patients. The risk of myocardial infarction, HF, stroke, and death was higher in male hypertensive patients than in female hypertensive patients, and myocardial infarction showed the greatest difference. In this study, the incidence of stroke and dementia was higher in female patients, but after adjusting for age, there was no difference in the risk of stroke and dementia. This suggested that the reason why the incidence of stroke and dementia was higher in women was probably because female resistant hypertension patients were older than men. And, after adjusting for age, on-treatment BP and anti-hypertensive medication, the risk of myocardial infarction and dialysis, as well as hospitalization for HF, all deaths, and net adverse events were significantly higher in men than in women. This difference could be due to other factors, not the difference in BP and BP control between men and women. After further adjustment for potential confounding factors including cardiovascular risk factors, the male factor remained significant for HF hospitalization, myocardial infarction, all-cause death, and net adverse event. This suggests that there are gender differences in intrinsic cardiovascular risk that we have not yet accounted for cardiovascular prognosis, and more intensive preventive strategies could be helpful in male patients with resistant hypertension.
There are severe limitations in this study. Unlike the prospective cohort study, this study is a retrospective study, and the possibility of unintentional selection bias in the sampling process cannot be excluded. Clinical definitions based on EHR data may overestimate or underestimate variables. For example, the smoking and alcohol consumption was lower than expected. And, although the patients included in this study were carefully selected from the EHR database based on the definition of resistant hypertension in the current clinical guidelines, some patients may not actually be the patients with resistant hypertension. Patients with white uncontrolled hypertension and secondary hypertension could not be excluded. Accurately identifying a patient with resistant hypertension is not easy even in routine clinical practice because it is necessary to sufficiently investigate various factors such as the patient's history and drug adherence. However, the other recent study of resistant hypertension showed BP similar to the present study (SBP/DBP 132.6/71.8 mmHg in the other study vs. 131.2/76.1 mmHg in this study), suggesting that the patients included in this study were eligible for resistant hypertension.34 The 8-year age difference between men and women in this study would have had a significant effect on BP and the prevalence of end-organ damage. Statistical age adjustment may not be sufficient to exclude confounding effects of age and other factors beyond our control. Lastly, since this study analyzed patients in tertiary hospitals, the results should not be interpreted as a generalization.
In conclusion, male patients with resistant hypertension were younger than female patients, but had a higher cardiovascular risk and a higher prevalence of end-organ damage such as LVH and proteinuria. After adjustment, there was a clear difference in 3-year net adverse event rate between men and women, particularly the risk of HF hospitalization, myocardial infarction, and all-cause death was significantly higher in men.
 XML Download
XML Download