

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Heart disease is the leading cause of death worldwide and responsible for an estimated 16% of the total global mortality.1 Although the total mortality rate of cardiovascular disease (CVD) in South Korea has significantly decreased, heart disease remains the second leading cause of death, and ischemic heart disease (IHD) mortality has continuously increased until recently.23 The increase in CVD burden is most likely due to the aging of the global population, accompanied by an increase in the prevalence of modifiable risk factors.34
Although most cases of CVD manifest clinically as an acute disease, they are actually chronic degenerative diseases that progress over time.5 Therefore, patients with CVD should receive cardiac rehabilitation (CR) after hospital discharge; however, the actual CR participation rate is approximately 20–40% even among countries with advanced medical care.6
A comprehensive CR program was introduced in South Korea in the late 1990s, and there has been a subsequent increase in CR participation. However, hospital-based CR has not been actively applied to eligible patients, and one report from 2017 showed that the CR participation rate among 26 CR-providing facilities was approximately only 1.5%.7 Currently, 47 (28.7%) of 164 hospitals that practice percutaneous coronary intervention (PCI) have CR programs; therefore, the number of CR facilities remains insufficient, and there are regional gaps when considering the number of IHD cases in South Korea.8 Furthermore, participation in CR remains consistently poor, except in several unique CR-specialized hospitals.
The purpose of this study was to investigate the actual nationwide practice rate of CR and its impact on clinical outcomes after acute coronary syndrome (ACS) using the medical claims data of the National Health Insurance Service (NHIS).9 To our knowledge, this is the first study to reveal the impact of CR on clinical outcomes after ACS and the dose-response relationship between the numbers of CR sessions attended and the risk of death and recurrence using a cohort of NHIS insurance claim data. This study demonstrates the actual status of CR in South Korea in terms of CR participation and adherence, possible regional and institutional gaps, and the number of CR sessions attended to date.
Go to : 
METHODS
Data sources
Data for this study were obtained from the NHIS database of South Korea. As a single-payer healthcare system, the NHIS provides obligatory health insurance for all residents of Korea, covering more than 97% of the country’s population (approximately 51 million people).10 In addition, the NHIS also operates the National Health Insurance Sharing Service to support policy and academic research using public health information.11 The NHIS database is a public database comprising patients’ socio-demographic data; medical claim codes; diagnoses confirmed by the International Classification of Diseases, 10th revision, Clinical Modification codes; and date of death.12 Access to the research data was approved by the Review Committee of the National Health Research Institutes.
Selection of participants
This nationwide retrospective cohort study was based on Korean NHIS (KNHIS) data recorded from January 1, 2017 to December 31, 2019. Inclusion criteria were as follows: all patients who were hospitalized for acute myocardial infarction (AMI) (I21, I22, I23, I25.2, and I25.5) or unstable angina (UA) (I20 and I24) and who underwent PCI or coronary artery bypass graft (CABG) surgery defined by the presence of one of the following claim codes: PCI (M6551, M6552, M6561, M6562, M6563, M6564, M6571, and M6572), CABG (O1641, O1642, O1647, OA641, OA642, OA647, O0161, O0170, and O0171), or thrombolysis (M6533 and M6534) during the index admission from January 1, 2017 to December 31, 2018. Exclusion criteria were any pre-existing conditions of AMI or UA from 2014 to 2016.
Measurement
CR attendance was defined by the presence of at least one claim code for MM451 (CR education), MM452 (CR evaluation), or MM453 (CR therapy), regardless of in- or outpatient status. To evaluate compliance to the CR program, data regarding CR attendance, grading of hospitals where CR was performed, and the frequency of each claim code were collected to assess CR education, CR evaluation (cardiopulmonary exercise [CPX] test), and CR therapy (monitoring exercise). We compared demographic data, diagnosis, type of intervention, and comorbidities between the CR and non-CR groups.
Cardiovascular outcomes
To compare the impact of CR on clinical outcomes after ACS, we checked the cardiovascular outcomes during the follow-up periods after index admission by using request data. Cardiovascular outcomes included all-cause death, recurred ACS, revascularization, cardiovascular readmission, and major adverse cardiovascular events (MACE) based on CR attendance. All-cause death was defined as death from any cause until December 31, 2019. ACS recurrence, revascularization, and cardiovascular readmission were defined as in Table 113 during the follow-up period, using the claim codes. MACE was defined as the composite of all-cause death, ACS recurrence, revascularization, and cardiovascular readmission. All cardiovascular outcome indices were obtained from the NHIS database using each claim code.
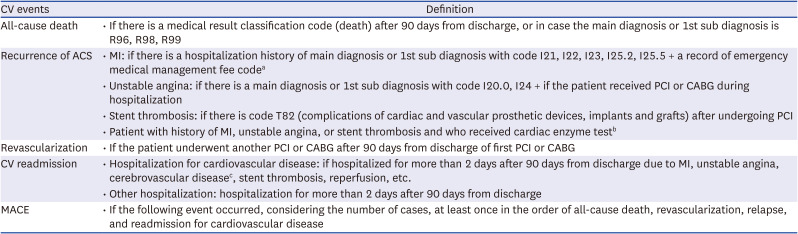
Table 1
Definition of clinical events
CV = cardiovascular, ACS = acute coronary syndrome, MACE = major adverse cardiovascular events, MI = myocardial infarction regardless of ST-elevation myocardial infarction or non-ST-elevation myocardial infarction, PCI = percutaneous coronary intervention, CABG = coronary artery bypass graft.
aEmergency medical management fee (AC101, AC103, AC105, V1100, V1200, V1300, V1400) or department of emergency medicine.
bTroponin-T (C3941), troponin I (C3942), creatine kinase-MB (B2640).
cHospitalization with I60–I69 without history of cerebrovascular disease.
![]()
Statistical analysis
A 1:1 propensity score (PS) matched analysis was conducted to minimize differences between the CR and non-CR groups using socio-demographic data (sex and age), diagnosis (disease code), comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease, cerebrovascular disease, cancer, and chronic obstructive pulmonary disease), and type of insurance. The balance of the study population’s characteristics was evaluated utilizing the absolute standardized difference. Baseline characteristics were summarized using descriptive statistics and presented as frequencies and percentages of patients or means with standard deviation. Kaplan-Meier survival curves and log-rank tests were utilized to compare the cumulative incidence rates of cardiovascular outcomes according to CR attendance. In addition, Cox proportional hazards regression analysis was used to estimate the hazard ratio (HR) of each cardiovascular outcome. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). P values of < 0.05 were considered statistically significant.
Ethics statement
Before the data were provided, the NHIS removed confidential and identifying information of all patients to protect their privacy. Therefore, this study was exempt from acquiring patients’ informed consent due to the de-identification of all personal information. The study protocol was approved by the Institutional Review Board (IRB) of the Inje University Haeundae Paik Hospital (IRB No. HPIRB 2019-05-028-003), and official approval was obtained from review and assessment committee of the National Health Insurance Servic (No. NHIS-2021-1-129). The data that support the findings of this study were available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Go to :
RESULTS
Characteristics of study participants
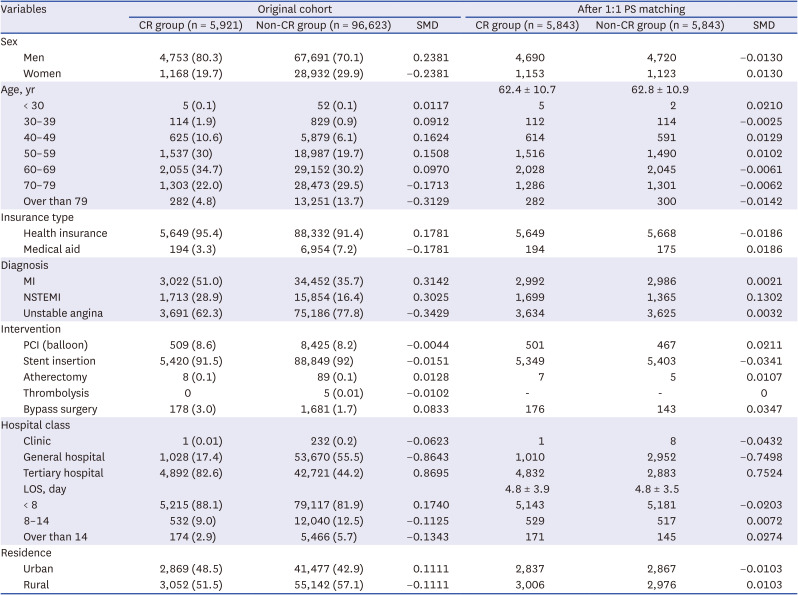
During the survey, a total of 163,581 patients were identified as potential study candidates; after excluding 61,337 patients based on the selection criteria, 102,544 patients were selected for the study. Fig. 1 depicts a flowchart illustrating the number of patients who met the inclusion criteria, the number of excluded patients, and the reasons for their exclusion. The patient characteristics are shown in Table 2. The standardized mean difference values of all characteristic variables were less than 0.1, indicating that there was no significant difference in patient characteristics between the two groups. In the original cohort, only 5,921 patients (5.8%) attended CR; 80.2% were male, and the mean age was 62.3 years, with most patients in their 60s, followed by those in their 50s. Of the 96,623 patients (94.2%) who did not attend CR, 70.1% were male, and the mean age was 66.8 years; most patients were in their 60s, followed by those in their 70s. Medical aid beneficiaries attended CR less than health insurance subscribers. The proportions of AMI and UA cases were similar in the CR group, but UA (77.8%) was more common than AMI (35.7%) in the non-CR group. CR was mostly implemented at tertiary hospitals (82.6%) and much less practiced at general hospitals (17.4%). The length of stay in acute hospital settings was longer in the non-CR group (5.52 ± 5.1 days) than in the CR group (4.8 ± 3.9 days). Patients living in urban areas were more likely to attend CR compared to those in rural areas. After 1:1 PS matching, no differences in patient characteristics were noted between the two groups (total, 11,686 patients) for almost all variables, except non-ST elevated myocardial infarction and tertiary hospital status, which were more common in the CR group. Comorbidities of the study participants are summarized in Table 3.

 | Fig. 1Flow chart showing the selection of subjects for this study.PCI = percutaneous coronary intervention, CABG = coronary artery bypass grafting, ACS = acute coronary syndrome, HIRA = Health Insurance Review & Assessment Service, CR = cardiac rehabilitation, MACE = major adverse cardiovascular events.
|
Table 2
Characteristics of study participants
Values are presented as number (%) or mean ± standard deviation.
PS = propensity score, CR = cardiac rehabilitation, SMD = standardized mean difference, MI = myocardial infarction regardless of ST-elevation myocardial infarction or non-ST-elevation myocardial infarction, NSTEMI = non-ST-elevation myocardial infarction, PCI = percutaneous coronary intervention, LOS = length of stay in acute hospital setting.
![]()
Table 3
Comorbidities of the study participants
PS = propensity score, CR = cardiac rehabilitation, SMD = standardized mean difference, CKD = chronic kidney disease, CVA = cerebrovascular disease including stroke and transient ischemic attack, COPD = chronic obstructive pulmonary disease.
![]()
Quality of participation among CR attendees of the original cohort
Only 5.84% (5,921) of the 102,544 study patients attended a CR program, either as an inpatient or outpatient. Table 4 shows the quality of participation among CR attendees (n = 5,921). In total, 83.58% of patients in the CR group underwent a CR evaluation that included the CPX test, but follow-up CPX tests were not frequently performed; 14.5% and 9% of patients in the CR group undertook the CPX test two and three times, respectively. Regarding monitoring, 3,145 patients (53.12% of the CR group) participated in an electrocardiogram (ECG) monitoring exercise at the hospital. However, over half of them (1,700 patients) participated in only one session; 1,136 patients participated in 2–10 sessions; 187 patients participated in 11–20 sessions; and only 117 patients (1.98% of the CR group) completed 20 or more exercise sessions at the hospital. Further, 46.88% of the patients in the CR group received a CR evaluation or education without exercise training at the hospital, and it is unknown whether the patients correctly adhered to a proper exercise protocol. According to the claim code of MM451, only 23.95% of patients in the CR group received CR education.
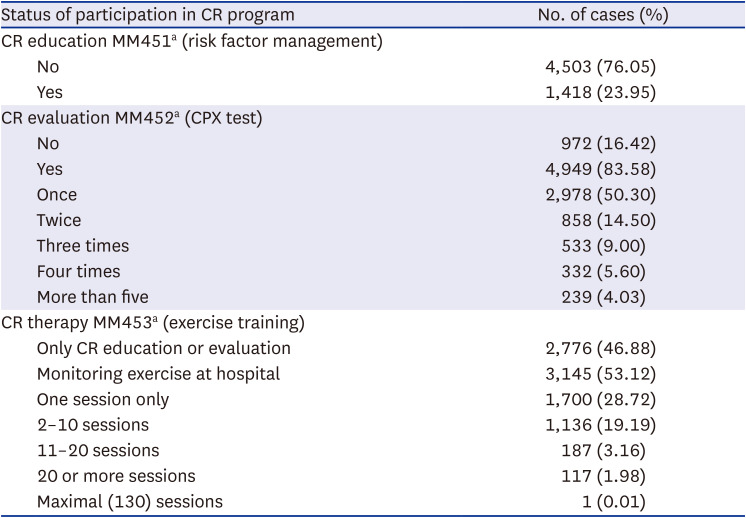
Table 4
The quality of CR participation among CR attendees in the original cohort (n = 5,921)
![]()
Prognostic impact of CR on cardiovascular outcomes after ACS
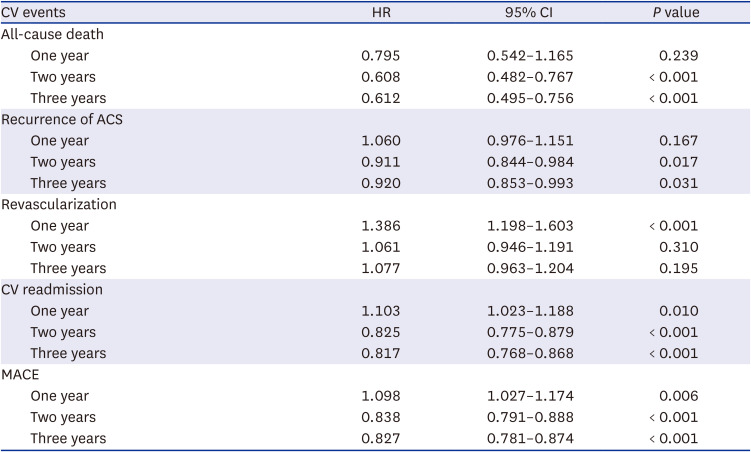
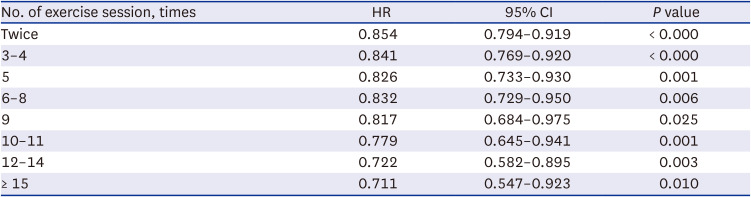
The 1:1 matching of 5,843 CR and non-CR patients showed that 143 (2.45%) and 223 (3.82%) patients died during the follow-up period, respectively. Table 5 shows that cardiovascular events including all-cause death, recurred ACS, cardiovascular readmission, and MACE were significantly lower in the CR group than in the non-CR group, after adjusting for potential confounders. Fig. 2 shows the Kaplan-Meier survival curves for cardiovascular events in both groups during the three-year follow-up period. The survival rates were 96.6% and 94.4% (log-rank P < 0.001), recurred ACS rates were 23.9% and 25.8% (log-rank P < 0.00289), cardiovascular readmission rates were 36.5% and 42.1% (log-rank P < 0.001), and MACE rates were 43.3% and 49.8% (log-rank P < 0.001) in the CR and non-CR groups, respectively. However, the revascularization rates were not different between the two groups (log-rank P < 0.2922). Table 6 shows the impact of CR on cardiovascular outcomes within three years after ACS in the propensity-score weighted study cohort. The cumulative 3-year HR for all-cause death was 0.612 (95% confidence interval [CI], 0.495–0.756), recurred ACS was 0.92 (95% CI, 0.853–0.993), CR readmission was 0.817 (95% CI, 0.768–0.868), and MACE was 0.827 (95% CI, 0.781–0.874) in the CR group. According to the subgroup analysis, CR was associated with a significant dose-response effect on the cumulative incidence of MACE, with a reduction in MACE incidence from 0.854 to 0.711 (Fig. 3, Table 7).

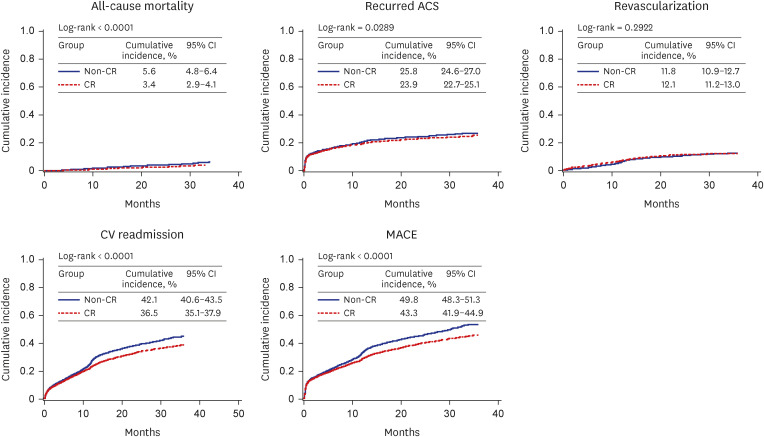 | Fig. 2Kaplan-Meier survival curves of CV outcomes.ACS = acute coronary syndrome, CR = cardiac rehabilitation, CV = cardiovascular, MACE = major adverse cardiovascular events, CI = confidence interval.
|
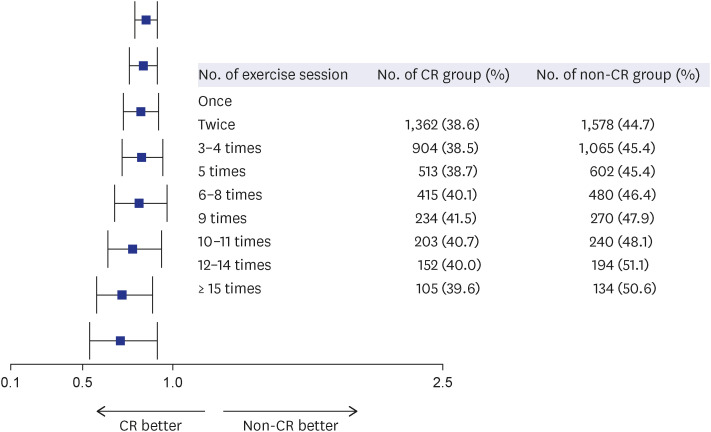 | Fig. 3Dose-response impact of CR on three-year cumulative MACE.CR = cardiac rehabilitation, MACE = major adverse cardiovascular events.
|
Table 5
Comparison of three-year CV outcomes between the CR and non-CR groups
CV = cardiovascular, CR = cardiac rehabilitation, ACS = acute coronary syndrome, MACE = major adverse cardiovascular event, PY = person-year.
![]()
Table 6
The impact of CR on CV outcomes in propensity-score weighted cohort
CR = cardiac rehabilitation, CV = cardiovascular, HR = hazard ratio, CI = confidence interval, ACS = acute coronary syndrome, MACE = major adverse cardiovascular events.
![]()
Table 7
Dose-response impact of CR on three-year cumulative MACE
CR = cardiac rehabilitation, HR = hazard ratio, CI = confidence interval, MACE = major adverse cardiovascular events.
![]()
Go to :
DISCUSSION
Clinical practice guidelines for CR have been officially published by many countries, including the United Kingdom, European Union, Canada, United States of America, Japan, and Korea.5141516171819 However, in spite of the high level of evidence and the strong recommendation for CR, the overall rate of CR participation is only about 30% to 40% globally.20 According to our study, the actual rate of CR participation in South Korea was only 5.8%. A previous study using KNHIS data reported a much lower rate of only 1.5%7 probably due to different study selection criteria, as we included patients with not only AMI but also those with UA and who underwent bypass surgery. We also included both inpatient and outpatient CR participation and more recent KNHIS data, which may imply that the CR participation rate had increased with time. In South Korea, CR insurance benefits were introduced in February 2017, and CR facilities have increased by up to 46 centers.8 Nevertheless, the rate of CR participation in South Korea remains much lower than that in high-income Western countries.2122 Therefore, efforts should be made to increase CR participation, including the establishment of new CR facilities in line with the increasing incidence of ACS.723 and active application of efficient strategies to resolve barriers to CR.62425 To achieve this goal, medical professionals’ efforts to improve CR environments and government-initiated strategies to improve CR policy are necessary.
Our study showed that patients in the CR group were more likely to be male, of middle age, health insurance subscribers, treated at tertiary hospitals, urban residents, and have less comorbidity than those in the non-CR group. Sex and age differences are well known issues related to CR participation; therefore, continuous efforts to solve these barriers are needed by providing women and older people a friendly CR environment through educational programs and nationwide campaigns, involving collaboration between hospitals, academic medical societies, and government programs. Paradoxically, medical aid beneficiaries were less likely to attend CR than were health insurance subscribers. According to the KNHIS policy, health insurance subscribers pay 50% of CR fee as allotted charges, but 2nd grade beneficiaries pay 15% and 1st grade beneficiaries pay 5%.9 Since most medical aid beneficiaries are in the low-income group, they may lack the time and resources to attend CR programs. Therefore, more special advantages or incentives, such as no allotted charges for CR fees, provision of transportation costs, and maintenance grants or special support grants for this group during the period of CR should be considered. There were regional gaps in the CR practice rate when considering the number of annual ACS cases and that most CR facilities are located in the metropolitan area or big cities of South Korea.8 Therefore, it may be too inconvenient for rural residents (i.e., those from farming/fishing villages, mountainous villages, and islands) to attend a CR program. Therefore, equal distribution of CR facilities and the establishment of CR programs at both tertiary and CVD-specialized general hospitals are also needed.
In addition to the low rate of CR participation, the quality of participation among CR attendees was subpar. While CR evaluations frequently included a CPX test (in 83.58% of the CR group), follow-up CPX tests were not frequently performed; less than half of the CR patients participated in ECG monitoring exercise sessions and only 1.98% (117 patients) completed 20 or more sessions. Moreover, 46.88% of CR attendees received only CR evaluation or education without exercise training at the hospital, mostly due to socio-economic barriers, indicating that active application of a well-organized home-based CR program is needed and that the medical cost for such a program should be reimbursed by the national healthcare systems. We considered patients with claim code MM451 as those who received CR education; therefore, 76.05% (4,503 patients) of the CR attendees were considered to have not received CR education. However, many hospitals may not have processed the claim code MM451 during the time of our study; therefore, this may be a transient phenomenon.8
Our study on original claims data of this KNHIS cohort demonstrated that the impact of CR on cardiovascular outcomes was superior to that of usual care after ACS, with follow-up death rates of 2.45% and 3.82% in the matched CR and non-CR groups, respectively. In spite of the short follow-up period, the incidence of all-cause death, recurred ACS, cardiovascular readmission, and MACE were significantly lower in the CR group than in the non-CR group, after adjusting for potential confounders. Interestingly, there was a significant dose-response effect of CR on the cumulative incidence of MACE with MACE incidence reduction from 0.854 to 0.711. Hammill et al.26 also reported a strong dose-response relationship between the number of CR sessions and long-term outcomes. If the rate and quality of CR participation are improved close to the expected goal, the impact of CR on cardiovascular outcomes may be magnified.
This study has several limitations that should be noted. First, the present study retrospectively reviewed medical records of patients with data linked to national health insurance claims; therefore, the results may have been biased due to various unmeasured confounding factors. Insufficient information on prognostic factors may have influenced the effects of CR, such as the size and location of myocardial infarcts, severity of coronary artery stenosis, time duration of myocardial ischemia, whether PCI was successful, and the presence of heart failure. In addition, the CR group may have shown better adherence to prognostic management than the non-CR group. Furthermore, economic ability, family interest and support, and particularly the patient’s baseline functional status would have influenced clinical outcomes. Second, the diagnosis of ACS was operationally defined using medical claims records, and there are possibilities of false exclusion or inclusion. Third, there could be a mismatch between actual performance and the claims record. As mentioned before, our period of index admission was the transient period of insurance benefit for CR, and incomplete claims for CR, especially CR education, may exist. Fourth, due to the limitation of health insurance claims data, the cause of death was especially difficult to identify. Therefore, cardiovascular mortality could not be distinguished. Nevertheless, this study’s finding is consistent with previous related studies, which showed that CR participation has a favorable effect on cardiovascular and all-cause mortality. Fifth, the follow-up period was relatively short (three years) because the claim codes of KNHIS for CR have only been collected since 2017. Therefore, further study is required with various kinds of CR cases for longer follow-up periods using NHIS claim data. Finally, we excluded the claim code AZ110 for CR education analysis, which is also used for CVD education in tertiary hospitals. We analyzed the three new claim codes created when CR insurance benefits were introduced; therefore, CR education may be underestimated since we could not analyze the claim code AZ110 together.
Despite these limitations, this nationwide population-based study is the first report to demonstrate the actual rate and quality of CR participation and the real impact of CR on cardiovascular outcomes. As previously mentioned, CR has only been covered by insurance provided by the Korean government since 2017; therefore, we need more time to establish a national systematic plan for improving CR implementation and a state-controlled CR network. CR participation should be increased through the establishment of new CR facilities and active application of efficient strategies to resolve barriers to CR. In addition, patient-oriented CR programs, such as a patient-preferred home-based CR strategy, should be applied to increase the rate of outpatient CR adherence. However, effective governmental policy and financial support are necessary for these strategies to be realized. Finally, we believe that these study results would be beneficial for use in countries where the status of CR participation is similar to that in South Korea or where CR is yet to be implemented.
In conclusion, the actual rate of hospital-based CR participation after ACS was only 5.8% in South Korea, despite coverage by the NHIS. In addition to low rate of CR participation, the quality of participation among CR attendees was subpar. Nevertheless, the original claims data of the KNHIS cohort revealed that the impact of CR on cardiovascular outcomes was superior to that of usual care after ACS. In spite of the short follow-up period, the incidence of all-cause death was significantly lower in the CR group than in the non-CR group, and CR was associated with a significant dose-response effect on the cumulative incidence of MACE.
Go to :
 XML Download
XML Download