

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Escherichia coli is a normal gut flora in humans, but occasionally, some E. coli strains can cause intestinal infections. Intestinal pathogenic E. coli is classified into five types according to clinical characteristic features: enterotoxigenic E. coli, enteropathogenic E. coli, enteroinvasive E. coli, enteroaggregative E. coli, and enterohemorrhagic E. coli (EHEC).1 Of these, EHEC is known to secrete Shiga toxin and cause serious problems, such as hemolytic uremic syndrome (HUS).
EHEC infection is estimated to occur in more than 1 million cases every year worldwide since the first report in 1982.23 EHEC infection is continuously reported in the United States and Europe.45 In Asia, EHEC infection is found mainly in Japan, which has reported 3,000 to 4,000 cases every year since 2010.6 Furthermore, severe complications of infection caused by EHEC are a major concern in global public health.7 In particular, HUS, which appears in approximately 5% of patients infected with the E. coli O157:H7 strain, may cause permanent renal sequelae.8 EHEC infection appears to be predominant in children so far because they are vulnerable to infection from their low level of immunity.89 Patients under 9 years of age accounted for over 50% of EHEC infection cases.210
In South Korea, approximately 2000 cases of EHEC infection have been reported since the designation of EHEC infection as a notifiable disease in 2000, with a yearly average of 90 cases. During that period, most cases occurred sporadically, and only a few small-scale outbreaks of EHEC infection occurred. There was an outbreak in 2011 where 9 people were infected with EHEC but were asymptomatic. Epidemiologic investigation revealed that the outbreak was associated with groundwater contaminated by feces from barns. Serotypes confirmed in the outbreak were O91, O82, and O15.11
From 2015 to 2019, there were 5 outbreaks, with an average of 3.8 cases per outbreak.12 Of these, 3 outbreaks were related to restaurants and 2 outbreaks occurred at home. Serotypes associated 5 outbreaks were O165, O168, and O26, and there was no case associated with O157 among them.12
In June 2020, the largest outbreak of EHEC infection involved 103 pediatric patients at a preschool A in Gyeonggi-do. In this study, we explain the epidemiological and clinical characteristics of the largest EHEC outbreak in South Korea. Our efforts with large-scale EHEC outbreak mentioned in this study will provide an example for future studies and a lesson to prevent other EHEC outbreaks.
In addition, we would like to describe the epidemiological investigations we conducted in response to the outbreak. Epidemiological investigations have already made significant contributions to tackling health challenges in resource-limited contexts through COVID-19 era and are also crucial for responding to new infectious disease such as monkeypox.1314 Contact isolation and quarantine measures used in our in-depth epidemiological investigation will greatly help to prevent the spread of EHEC outbreaks in the future.
Go to : 
METHODS
Outbreak detection and case definition
On June 15–16, 2020, 4 children attending preschool A, which had 184 children and 19 workers, visited a hospital in Gyeonggi-do with complaints of diarrhea and bloody stool. As group food poisoning was suspected, the cases were notified to the Public Health Center. The positive stool PCR test for EHEC in these 4 pediatric patients led to the identification of an EHEC outbreak and an epidemiological investigation by the Korea Disease Control and Prevention Agency (KDCA).
A laboratory-confirmed case of EHEC infection was defined as the isolation of E. coli harboring virulent genes (stx1 and stx2) in fecal specimens. If E. coli with stx1 or stx2 from fecal specimens was not isolated despite the presence of symptoms relevant to EHEC infection, the case was classified as a suspected case. The total cases are a combination of laboratory-confirmed cases and suspected cases. A retrospective cohort study was developed to identify the association between infection and exposure to presumed causative agents.
Epidemiological investigation
All 184 children and 19 workers at preschool A were included in the epidemiological investigation. They were requested to complete a standard questionnaire to assess clinical symptoms, prior food intake, attendance, and special activity history. For children, the survey was conducted through their teachers. To increase the reliability of the survey results, the teachers confirmed the children’s intake history and answered the questionnaire using a CCTV footage of preschool A that was recorded before the investigation.
For those who met the case definition, their travel history and symptoms of their household members were checked to determine whether the outbreak was associated with infection reported in other regions and was attributed to infection outside preschool A.
Laboratory investigations
Rectal swabs were conducted and samples were collected from 184 children, 19 workers, and 141 family members who had related symptoms or wanted to be tested. The specimens from the 184 preschool children were tested at the Gyeonggi-do Institute of Health and Environment. Tests for patients who were already hospitalized before sample collection were conducted at the hospital.
During the first field epidemiological investigation on June 16, cooking utensils, drinking water, and preserved food were collected from the preschool and tested. Then, on June 19, environmental samples were collected from classrooms and toilets, and tests were conducted. Additionally, inspections were conducted at companies that delivered meat to the preschool. Since the children played with soil on June 10 and 11, dates on which they were highly likely to be exposed to the source of infection, specimens from the dirt outside the preschool were collected and tested.
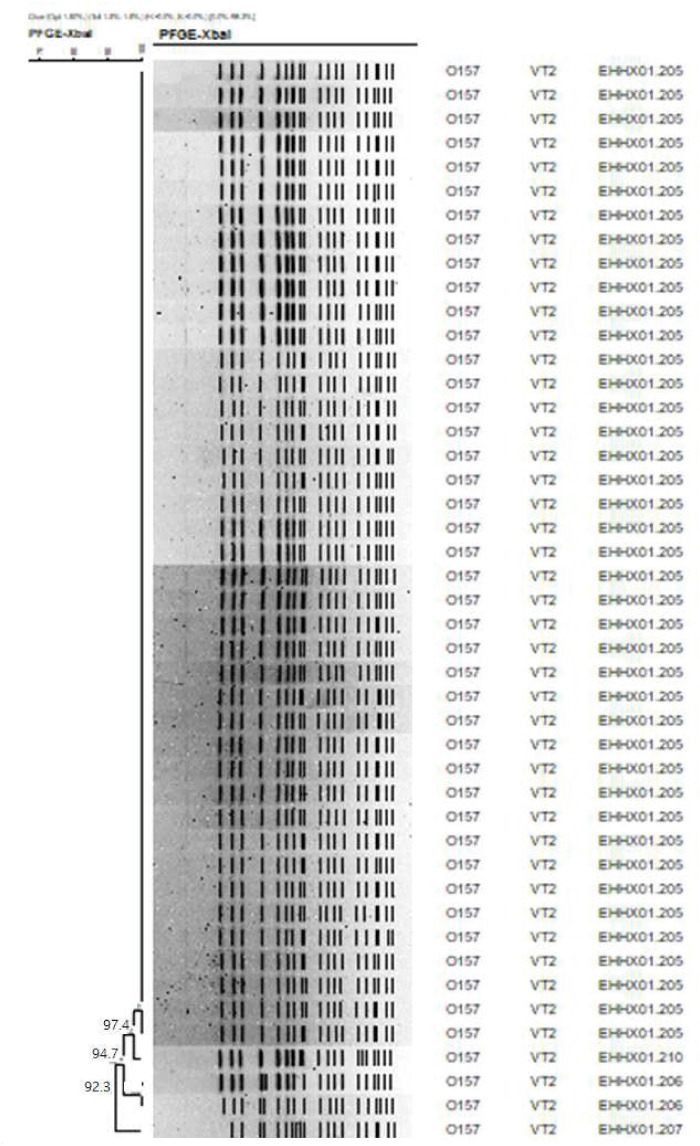
Pulsed-field gel electrophoresis (PFGE) was performed using a standardized protocol (www.pulsenetinternational.org). Plug-embedded genomic DNA of each isolate was treated with an XbaI restriction enzyme and then separated to a CHEF Mapper system (Bio-Rad, Hercules, CA, USA) with switch times of 2.16 seconds and 54.17 seconds at 6 V/cm for 18 hours. Genetic similarity among strains was analyzed using DICE (optimization of 1.5%) and UPGMA (tolerance of 1.5%) generated by BioNumerics software ver. 7.5 (Applied Math, Austin, TX, USA).
Statistical analysis
For general and clinical characteristics, descriptive statistics were presented as numbers with percentages for categorical variables. The relative risk of EHEC infection was calculated with a 95% Wald confidence interval (CI) for each food. When there was no infection in the non-intake group for a food, the number of infections was added to 0.5 for both the intake and non-intake groups. Foods with a lower 95% confidence limit greater than 0 were considered a risk factor for EHEC infection. All analyses were performed using R software (version 4.1.2; www.r-project.org; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Yonsei University College of Medicine, Yongin Severance Hospital (approval No. 9-2022-0043). As this outbreak investigation was part of an urgent response to a public health emergency conducted in accordance with the Korean Infectious Disease Control and Prevention Act No.4 and Enforcement Rule of Bioethics and Safety Act No.33., informed consent was waived by the IRB.
Go to :
RESULTS
Outbreak description
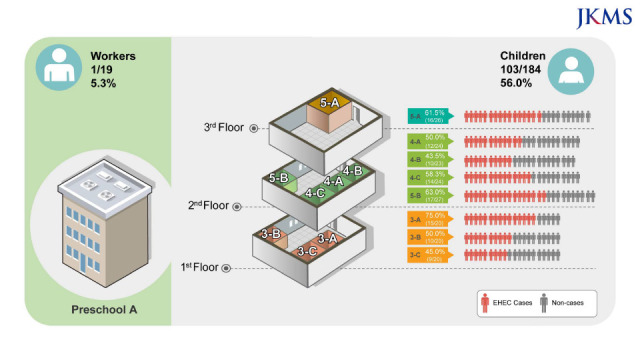
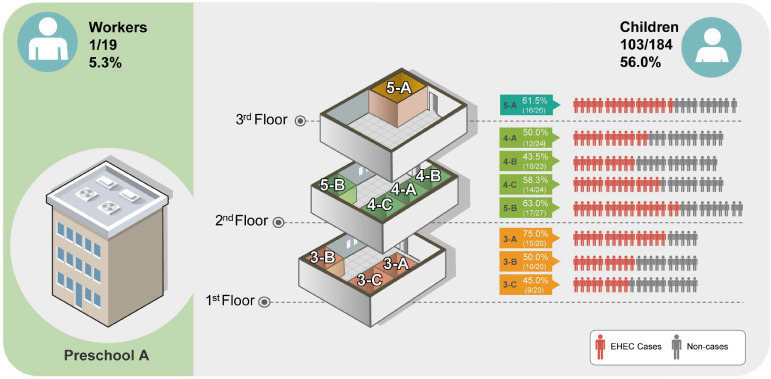
All children and workers in preschool A completed the interview for the epidemiological investigation. A total of 104 persons (70 laboratory-confirmed cases and 34 suspected cases) were involved in the outbreak, and the overall attack rate was 51.2%. There were 103 affected children out of 184 (56.0%), whereas only 1 worker was identified among the 19 workers (5.3%). The three-story preschool A had 8 classrooms, and the attack rates did not differ significantly among classes (Fig. 1).
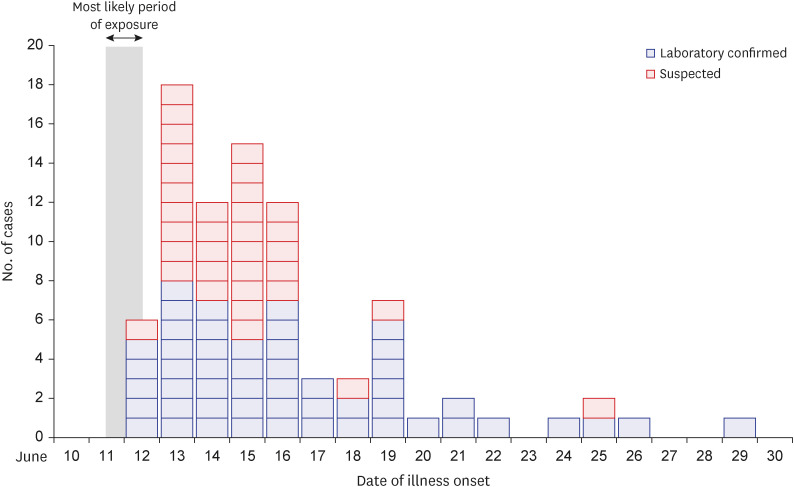
The epidemic curve was plotted based on the date of symptom onset of the 85 symptomatic cases, which consisted of 51 laboratory-confirmed cases and 34 suspected cases (Fig. 2). Ever since the first 6 cases were reported on June 12, more cases were continuously identified by June 29. Fifty-seven cases (67%) yielded a peak curve from June 13 to 16. The attendance date of confirmed cases was reviewed to narrow down the estimated date of exposure. Child A did not attend preschool for 10 days and had no contact with other children of the preschool. However, after attending school from June 11 to 12, the child showed symptoms on June 13 and was confirmed to have EHEC, which has a genetic link to the pathogen of the outbreak. This fact served as an essential clue to specify the suspected exposure dates to June 11–12. Five cases between June 24 and 29, which occurred after the maximal incubation period of EHEC of 10 days, mean that a secondary attack occurred in this outbreak.
Clinical characteristics of the cases are demonstrated in Table 1. Girls accounted for 52.4% (54/103) and the mean age was 3.99 years (range 3–5 years). Of the 103 children, 85 (82.5%) had symptoms, but 18 (17.5%) remained asymptomatic during the investigation. The most common symptom was diarrhea (75.7%), followed by abdominal pain (57.3%). When we followed up the clinical course of these 103 children, 32 (31.1%) were admitted to the hospital, of which 81.5% had a bloody stool, which was more frequently observed in admitted children than in non-hospitalized children. Fifteen (14.6%) experienced HUS and 4 (3.9%) received dialysis treatment. All patients were discharged (mean duration of hospitalization, 11.6 ± 6.1 days) and there were no deaths. No patient required permanent dialysis.
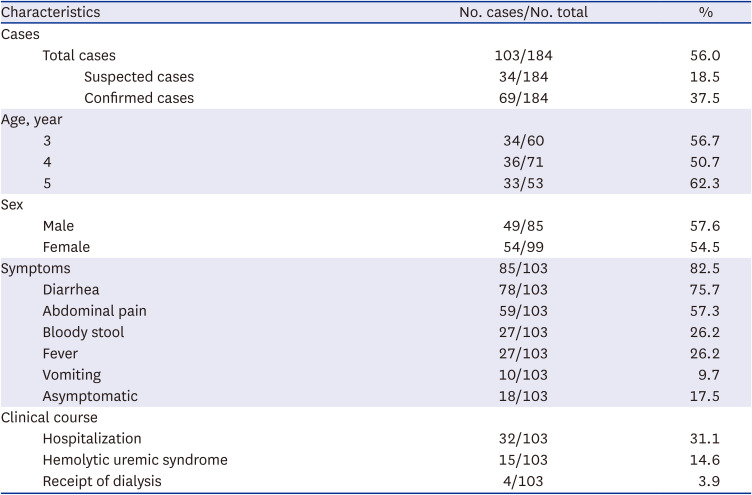
Table 1
Characteristics of enterohemorrhagic Escherichia coli O157:H7 outbreak among children in preschool A
![]()
Microbiological investigations
EHEC was isolated in 70 of 103 persons. PFGE analysis of the 45 available samples from confirmed cases revealed that all isolates were classified as O157:H7. Four genotypes with high genetic relevance (92.3%) were identified: EHHX01.205 type, 41 cases; EHHX01.206 type, 2 cases; EHHX01.207 type, 1 case; and EHHX01.211 type, 1 case (Fig. 3). This means that all the confirmed O157:H7 cases were highly likely to have a single source of infection.
Epidemiological investigations
No relevant microorganisms were identified in samples collected from the foods and the environment. All preschools with catering facilities are required by law to store food for 144 hours, hence called as “preserved food.” We attempted to collect the preserved food to identify the cause of the infection. However, most foods served to children were not stored until the investigation. Despite trying to trace the food ingredients, we found it difficult to find any causative clues of infection. Furthermore, the environment had been disinfected before the investigation began. The investigation on the spot of outdoor activity including soil, no relevant microorganisms were also isolated.
Refrigerator inspection revealed that the temperature in the food refrigerator compartment was consistently above 10°C even when the door was not opened for more than 8 hours, which means that the refrigeration function was not maintained well for this compartment.
Analysis of the children’s food intake history revealed that ingestion of paprika and apple served on June 11–12 was associated with EHEC infection (Table 2). In analyses, paprika served on June 11 and apple served on June 12 had relative risks of 9.80 (95% CI, 1.46–65.91) and 6.85 (95% CI, 1.04–44.92), respectively.
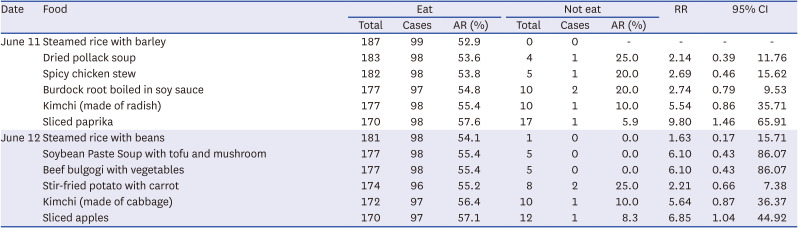
Table 2
Food-specific attack rates and relative risks among cases who attended preschool A
![]()
Intervention
After recognizing the outbreak on June 16, active surveillance and disinfection were continued. At first, it was recommended to stay at home to prevent secondary transmission due to person-to-person contact. However, as children in urgent need of daycare continued to attend despite the recommendation, additional infections occurred continuously, and the preschool was forced to close by law enforcement on June 19.
Go to :
DISCUSSION
An outbreak of EHEC infection requires an immediate response because it can cause serious consequences such as HUS. Therefore, it is important to evaluate the epidemiological and clinical characteristics of an EHEC infection outbreak. In this study, we described the largest outbreak of EHEC infection that occurred in a preschool in South Korea. A total of 104 patients were involved in this outbreak, almost all of whom were children. A considerable proportion of affected children experienced HUS and received dialysis treatment. Despite the prompt response by the KDCA, including isolation of patients, management of contacts, and disinfection of the environment, patients with EHEC infection continued to be identified. Finally, the outbreak was terminated after the preschool was closed to prevent ongoing transmission. Our experience from the response to the largest outbreak will help prepare countermeasures against an EHEC infection outbreak in the future.
In the past 10 years, a total of 438 cases of EHEC infection have occurred in South Korea. Among them, children under the age of 10 years account for 51.7%, and it has been confirmed that EHEC infection mainly occurs in children.15 Several reports also confirmed frequent occurrences in children under the age of 5.161718 This may be related to more than just outbreaks in preschools and elementary schools10; it is presumed that children are more susceptible to infection because of their lower immunity than adults.89 In addition, person-to-person transmission is known to be more common among infants and toddlers attending preschool1619 because exposure occurs easily through diapers with feces contaminated with pathogens.20 When exposed to an infectious agent, the clinical course is monitored during the incubation period, and if there are symptoms, a stool culture test is performed. However, in infants and young children, who cannot express their symptoms well, diagnosis and examination are delayed, which can spread the infection in preschools. In this outbreak, 5 cases (June 24–29) that occurred beyond the maximum incubation period were considered secondary transmission of EHEC from children exposed to the contaminated food. Therefore, to prevent the occurrence and spread of an outbreak of EHEC infection in preschools with infants and children, it is necessary to thoroughly manage not only the infected but also the exposed people through hand washing, contact restrictions, attendance restrictions, and so on.
The O antigen, one of the structural regions of lipopolysaccharide in the outer membrane of EHEC, is an important cellular component for classifying strains for epidemiology and taxonomy; to date, more than 180 O antigens have been identified.21 In South Korea, there were 68 types of O antigens analyzed from 438 EHEC strains isolated from 2010 to 2019, with O157 accounting for the largest proportion (17.1%).15 The proportion of O157 is decreasing because of the non-O157 serotype, which is increasing owing to the recent development of inspection technology. However, it is a serotype that still accounts for a large proportion—39% (2017) in the US4 and 26.6% (2019) in Europe.22 Similar to the global trend, while the isolation rate of non-O157 serotypes O103 and O26 in South Korea has increased, the isolation rate of O157 is no longer the highest.15 However, O157 surged because of this large-scale epidemic and is still the main serotype of the EHEC epidemic. Therefore, continuous surveillance of the serotype trend of EHEC to identify the causative pathogens and to analyze various prevalence patterns of pathogens is essential to provide information necessary for infection prevention and management.
The epidemic curve of this outbreak showed a unimodal curve with peak occurrence on June 13. This type of curve suggests that this outbreak may be caused by simultaneous exposure to an infection source.23 In general, ingestion of food contaminated by E. coli is the major route of entry for EHEC infections.7 In our outbreak, the meals provided in the preschool are also considered the main cause of EHEC infection based on the epidemiological investigation. Among the meals provided on the suspected exposure dates (June 11–12), a paprika stick on June 11 and a sliced apple on June 12 had an increased relative risk for source of infection. Although EHEC infection is often associated with beef that is not cooked properly, vegetables have been reported as the cause of EHEC infections in a number of recent cases.1924 Vegetables could be contaminated with feces of cattle or cross-infected by meat during storage or food processing.
E. coli grows between 7°C and 50°C with the optimum temperature at 37°C, and it can survive for a considerable period when stored refrigerated or frozen.25 Owing to these microbiologic characteristics, EHEC infection occurs mainly in the summer, from June to September. In our outbreak, the investigation revealed that the refrigerator, in which the food (paprika stick and apple) suspected to be the infectious source was stored, did not cool below 10°C. Food ingredients stored in the refrigerator were exposed to temperatures conducive to bacterial growth, especially during the daytime when the refrigerator door is frequently opened. Moreover, it is possible that bacterial growth accelerated because the food materials had been exposed to room temperature in June several times before being transferred to the storage refrigerator after delivery.
Our study has several limitations. First, the preschool did not sufficiently cooperate with the epidemiological investigations, which prevented identification of the causative pathogen. Although the food service group had an obligation to store preserved food, this was done improperly. Moreover, disinfection was performed several times before the first epidemiological investigation, hence the environmental specimen was not expected to provide meaningful results. Second, recall bias may occur during surveys. However, through the CCTV footage, a high-risk diet was thoroughly reviewed, and the dates and foods that were estimated to be sources of exposure could be confirmed.
In conclusion, the findings of this study indicate the difficulty in terminating an EHEC outbreak among children at child care center. Therefore, we suggest that a prompt and aggressive response based on thorough investigation is needed to mitigate an outbreak when it occurs.
Go to :
 XML Download
XML Download