

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neuroendocrine tumors (NETs), also called carcinoid tumors, were described and defined as epithelial neoplasms with predominant neuroendocrine differentiation, and they can arise in most organs of the human body.1 However, 70% to 90% of NETs occur in the gastrointestinal (GI) tract.23 Rectal NET is a rare tumor with a relatively good prognosis, representing 1.8% of malignant anorectal neoplasms.45 Rectal NET is asymptomatic in over 50% of patients. Generally, rectal NETs are found incidentally during endoscopic examination. Recent improvements in endoscopic diagnosis and treatment procedures has facilitated the diagnosis of rectal NETs at an early stage.46 The typical endoscopic examination of rectal NETs reveals smooth, round, elevations covered with yellow-discolored mucosa.7
Several parameters have been suggested as being useful for predicting the malignant nature of rectal NETs, including size, endoscopic features, histological growth pattern, muscularis propria invasion, and lympho-vascular invasion.78 Among these parameters, tumor size has been proposed as the most important and reliable guide to malignancy of rectal NETs.91011 According to a recent survey, metastasis is found in fewer than 3% of tumors that are ≤10 mm in diameter.12 The frequency increases to 80% for those that are >20 mm.513
Recent recommended therapeutic strategies for rectal NET suggest that endoscopic resection is appropriate for tumors that are ≤10 mm and confined to the submucosa, as they are judged to have low metastatic potential.14 Endoscopic mucosal resection (EMR) is the endoscopic treatment of choice for small rectal NETs. However, pathologically complete resection is not always easy using EMR because most rectal NETs are not limited to the mucosa, but rather, invade the submucosa. It is often necessary to perform additional treatments due to involvement of the resection margin (16% to 62%).13 Recently, various methods of endoscopic resection were introduced and studied, such as endoscopic submucosal dissection (ESD) and EMR using an elastic band (EMR-L). However, these treatments are still controversial because long-term outcomes for patients with ≤10 mm rectal NETs without metastasis are poorly described in the literature.1315
In this study, we compared the efficacy and feasibility of treatment between endoscopic resection using a pneumoband and an elastic band (ER-BL) and conventional EMR for rectal NETs smaller than 10 mm.
METHODS
1. Patients
From January 2004 to December 2011, rectal NETs were diagnosed histopathologically after endoscopic examination followed by ER-BL or conventional EMR at Gil Medical Center. Rectal NETs 10 mm or less in size on endoscopy without distant metastases on abdominal CT were indications for endoscopic resection. We retrospectively reviewed the medical records of all of these patients. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the ethics committee of Gachon University Gil Medical Center (Grant No. GCIRB 2870-2012).
2. Resection Methods
1) ER-BL
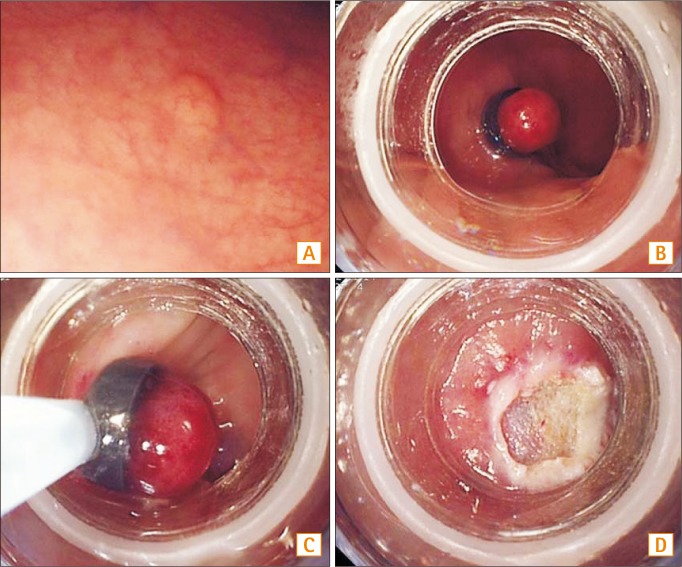
ER-BL and EMR-L were carried out with a single-channel scope (GIF-Q260 or H260, Olympus Medical Systems Co., Tokyo, Japan). Endoscopic resection using a pneumoband (ER-PB) was conducted as follows: after aspirating the lesion into the pneumoband cap with or without a submucosal injection of the solution (10% glycerin plus 5% fructose in 0.9% saline, a small amount of indigocarmine and epinephrine diluted to 1:1:100,000), the tumor was ligated with the pneumoband. A snare (SD-9U-1, Olympus Medical Systems Co.) was placed just below the pneumoband (MD-48709, Akita Sumitomo Bakelite Co., Ltd., Tokyo, Japan) and it was resected immediately using a high-frequency cutting current (Fig. 1).
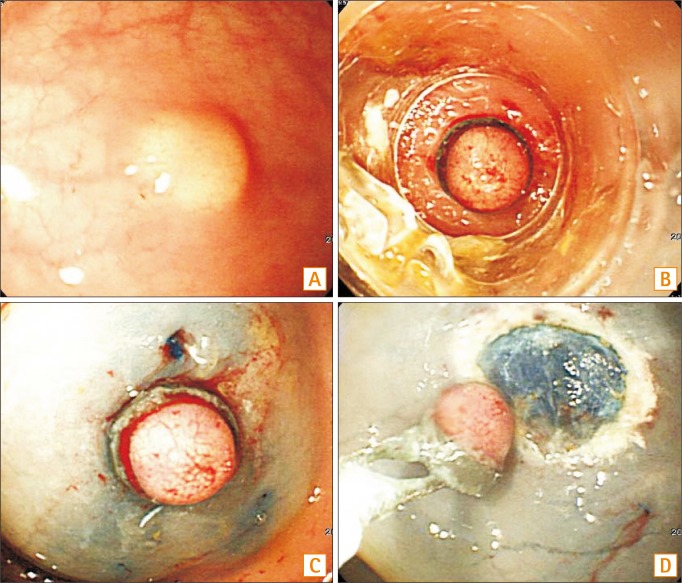
EMR-L was conducted as follows: the lesion was elevated by submucosal injection of the same solution described above for ER-PB. After aspirating the lesion, the tumor was ligated with an elastic band (Stiegmann-goff Clearvue Endoscopic Ligator, ConMed, NY, USA). The section below the band was resected by using a high-frequency cutting current with the snare placed below the band (Fig. 2).
2) Conventional EMR
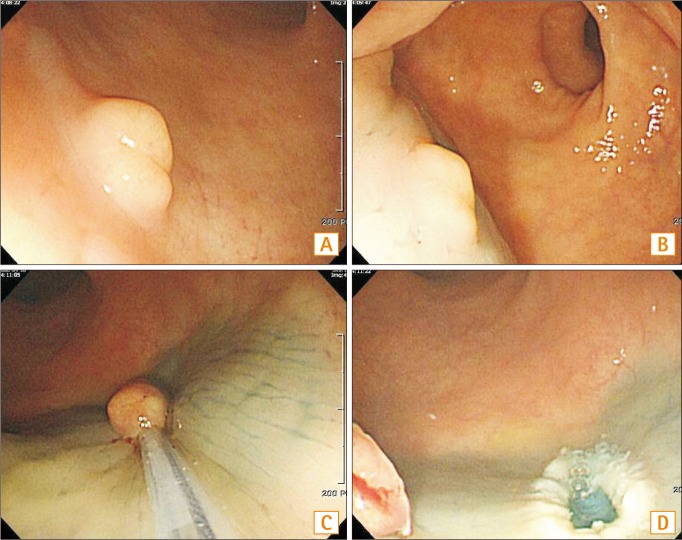
We used a single-channel scope (GIF-Q260 or H260, Olympus Medical Systems Co.). Conventional EMR was conducted as follows: the tumor was elevated by submucosal injection of the same solution described above for ER-PB. Then, the lesion was snared and resected using a high-frequency cutting current (Fig. 3).
3. Outcomes
The primary end-point of this study was the complete resection rate, including the lateral and deep resection margin in resected rectal NETs. Complete resection was defined as the existence of normal tissue in the mucosa or submucosa surrounding both the lateral and deep margins of the tumor without any tumor cells in the resection margin on microscopy. All histopathological appearances were thoroughly examined by a GI pathologist at our institution. The secondary end-point was complications such as bleeding or perforation.
4. Follow-up
To evaluate recurrences, periodic follow-up endoscopy and abdominal CT were performed for all of the patients. The first follow-up examination was performed 6 months after endoscopic resection with endoscopy and abdominal CT. After that, endoscopy and abdominal CT were performed annually.
5. Statistical Analysis
Student's t-test was applied to estimate and compare age, tumor size, and distance from the anal verge (AV) between groups. The chi-squared test was performed for analysis of sex, ratio of positive resection margin, and complications. Factors evaluated for complete resection by univariate analysis were sex, age, method, color, size, ulceration, and complications. Multivariate analysis including all predictors from the univariate analysis was assessed by multiple logistic regression analysis, and the OR with 95% CI was determined. A P-value <0.05 was considered significant. All analyses were conducted using SPSS software (SPSS II v.12; SPSS Inc., Chicago, IL, USA).
RESULTS
1. Demographic and Clinical Characteristics
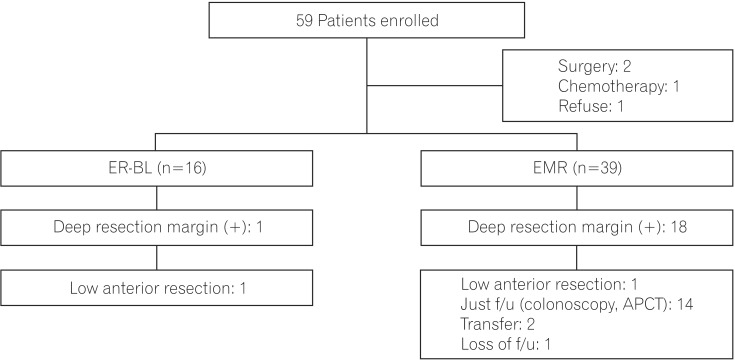
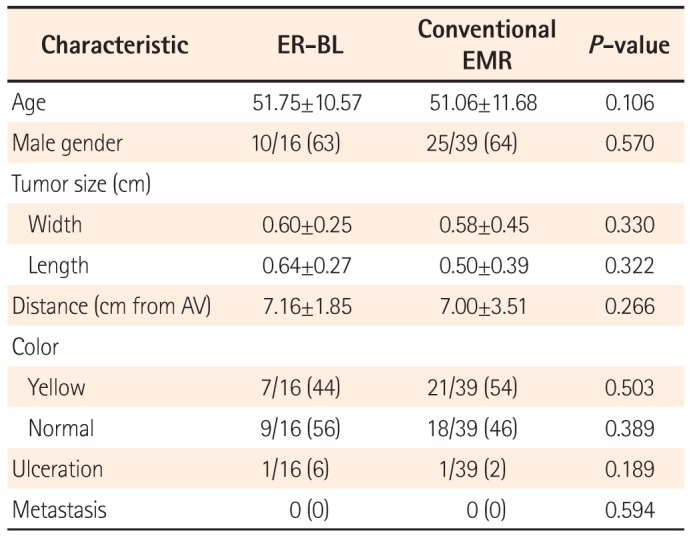
Over the 8 years from January 2004 to December 2011, 59 patients at Gil Medical Center were diagnosed with rectal NET. Among 59 patients, four patients received other treatments. Two patients underwent radical surgery involving a low anterior resection. As one patient's tumor had spread to the liver, she was referred for chemotherapy. Moreover, another patient refused treatment. Consequently, 55 patients received endoscopic resection for rectal NET. Sixteen patients underwent ER-BL. For comparison, 39 patients underwent conventional EMR. The demographic characteristics of the 55 enrolled patients are summarized in Table 1. All patients were asymptomatic and none had symptoms or signs of carcinoid syndrome. There was no significant difference in the age, sex, tumor size, distance from the AV, or tumor color between these two groups.
2. Endoscopic Ultrasonographic Findings
Among 59 patients, nine patients underwent EUS. Two patients who were confirmed to have submucosal invasion on the EUS underwent surgery. Seven patients were confirmed to have a hypoechoic lesion smaller than 1 cm in the submucosa without lymph node involvement.
3. Endoscopic Findings and Clinical Outcomes
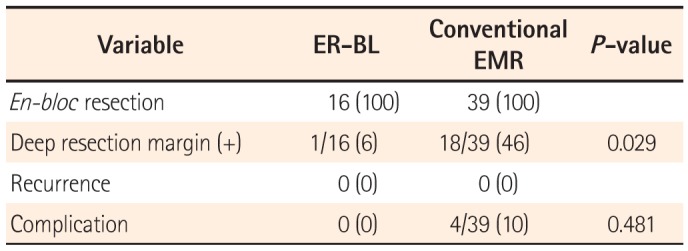
All the tumors were removed in an en bloc manner. Significantly, the rate of positive deep resection margins was one patient (6%) in the ER-BL group and 18 (46%) in the conventional EMR group (P =0.029) (Table 2). A patient with a positive deep resection margin in the ER-BL underwent low anterior resection. Eighteen patients with a positive deep resection margin on conventional EMR underwent the following additional treatments: low anterior resection (one patient); just follow-up with colonoscopy and abdominal CT (14 patients); transferred to other hospital (two patients); and loss of follow-up (one patient) (Fig. 4). The 55 patients who underwent endoscopic resection all received follow-up endoscopy and abdominal CT. To date, there have been no recurrences and no patients have received additional interventions.
4. Adverse Events
Four patients who underwent conventional EMR experienced complications. Three patients experienced delayed bleeding and were treated using argon plasma coagulation. One patient experienced perforation. We did hemoclipping immediately. Consequently, the patient recovered within a few days. On the other hand, patients who underwent ER-PB did not experience any complications (Table 2).
5. Factors Affecting the Success of Complete Resection
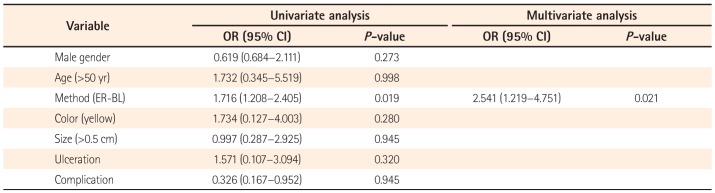
To investigate the independent factors affecting a successful complete resection, stepwise forward multiple logistic regression analysis was performed. Sex, age, method, color, size, ulceration or not, and complications were analyzed. Among these even factors, ER-PB remained significant in multivariate analysis (OR [95% CI], 2.541 [1.219–4.751], P=0.021) (Table 3).
DISCUSSION
With the development of endoscopy, GI NETs have been discovered at an early stage.1 In general, rectal NETs less than 10 mm in diameter and a depth of invasion limited to the submucosa can be curatively treated by endoscopic resection. 1617 Furthermore, rectal NETs of less than 10 mm in size, without metastases or muscle invasion, are reported to have a good prognosis, with an almost 100% 5-year survival rate.1819 There is no definite guideline about endoscopic resection for patients diagnosed with small sized rectal NETs without metastasis. We show here that novel ER-PB could be an effective endoscopic resection method for rectal NETs smaller than 10 mm.
NETs are characterized as slow-growing malignant neoplasms, being epithelial tumors composed of endocrine cells.20 GI NETs are frequently seen in the colorectal area, especially the rectum. One of the most common primary sites of GI NETs is the rectum within 10 cm of the anus.20 According to previous reports, risk factors for metastasis of rectal NET are: over 10 mm in diameter, muscular invasion, poorly differentiated neuroendocrine histology, and lympho-vascular invasion.5 However, rectal NETs estimated as <10 mm in diameter with no atypical histology and confined to the submucosa without lympho-vascular invasion almost never metastasize.2122
Due to recent advances in endoscopy technique, various methods of endoscopic resection were introduced and widely used. The representative methods are polypectomy and conventional EMR. Even though polypectomy and conventional EMR are quite simple, these techniques are sometimes associated with margin involvement and crush injury of the resected specimen, which leads to a need for an additional intervention.2324 To overcome these shortcomings, various modified methods of endoscopic resections have been described. Especially, ESD and EMR-L result in good outcomes for rectal NETs less than 10 mm.1325
ESD was originally developed to obtain one-piece resection for early gastric cancer.26 ESD is a superior method and has the advantage of permitting en bloc and histologically complete resection, compared with other endoscopic interventions. ESD can control the depth of submucosal dissection under endoscopic view. In this respect, it is clear that ESD is a useful therapeutic option for rectal NET.1627 However, ESD has the disadvantage of a long procedural time and a considerably high risk of perforation as well as demanding a high level of technical skill.2528
Theoretically, by adding a ligation process, EMR-L should be able to safely and completely resect the lesion and submucosal layer. Compared with conventional EMR and polypectomy, EMR-L can remove a deeper part of the submucosal layer.1315 Some studies show that EMR-L is as effective as ESD for treatment of rectal NETs less than 10 mm in diameter showing invasion up to the submucosa without complications such as bleeding or perforation.23 However, there are still certain cases that exhibit a positive resection margin, and it has a risk of bleeding and perforation greater than that of polypectomy and conventional EMR.1529
Pneumoband (PB), also called pneumo-active band, is commonly used in variceal bleeding.30 PB can be used in various endoscopic interventions. Recently, PB was attempted for treating non-variceal bleeding such as Malloy-Weiss syndrome and after perforation as a salvage technique after endoclip failure.31 ER-PB has many advantages when compared to other endoscopic interventions. First, ER-PB is technically easier to use than other methods, with the lesions well viewed under direct pressure and suction from the ligation cap.32 Second, other endoscopic devices such as a snare or a catheter for electrohemostasis can be used through the same channel when needed. Third, ER-PB might secure a clearer view due to the wider ligation cap. On the basis of these theories, in this study, we compared patients with rectal NET treated with different methods. Consequently, this study shows that ER-BL has a better outcome than conventional EMR in regards to deeper resection margins and complications. Moreover, multivariate analysis revealed that ER-BL was significantly associated with a successful complete resection.
However, there are some limitations to our study. First, our study is retrospective, non-randomized, and is a single-center study conducted on a small number of patients. Second, ESD is known to be an efficient method for en bloc resection of large colorectal tumors. therefore ESD tends to increase gradually for rectal NET. Thus, there was no definite indication for choosing between conventional EMR and ER-BL.
In conclusion, ER-BL is a very effective method of endoscopic resection with regards to deep margin resection and a low rate of complications for rectal NETs less than 10 mm in diameter without metastasis. However, a large-scale, randomized, prospective, multicenter clinical study is necessary to confirm the feasibility and usefulness of ER-BL.
 XML Download
XML Download