

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Serrated polyposis syndrome (SPS), previously known as hyperplastic polyposis, is a rare condition characterized by multiple serrated polyps (SPs) spread throughout the colon and rectum.123 Since SPS is a somewhat complex syndrome whose molecular basis is not yet clearly understood, the World Health Organization (WHO) developed consensus criteria for the clinical diagnosis of SPS.4 SPS is associated with an increased personal and familial risk of developing colorectal cancer (CRC) despite endoscopic surveillance.15678910 Boparai et al.6 reported that the cumulative CRC risk was 7% at 5 years in patients with SPS undergoing endoscopic surveillance. Edelstein et al.8 reported a high recurrence rate (68%) of sessile serrated adenomas/polyps (SSA/P) and/or adenomas as well as a significant risk of CRC. Therefore, close surveillance including an annual colonoscopy is recommended in patients with SPS.8111213
However, a considerable number of patients with symptoms suggestive of CRC including acute large bowel obstruction, diffuse abdominal pain or discomfort, weight loss, bowel habit changes, anemia, and rectal bleeding episodes were included in previous studies. These inclusions might have produced an overestimated CRC risk.212 Furthermore, most previous studies were performed in Western countries. There is very little data regarding SPS patients in Asian countries.14
In the present study, we investigated the clinical characteristics of SPS and evaluated the CRC risk by assessing the cumulative incidence of CRC in patients with SPS in Korea. We also identified the differences between Western and Korean patients with SPS.
METHODS
1. Patients
We retrospectively enrolled consecutive patients aged ≥18 years who fulfilled SPS WHO criterion 1 or 3 and were treated at Samsung Medical Center, Seoul, Korea, between March 1999 and May 2011.
Specific data including demographic factors such as age, sex, and personal history of CRC and other malignancies were obtained from the medical records. Colonoscopy reports with corresponding pathology reports during follow-up were collected to derive information regarding polyp size, number, location, morphology, and treatment method. Esophagogastroduodenoscopy (EGD) reports were ascertained to evaluate extracolonic cancer risks. A cumulative method was used to count the polyps; all that were diagnosed over the course of colonoscopies were counted. Interval CRC was defined as a CRC that developed under endoscopic surveillance after SPS diagnosis.
The follow-up period was measured from the date of the initial colonoscopy to that of the last surveillance colonoscopy. Patients were excluded if they had a known germline adenomatous polyposis coli mutation, Lynch syndrome, IBD, or total proctocolectomy.
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB number: 2011-12-077). Because this study conducted a retrospective data review, consent was not required or obtained. However, patient records and information were anonymized and de-identified prior to the analysis.
2. Definition
The WHO criteria were used to identify SPS. The criteria included: (1) at least 5 SPs proximal to the sigmoid colon, of which 2 measured at least 10 mm in diameter (WHO criterion 1); (2) any number of SPs occurring proximal to the sigmoid colon in an individual who has a first-degree relative with SPS (WHO criterion 2); and/or (3) ≥20 SPs spread throughout the colon (WHO criterion 3).4 In the present study, none of the patients were diagnosed with SPS based on the second criterion alone because familial histories are not always reliable in a retrospective study. Adherence to the described criteria was assessed by analyzing endoscopy reports and the corresponding pathology reports as well as pathology reports of colonic surgical resection specimens. All of the counted polyps were biopsy proven and tallied once. Polypectomy or endoscopic mucosal resection for the polyps was performed once they were ≥5 mm in diameter.141516
Polyps were classified as SP and conventional adenoma. SPs were subdivided as hyperplastic polyps (HPs) and serrated adenomas (SAs). The pathology reports showed SSA/P or traditional serrated adenoma (TSA). However, since the distinction between these polyps was not made throughout the early study period and they are both considered precursor lesions in the “serrated pathway,” the SA category comprised both lesion types.1617
The proximal colon was defined as the area proximal to the splenic flexure (transverse, ascending colon, and cecum), while the distal colon was defined as the descending colon and sigmoid colon.
RESULTS
1. Clinical Characteristics of SPS Patients
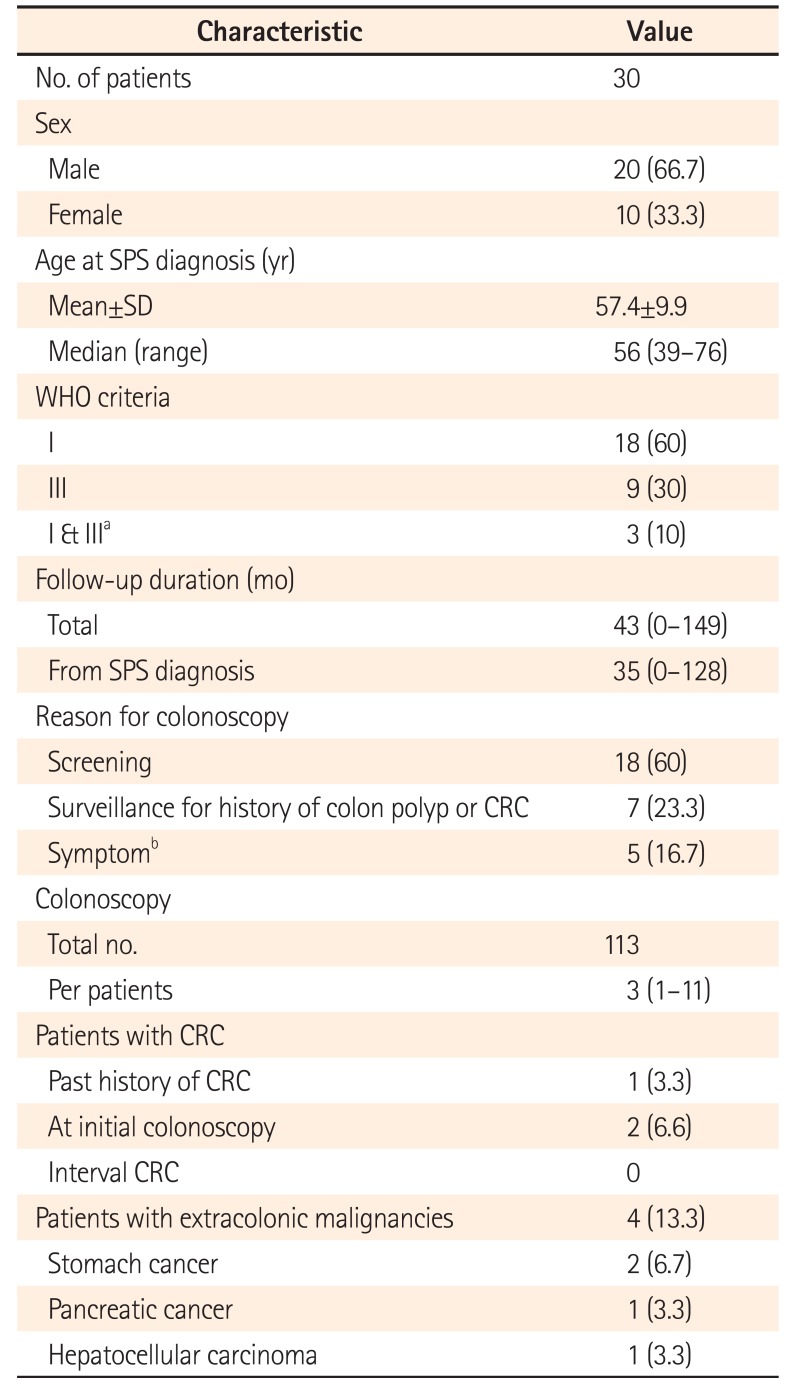
A total of 120,095 patients (69,369 men and 50,726 women) underwent a colonoscopy at the Samsung Medical Center between March 1999 and May 2011. Among them, 30 (0.025%) met the WHO criteria for SPS. Table 1 presents the clinical characteristics of the patients with SPS. The median age at diagnosis was 56 years (range, 39–76 years), and 20 (66.7%) patients were male. Twenty-one of 30 patients (70%) met WHO criterion 1 and 12 patients (40%) fulfilled WHO criterion 3. Three patients initially diagnosed with SPS by WHO criterion I then met criterion III during surveillance. In addition, 22 patients (73.3%) had synchronous adenomatous polyps.
The reasons for the initial colonoscopy were screening in 18 patients (60%), colon polyp history in 6 patients (20%), bloody stool and/or anemia in 2 patients (6.7%), bowel habit changes in 2 patients (6.7%), abdominal pain in 1 patient (3.3%), and history of CRC in 1 patient (3.3%). The median overall follow-up period was 43 months (range, 0–149 months) and the median follow-up period from the diagnosis of SPS was 35 months (range, 0–128 months). A total of 6 patients (20%) underwent only the initial colonoscopy. Among them, 2 patients could not undergo surveillance colonoscopy due to cancer progression (advanced gastric cancer in one, advanced rectal cancer in one). The other 4 patients (13.3%) were lost to follow-up after the initial colonoscopy. In the time period observed, 113 colonoscopies were performed for a median number of colonoscopies per patient of 3 (range, 1–11). Three of the 30 patients underwent colectomy. Two patients were diagnosed with CRC at the initial colonoscopy. The other patient underwent colectomy because the polyps were too numerous to remove endoscopically. However, there was no evidence of hereditary polyposis syndrome on genetic testing.
A total of 26 patients (86.7%) underwent EGD. One patient (3.8%) had numerable HPs, 2 (7.7%) had gastric adenoma, and 2 (7.7%) were diagnosed with stomach cancer. Another 2 patients (7.7%) had other extracolonic malignancies that included pancreatic cancer and hepatocellular carcinoma (one each).
2. Features of Polyps in SPS Patients
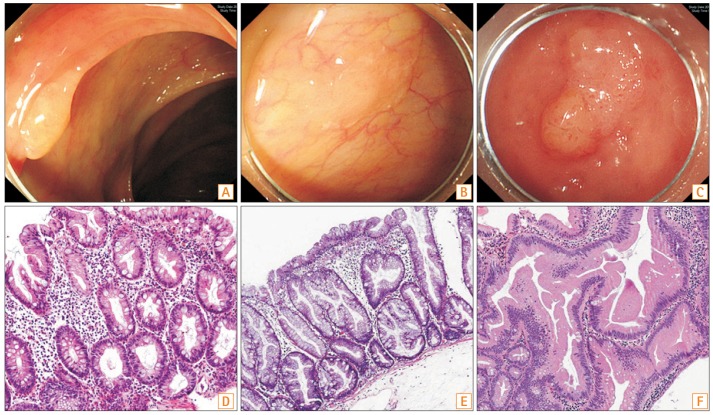
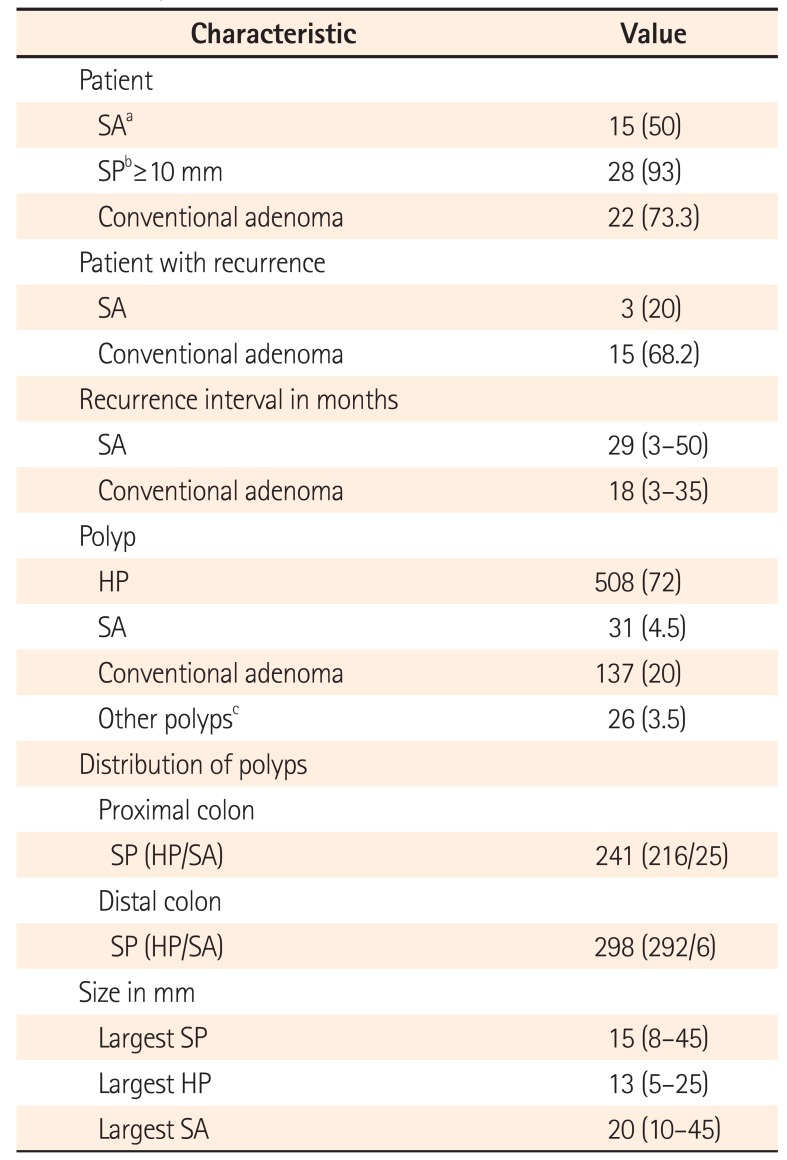
The characteristics of polyps in the patients with SPS are summarized in Table 2. A total of 702 polyps were detected: 508 (72%) HPs, 31 (4.5%) SAs, and 137 (19.5%) conventional adenomas (Fig. 1). Of the SPs, 241 (45%) were located in the proximal colon and 298 (55%) in the distal colon. However, SPs ≥10 mm in diameter were more found frequently in the proximal colon than in the distal colon. Similar to SPs ≥10 mm, the SAs were mainly distributed throughout the proximal colon (Fig. 2). The maximum size of the HPs and SAs were 25 mm and 45 mm, respectively; they were all located in the ascending colon. A total of 20% of patients (3/15) had recurrent SA, while 68% (15/22) had adenoma recurrence on surveillance colonoscopy. The median recurrence interval of SA and adenoma was 29 months (range, 3–50 months) and 18 months (range, 3–35 months), respectively. Additional polyps were discovered during surveillance colonoscopy in all patients (Table 3). During follow-up, the median cumulative number of polyps per person was 19 (range, 5–82), 14 HPs (range, 5–55), 0.5 SAs (range, 0–5), and 2 adenomas (range, 0–29).
3. Risk of CRC in SPS Patients
Of the 30 patients with SPS included in this study, 3 (10%) were diagnosed with CRC. One was already diagnosed with CRC before inclusion, while 2 were diagnosed at the initial colonoscopy. The first patient underwent colon resection for rectal cancer (papillary adenocarcinoma, T2, N0, M0) at 39 years of age, 1 year before being included in this study. He was diagnosed with SPS at the surveillance colonoscopy. He subsequently had an additional 14 HPs located in the proximal colon and measured 3 to 15 mm at surveillance colonoscopy. During follow-up, no cases of SA or advanced adenoma were detected.
Two other patients (6.6%) were diagnosed with CRC at the time of diagnosis of SPS on the initial colonoscopy. One patient was a 75-year-old woman who underwent colonoscopy because of bowel habit changes that included persistent diarrhea. At the initial colonoscopy, she was diagnosed with CRC in the hepatic flexure. She also had multiple SPs including 1 SA throughout the proximal colon that measured 3 to 25 mm. The largest polyp was proven as HP. She underwent a right hemicolectomy, and examination of the resected specimen revealed an adenocarcinoma microsatellite stable tumor (T1, N0, and M0). The other patient was a 61-year-old man who complained of recurrent bloody stool. On colonoscopy, a rectal mass was apparent and was diagnosed as adenocarcinoma, microsatellite stable tumor. He also had 22 SPs including 1 SA and 1 adenoma located in all segments of the colon that measured 2 to 20 mm. Multiple hepatic metastases were detected during the preoperative work-up, and he subsequently underwent palliative chemotherapy. However, he died of cancer progression within 1 year. All 3 patients were diagnosed with CRC; however, advanced immunohistochemistry testing such as that for the BRAF/KRAS mutation was not conducted at the time of diagnosis.
During the follow-up of patients with SPS, except for 2 with SPS-synchronous CRC and 1 with a history of CRC, no cases of CRC were detected on the surveillance colonoscopy.
DISCUSSION
To date, several studies and a case series have reported on SPS; however, they provided limited information on SPS because most were retrospective with small sample sizes. Scant data are available on the natural history of patients with SPS, and studies of Asian patients with SPS are nearly nonexistent. Here we evaluated the clinical characteristics and CRC risk of patients with SPS in Korea. Based on the present findings and data gleaned from the literature, we identified the differences between Western and Asian patients with SPS.
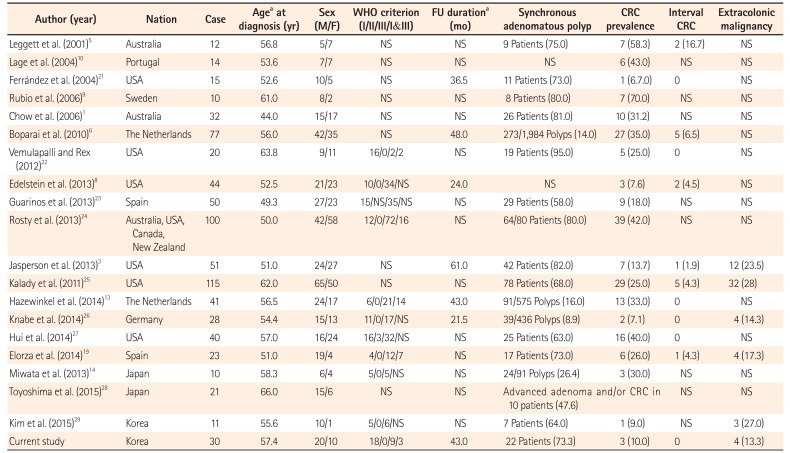
Table 4 summarizes the clinical characteristics of patients with SPS in recent studies reporting >10 cases of SPS. Only a few reports have addressed the prevalence of SPS. In Western studies, the prevalence of SPS was 0.08% to 0.66%.181920 One Korean study also reported the prevalence of SPS as 0.06%.29 In the present study, the prevalence was estimated as 0.025%. However, a recent Japanese study reported the prevalence of SPS as 8.4%,28 which was higher than those of the previous studies. The key difference is that all the enrolled patients underwent initial colonoscopy using a magnifying videoscope with chromoendoscopy in the Japanese study. HPs and SPs are difficult to detect by conventional imaging, and the study included patients who were previously treated for a colorectal neoplasm at another hospital. Therefore, the prevalence of SPS is higher than previously known. The age at SPS diagnosis in both Western countries and Asia tended to be in the 50s. However, in the West, the age at diagnosis was slightly younger than that in Asia. Additionally, there was no sex predominance in Western countries, while males predominated in Asian studies.
In the Western studies, the majority of patients met WHO criterion 3 on the basis of a large number of SPs throughout the colon.813232426 However, in the present study, the majority of patients who met WHO criterion 1 did not fulfill criterion 3. These findings correspond with those of a Japanese study and another Korean study in which half of the patients met WHO criterion 1. No patient underwent colectomy due to numerous polyps.1429
Different lifestyle and dietary factors of Asians may cause these phenotypic differences between Western and Asian patients with SPS.303132 However, the distribution of polyps was similar in the Western and Asian studies. The polyps were distributed evenly throughout the colon or predominantly in the distal colon, while large polyps (>10 mm) or SAs tended to be distributed in the proximal colon except in a few Western studies.
Above all, this syndrome increases the risk of CRC. However, scant data exist about the natural history of patients with SPS, while almost all studies were performed in Western countries (Table 4). In the present study, we investigated the natural history of SPS patients in Korea during a median 43 months (range, 0–149 months). The incidence of CRC in the present study was 10% (3/30). This rate was similar to that of another Korean study.29 In the Western studies, the incidence of CRC was 20% to 40% with the exception of a few small studies in which the incidence was much higher than those in the Korean studies.
There are several reasons for the difference in CRC incidence. First, the Western studies included more patients presenting with symptoms suggestive of CRC. For instance, in the study by Boparai et al.,6 CRC was found in 35% of the patients (27/77). Among them, 96% (76/77) had reasons for undergoing colonoscopy that included colorectal polyp history, family history of CRC, and clinical symptoms suggestive of CRC. Because of this selection bias, the estimation of CRC risk is likely to be inflated and reflect a CRC risk associated with symptomatic patients.283334 On the contrary, more than half of the patients (60%) in the present study underwent colonoscopy for screening purposes. Actually, some of the studies that included a majority of asymptomatic patients diagnosed with SPS by screening colonoscopy showed similar CRC incidences to our results (Edelstein et al.,8 7.6% [3/44]; Orlowska et al.,35 6.6% [1/16]).
Second, the ethnic differences may cause a discrepancy in CRC incidence between Western and Korean SPS patients. Western countries have shown a higher incidence of CRC than Asia countries in general populations.36 As mentioned above, fewer polyps were found in Asian patients with SPS than in Western patients.14 Few polyps may cause a low CRC incidence. There may also be genetic difference in patients with SPS. Kim et al.30 reported that SPs in Korean patients showed somewhat different molecular characteristics than those that occur in Americans.
Third, regardless of the discrepancy of CRC incidence between Western countries and Korea, the incidence of CRC in patients with SPS is higher than that in the general population. Accordingly, we must examine the prevalence of synchronous adenomatous polyps in patients with SPS, which was also higher than that in the general population.373839 Therefore, we do not know whether CRC in patients with SPS arose from the adenoma-carcinoma sequence or from the SA pathway. To date, there have been no reports of CRC origin in patients with SPS, so the CRC risk in patients with SPS may be exaggerated slightly.
The U.S. Multi-Society Task Force on Colorectal Cancer recommended annual colonoscopy surveillance in SPS patients. 11 This recommendation considered the high rate of interval cancer and rapid recurrence of colorectal polyps. A literature review34 reported that 5 of 27 patients (18.5%) with SPS but without CRC on initial colonoscopy developed CRC during follow-up. However, interval cancer can develop from missed polyps or incompletely resected polyps, although some may grow rapidly due to biologic behavior.40 Also, small polyps (<10 mm) can be easily missed during colonoscopy. 15 According to studies by Hazewinkel et al.13 and Knabe et al.,26 no CRC was found in SPS patients during annually surveillance colonoscopy after clearing colonoscopy. In addition, the number of newly detected polyps gradually decreased on sequential colonoscopies. These results support the notion that interval cancer mainly originates from missed polyps rather than from the rapid growth of polyps in patients with SPS. Therefore, careful colonoscopic examination is more important than frequent surveillance to prevent missed polyps and decrease the CRC risk.
There have been few reports about extracolonic malignancies in patients with SPS. Although previous studies reported various types of extracolonic malignancies, data supporting an association between SP and extracolonic tumor risk is lacking.319252629
In the present study, 26 patients (87%) underwent EGD and 5 (19.2%) had significant lesions including multiple HPs (n=1), adenoma (n=2), and stomach cancer (n=2). Although few studies have evaluated the upper gastrointestinal tract, this finding was inconsistent with those of previous Western studies, which described no significant lesions detected on EGD.3829 Another Korean study also reported that no patients had significant lesions detected by EGD. However, that study enrolled only 10 patients with SPS. Therefore, the present study suggests that Asian patients with SPS may require an evaluation of the upper gastrointestinal tract.
This is the largest retrospective study to date on Korean patients with SPS. We identified the phenotypic differences between Western and Asian patients with SPS based on similar phenotypic characteristics described in other Asian studies. The current surveillance guideline about SPS does not reflect phenotypic differences between Western and Asian patients since it was made on the basis of Western patients. Therefore, large and long-term follow-up cohort studies on Asian patients with SPS and a surveillance guideline for Asian patients are needed.
Our approach has some limitations. First, it was retrospective. The study population could not be investigated under the same condition due to its retrospective nature. As in other retrospective studies, selection bias can influence the data. Second, we grouped SSA and TSA into a single SA category since a large proportion of our data was derived from a period before a distinction was made between SSA and TSA. Third, this study included a relatively short follow-up period. Therefore, the risk of interval cancer could be underestimated. It is difficult to draw a conclusion about the prognosis of SPS from the present study because of the small number of patients and relatively short-term follow-up period. However, most previous studies also had small study populations due to the low prevalence of SPS. Thus, the present study is still the largest observational study of Asian patients with SPS.
In conclusion, the phenotype of SPS in Korean patients is somewhat different from that of Western patients. In Korean patients, SPS is more common in men and the total number of SSA/P is lower than that in Western patients, while the distribution of large SSA/P is similar. The incidence of CRC is lower in Korean patients, but this rate is higher than that in the general population. The high prevalence of synchronous adenomatous polyps is similar in Western and Korean patients. Although very few studies have evaluated the gastrointestinal tract, Korean patients tend to more frequently have abnormal gastric lesions. Our results show that Korean patients with SPS have a different phenotype from that of Western patients with SPS. Larger prospective studies in Asian SPS patients are needed to clarify the differences in phenotypes and formulate a surveillance guideline for Asian patients with SPS.


 XML Download
XML Download