

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Near-infrared (NIR) fluorescence imaging technique is well-studied and widely adopted to promote real-time image-guided surgery in various clinical fields [12]. Numerous studies for several fluorophores were conducted during the last decade. Among them, indocyanine green (ICG) is well known to be a harmless and appropriate fluorophore. It emits a fluorescence that peaks at a wavelength of approximately 840 nm illuminated by NIR light [3], and barely influenced by water or hemoglobin [4]. For this reason, ICG is widely used as a suitable fluorophore in lymphatic and biliary systems, which have numerous variations.
The hepatobiliary tract is regarded as one of the most difficult and complex anatomical systems. Unintended injuries to the bile duct or major vessels such as the portal vein and hepatic artery can give rise to debilitating morbidities and mortality [45]. To avoid and prevent iatrogenic injury to the bile duct, the NIR fluorescence imaging technique using ICG was adopted, and the efficiency of this technique was verified by several studies [6789]. With the improvement of minimally invasive surgical devices, a series of transition procedures to attain ICG imaging during operation is becoming readily available and simplified. However, there are still several barriers that should be overcome to proliferate this technique, including the high cost of the essential camera system and the discrepancies between real and fusion images.
In our institution, several studies have been investigated to verify the effectiveness of another fluorophore, sodium fluorescein (SF) [1101112]. SF is used widely as a diagnostic tool in the field of ophthalmology and optometry [1314]. With exposure to blue light, fluorescein has an excitation wavelength between 460 and 490 nm and an emission wavelength between 520 and 530 nm, and this emitted green light can penetrate thin tissue [15]. Due to these characteristics, SF was conventionally used in angiography. A few studies demonstrated the effectiveness of SF in several clinical fields [1101112] in our institution. In these previous reports, blue-light fluorescence technique using SF was applied in sentinel node mapping for gastric cancer and breast cancer, cholangiography, and liver mapping for hepatocellular carcinoma. In contrast with the NIR fluorescence technique using ICG, blue-light fluorescence does not require an expensive specific camera system, because blue-light fluorescence can be visualized with the conventional laparoscopic system. Furthermore, we can see the tracer and surrounding tissues simultaneously; there is no concern regarding the discrepancies between real and fusion images.
Based on the expertise from the previous reports, we hypothesized that SF can be used as an appropriate fluorophore in minimally invasive surgery (MIS) of the hepatobiliary system. Therefore, a preclinical study was designed to verify the feasibility of blue-light fluorescence technique using SF in a porcine model.
METHODS
Animal models
All experimental procedures were approved by the Institutional Animal Care and Use Committee of Korea University College of Medicine (No. KOREA-2019-0007). The procedure was performed in a total of 20 male 3-way crossbred (Landrace × Yorkshire × Duroc) pigs. The animals were housed at a constant temperature (23 ℃) and relative humidity (60%) with a fixed 12-hour light/dark cycle and had free access to water and food.
Fluorescent tracer (fluorophore)
We used 10% FLUORESCITE (Alcon Laboratories) as the fluorescent tracer. This solution contains SF, which is a yellow, water-soluble, organic dye that has been used as an imaging agent for retinal angiography since 1960. When exposed to light, SF has an excitation wavelength between 465 and 490 nm and an emission wavelength between 520 and 530 nm (i.e., it absorbs blue light and emits yellow or green light) [101516].
SF is metabolized in the liver and is mainly eliminated via renal excretion. The renal clearance of fluorescein is estimated at 1.75 mL/min/kg, while hepatic clearance is 1.50 mL/min/kg. Systemic clearance is essentially complete within 48–72 hours after administration of 500-mg SF.
Light source
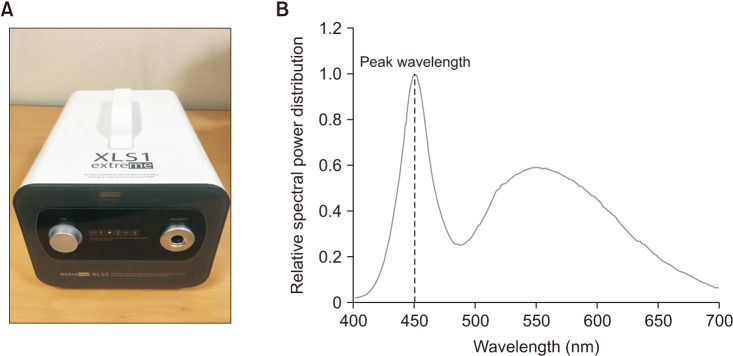
Blue light (a peak wavelength of 450 nm) was provided by a commercialized light-emitting diode (LED) light source (XLS1 extreme; Chammed) (Fig. 1). This light source was connected to a 5-mm rigid laparoscope (Karl Storz SE & Co. KG) via a fluid light cable (Karl Storz SE & Co. KG); on the tip portion of this laparoscope, a ring-shaped white-light source (Dokdo MDS) was conjoined (Fig. 2A).
Detailed procedures for the experiment
A pig was anesthetized with a mixture of alfaxalone (5 mg/kg), xylazine (2 mg/kg), and azaperone (6 mg/kg), and the following procedures were performed.
i) The 12-mm trocar was placed in the umbilicus of the pig and inflated with CO2 gas. Pneumoperitoneum was created and the intraabdominal pressure was maintained below 12 mmHg.
ii) Two additional ports were placed.
iii) The liver and gallbladder were identified under white light, and the gallbladder was pulled to the peritoneum.
iv) Five millimeters of SF solution was infused directly into the gallbladder. A small bile leak from the infused site was identified and clipped.
v) The biliary structures were observed under blue light emitted from an LED light source.
vi) The pig was euthanized at the end of the procedures.
RESULTS
The experiments were performed on 20 pigs. All images during the experiments were acquired using a digital recording device.
Visualization of the extrahepatic biliary tree under blue-light fluorescence
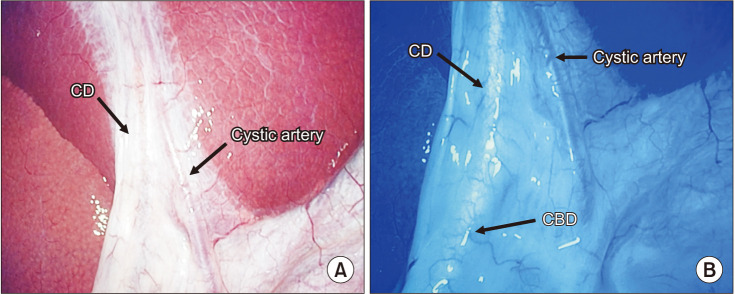
Before turning on the LED light source, we inspected the hepatobiliary structures under white light emitted from the ring-shaped light source (Fig. 3A). After injection of SF solution into the gallbladder, we turned off the white-light source and turned on the LED light source. Then, in 18 porcine models, the cystic duct and common bile duct were visualized by blue-light fluorescence (Fig. 3B).
Two cases of failed imaging
Of 20 porcine models, bile duct visualization failed in 2 cases. In 1 case, we underwent a considerable amount of dye leakage from the gallbladder, and therefore the hepatobiliary field could not be observed due to the leakage of SF. In another case, the extrahepatic biliary tree was not visualized, but lymphatics were visualized around the gallbladder.
DISCUSSION
Since MIS was first introduced, the indication of this technique has been dramatically expanded with the technical advancement of surgical devices and numerous studies to verify the feasibility and safety of MIS. This trend was also seen in the hepatobiliary system [17181920]. In the field of hepatobiliary system, laparoscopic cholecystectomy is considered as standard procedure for benign conditions such as cholecystitis and premalignancy lesion. However, gallbladders with severe inflammation, including gangrenous or xanthogranulomatous cholecystitis are also currently operated on by the MIS technique [21]. Furthermore, this technique is widely adopted in liver resection and bile duct resection, which have more complex anatomy and consist of critical structures. Concerning either benign or malignant conditions, accurate visualization of complex anatomy in the hepatobiliary system is the most important and desirable factor in MIS.
To obtain accurate visualization and identify relationships between the surrounding structures during operation, a real-time image technique was introduced, and numerous studies have been conducted [192021]. With the advancement of MIS technique and devices, real-time imaging techniques have been in progress as well. Recently, several researchers have introduced a NIR fluorescence imaging technique using ICG as a fluorescent tracer. ICG is the most popular tracer used for this purpose, as it is harmless to humans and is an appropriate fluorophore for image-guided surgery. ICG emits a fluorescence that peaks at a wavelength of approximately 840 nm when illuminated by NIR [4]. As this wavelength is long enough to penetrate connective tissue with a depth of 5–10 mm, NIR fluorescence is appropriate for visualizing hidden structures in humans. Moreover, NIR is barely influenced by water or hemoglobin and is therefore suited to tracing lymphatics, vessels, or biliary ducts.
Although several studies have reported the safety and effectiveness of clinical usage of ICG and NIR, the NIR fluorescence imaging had a drawback in that fluorescence imaging depends on the light source by which the fluorophore is excited. The critical shortcoming of NIR fluorescence arises from its long wavelength, which results in the NIR detecting camera system not visualizing the adjacent structures [10]. During the operation, the surgeon must turn on and off the NIR system to evaluate the NIR-detected target organ and adjacent structures. Recently, combined NIR and color imaging technology have been developed, and this advanced technology is compatible with laparoscopic and robotic surgery [2223]. Although many institutions around the world have established an MIS system, there is a disadvantage in that it is still very expensive for all institutions to have such advanced technological equipment.
To overcome these drawbacks of the NIR fluorescence technique, we reported SF as a fluorophore for fluorescence imaging in several clinical fields [1012]. SF is a widely accepted fluorescent dye that has been used as a tracer for retinal angiography, and, therefore, other researchers have investigated the feasibility of fluorescence imaging techniques using SF. Chang et al. [1] reported a sentinel lymph node detection technique using SF in breast cancer. SF was injected intradermally, and no systemic complications were detected. Although adverse effects of SF have been reported, most were trivial and considered as a safety solution for human use [2425]. Mohsen et al. [2627] reported fluorescence cholangiography using SF as a fluorophore with an ultraviolet light source. The result demonstrated only focal fluorescence on the biliary tract, and, therefore, has not been widely adopted as a technique for fluorescence cholangiography. With exposure to blue light, SF has an excitation wavelength between 460 and 490 nm and an emission wavelength between 520 and 530 nm, and this emitted green light can penetrate thin tissue. SF was ignored as a fluorophore, and its application was limited despite its safety, due to the short wavelength light. However, contrary to the previous concerns, we demonstrated that SF provided enough fluorescence to visualize the lymph nodes and lymphatics with an appropriate sensitivity [10]. In addition, to verify that blue-light fluorescence is an alternative to fluorescent imaging techniques in the hepatobiliary system, we reported a preclinical study in which the possibility of blue-light cholangiography and liver mapping with SF was demonstrated [11]. Afterward, to verify the clinical feasibility of the blue-light fluorescence with SF, the clinical outcomes of laparoscopic liver resection or video-assisted transthoracic liver resection using an intervention-guided fluorescence imaging technique were reported [12]. The results demonstrated a favorable outcome with a well-visualized target lesion in the liver.
In the current study, based on our expertise from the previous reports, we tried to unite the laparoscope and light source for blue-light fluorescence using SF. To provide both white light and pure blue light simultaneously, a ring-shaped light source was docked around the tip portion of conventional laparoscope. During the experiment using this modified laparoscope, as we could choose both white- or blue-light sources in 1 laparoscope, it was not necessary to manipulate the laparoscope and blue-light source separately; this also means we need not prepare an additional port for establishing the light source in laparoscopic approach.
Under blue light emitted from the modified laparoscope, the gallbladder and common bile duct were well visualized and distinguished from surrounding structures such as adipose tissue and liver tissue. If we succeed in our previous results regarding the diverse surgical fields, this ‘modified laparoscope’ concept can be expanded to various MIS including laparoscopic liver resection, cholecystectomy, and sentinel node mapping. In previous reports, we have already described that blue-light fluorescence using SF was advantageous in several issues; (1) no necessity of the image-fusion system; (2) lower hindrance to the standardization (i.e., cost and data burden); and (3) the possibility of time-lag due to image-fusion. In the next-phase study, our ‘blue-light source embedding laparoscope’ concept should be applied in the diverse fields of MIS.
The limitation of this preclinical study is that only 20 porcine models were involved in the experiment. There may be alterations in the study results due to differences in tissue thickness between individuals. Therefore, additional experiments using several porcine models are needed to verify the effectiveness of modified laparoscopic cameras and blue light imaging techniques in the future. Second, the SF was injected into the gallbladder directly. The safety and efficacy of SF with blue light should be verified by systemic injection such as portal flow. Third, the 5-mm laparoscope was modified for this study, and, therefore, the surgical view was not as comfortable as that of the commercial NIR fluorescence equipment in which a 10-mm laparoscope is usually embedded. In order to verify the definite advantages of blue-light fluorescence technique over NIR, it is necessary to develop new equipment that implements both LED and white light on a 10-mm laparoscope.
In conclusion, the authors demonstrated a preclinical result of a laparoscopic blue-light fluorescence imaging technique. It is necessary to demonstrate the clinical feasibility of these techniques during laparoscopic cholecystectomy and hepatectomy.

 XML Download
XML Download