

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The first case of coronavirus disease 2019 (COVID-19) was detected in Wuhan, China, in 2019, and it continues to be a global health crisis to this day.12 It is not only a threat to personal health but also a public health problem, nationally and internationally, affecting all areas, including the socioeconomic aspect.34567
Out-of-hospital cardiac arrest (OHCA) is a public health problem that is most closely related to death and is a prehospital task that has not yet been completely conquered.8910 It is widely known that the chain of survival is important for increasing the survival rate in OHCA, including early recognition, high-quality cardiopulmonary resuscitation (CPR), early defibrillation, and early advanced cardiac life support.1112 This chain of survival is highly dependent on the emergency medical services system (EMSS), which is significantly impacted by COVID-19.13
In the prehospital phase, it was reported in several countries, including Korea, that the incidence of OHCA increased, the emergency medical services (EMS) response time interval (RTI) was delayed, bystander CPR decreased, and the proportion of non-shockable rhythm increased during the pandemic, which affected survival rates.1415161718 However, in most studies, the study period was the initial period of the COVID-19 pandemic or the study group identified only short-term impacts in one city or a few cities.151719
This study aimed to investigate the effect of COVID-19 on OHCA patients. We compared prehospital return of spontaneous circulation (ROSC) of OHCA patients using the nationwide registry of EMS-assessed cardiac arrests for 1 year before and after the COVID-19 pandemic. Also, we investigated OHCA characteristics and EMS responses for 1 year before and after the COVID-19 pandemic.
METHODS
Study design and data source
Our study was a cross-sectional, retrospective, observational study using the nationwide registry of EMS-assessed cardiac arrests in Korea.
The nationwide EMS-assessed cardiac arrest registry comprised an EMS run sheet and EMS CPR registry. EMS providers filled out EMS run sheets for all emergency calls, including information on ambulance dispatch, patient symptoms, and treatment details. They also completed the EMS CPR registry for patients having a cardiac arrest, comprising cardiac arrest information based on the Utstein template.20
The first confirmed case of COVID-19 in Korea was reported on January 20, 2020. Subsequently, the Korea Disease Control and Prevention Agency (KDCA) defined the large-scale outbreak as a pandemic (when the number of confirmed cases rapidly increased) and classified it as a the first, second, and third outbreak.21
Study setting
The EMSS in Korea is a government-based (firefighting), single-tiered public service.
When an ambulance request is received from the 119-dispatch center, the dispatcher triages the patient whether the patient is in cardiac arrest. In the case of cardiac arrest, two or more ambulances or fire engine close to the scene are dispatched, and dispatch-assisted CPR (DA-CPR) is provided at the same time.2223 EMS providers comprise emergency medical technicians (EMTs) or registered nurses, and the scope of practice is similar to that of EMT-intermediate in the United States. They perform basic life support and can attempt intravenous access, supraglottic airway (SGA), and endotracheal intubation (ETI) under direct medical direction.24 The fire engine only provides basic life support resuscitation with automated external defibrillators.23
EMS providers perform resuscitation at the scene and during transport according to the 2015 American Heart Association guidelines.25 As the termination of resuscitation rule does not apply in Korea, EMS providers must transport patients having a cardiac arrest to the nearest capable hospital while performing CPR, unless otherwise specified, such as with a sign of obvious death (post-mortem stiffness, parenchymal prolapse, do not resuscitate order).
Study population
We analyzed OHCA cases recorded in the EMS-assessed cardiac arrest registry from January 19, 2019 to January 20, 2021.
All patients aged ≥ 18 years in whom resuscitation was attempted by an EMS provider were enrolled. Patients with do-not-resuscitate order, with signs of obvious death (arrest with signs of rigor mortis), and unknown EMS time interval information were excluded.
The cause of OHCA was classified as either presumed cardiac or noncardiac. Trauma, drowning, burns, asphyxia, drunkenness, and other noncardiac causes were classified as noncardiac causes. Unless evidence of a noncardiac cause was presented, the etiology of OHCA was presumed to be cardiac.26
Outcome measures
The primary outcome of the study was prehospital ROSC, which was defined as the resumption of perfusing cardiac activity, whether sustained or not, at the scene or during transport.
The secondary outcome was “ROSC in the Utstein comparator group,” which was defined as ROSC of an OHCA patient with presumed cardiac etiology, bystander witnessed, and initial recorded shockable rhythm.8
Variables and measurement
The main exposure of interest was the COVID-19 period.
The first confirmed case of COVID-19 in Korea was detected on January 20, 2020, and based on this, the previous year was defined as the non-COVID-19 period, and the following year was defined as the COVID-19 period.
A subgroup analysis was performed by defining the first, second, and third outbreak21 and 1 year before the first outbreaks as the non-pandemic period according to the pandemic period defined by the KDCA to confirm the impact of the outbreak period.
The collected variables were demographic factors (age, gender, location of arrest, and etiology), community factors (witnessed status and bystander CPR), prehospital factors (initial cardiac rhythm, EMS time intervals (RTI, the time interval from a call receipt to the first arrival of EMS at the scene; scene time interval [STI], the time interval from the arrival of EMS to departure from the scene; transport time interval [TTI], the time interval from departure from the scene to arrival at the hospital; multi-tier response, when two or more ambulances or fire engines arrived at the scene and responded jointly; and prehospital treatment).
RTI and STI of > 60 minutes were excluded because they were considered inappropriate time intervals.19
Statistical analysis
Descriptive analyses were performed to investigate the distribution of the study variables. Counts and proportions are used for categorical variables, and medians and interquartile ranges are used for continuous variables. Categorical variables were assessed using the χ2 test, and continuous variables were compared using the Mann-Whitney U test. The P values were based on a two-sided significance level of 0.05.
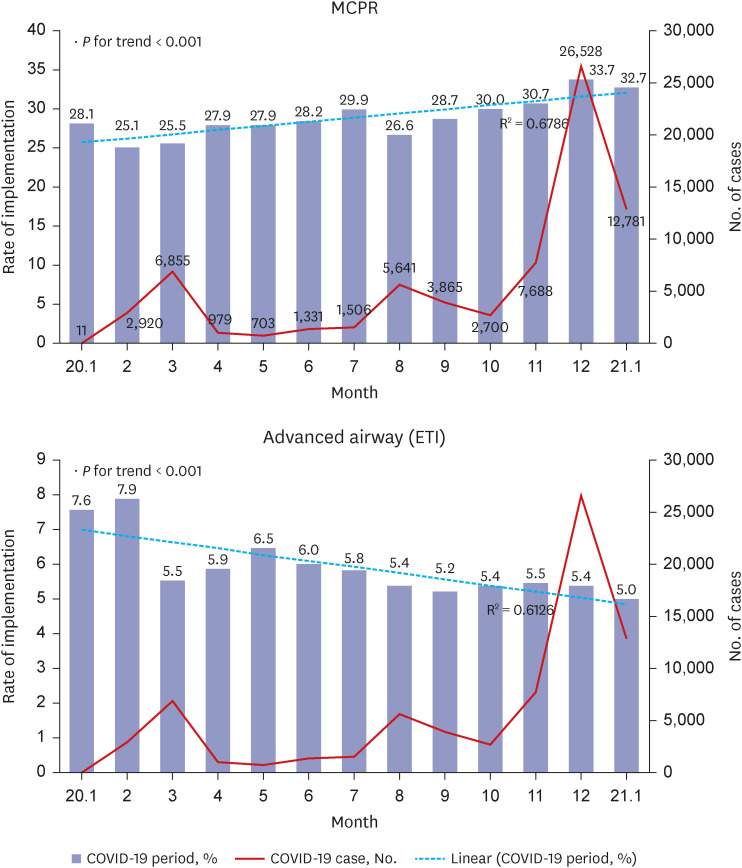
A Cochrane-Armitage trend analysis was conducted to confirm the trend of mechanical CPR (MCPR) and ETI implementation during the COVID-19 period.
Multivariable logistic regression was used to assess the effect of COVID-19 on OHCA patients with prehospital ROSC.
Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated, and covariates used for adjustment included factors known to influence survival from OHCA (age, gender, location of arrest, witnessed status, bystander CPR, initial cardiac rhythm, EMS time interval [RTI, STI, and TTI], multi-tier response, prehospital treatment [advanced airway management, epinephrine administration, and MCPR device]).
Separate multivariable logistic regression analyses were performed based on the outbreak period for subgroup analysis.
All statistical analyses were performed using R Statistical Software (version 4.1.2; The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Demographic findings
Among 62,749 EMS-treated OHCAs from 2019 to 2021, 51,921 cases were enrolled, including 25,355 (48.8%) during the non-COVID-19 period and 26,566 (51.2%) during the COVID-19 period (Fig. 1). The demographic characteristics according to the COVID-19 outbreak are summarized in Table 1.
Fig. 1
Diagram of study participants.
OHCA = out-of-hospital cardiac arrest, EMS = emergency medical service, COVID-19 = coronavirus disease 2019.
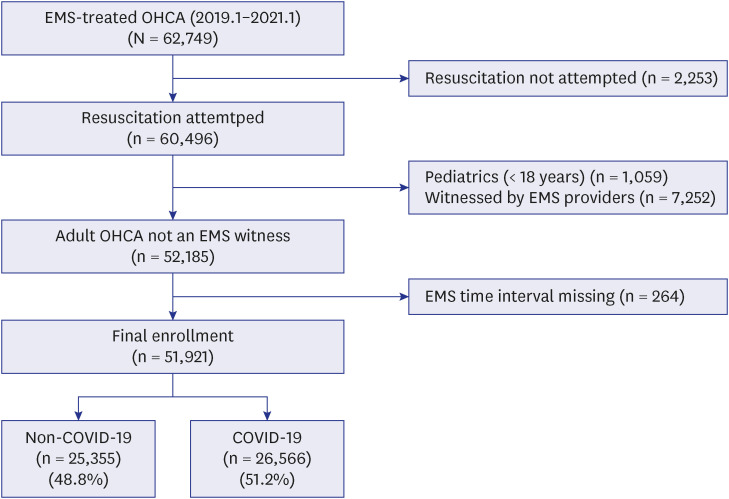
Table 1
Demographics of study population according to COVID-19 outbreak
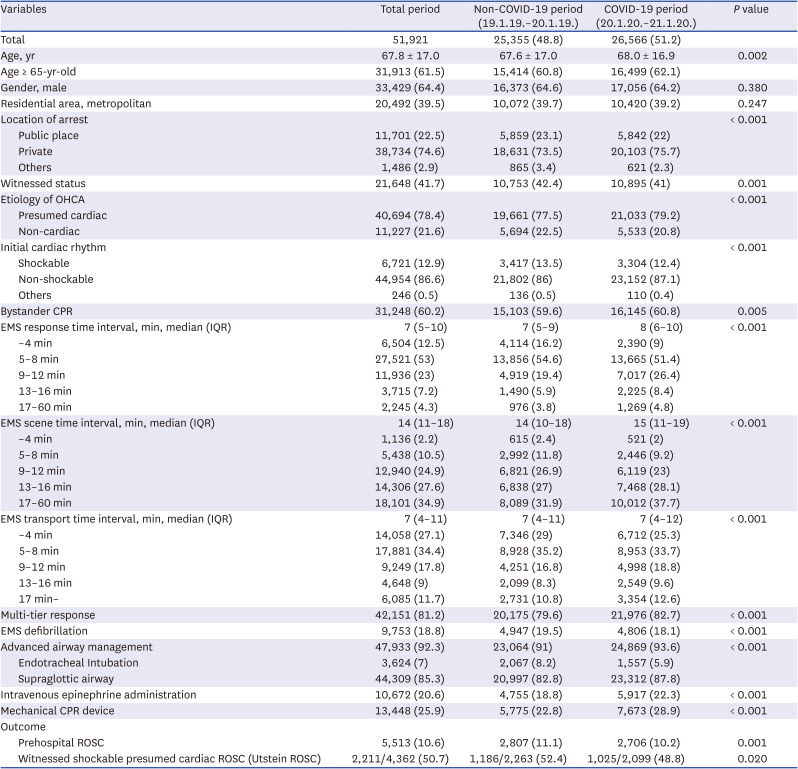
Values are presented as number (%) or mean ± standard deviation unless otherwise indicated.
COVID-19 = coronavirus disease 2019, OHCA = out-of-hospital cardiac arrest, CPR = cardiopulmonary resuscitation, EMS = emergency medical service, IQR = interquartile range, ROSC = return of spontaneous circulation.
Patients belonging to the COVID-19 period were older (mean ± standard deviation age was 68.0 ± 16.9 years vs. 67.6 ± 17.0 years, P = 0.002), with the arrest occurring more frequently in a private place (20,103 [75.7%] vs. 18,631 [73.5%], P < 0.001), with less number of witnesses compared with the non-COVID-19 period (10,895 [41%] vs. 10,753 [42.4%], P = 0.001).
Although there were more patients with presumed cardiac arrest during the COVID-19 period compared with the non-COVID-19 period (21,033 [79.2%] vs. 19,661 [77.5%], P < 0.001), more non-shockable rhythms were observed in the initial cardiac rhythm (23,152 [87.1%] vs. 21,802 [86%], P < 0.001).
The bystander CPR rate was higher in the COVID-19 period than in the non-COVID-19 period (16,145 [60.8%] vs. 15,103 [59.6%], P = 0.005).
Overall, all EMS time interval were longer during the COVID-19 period, and multi-tier response were more frequent during the COVID-19 period than during the non-COVID-19 period (21,976 [82.7%] vs. 20,175 [79.6%], P < 0.001).
Overall, advanced airway (SGA and ETI) was more prevalent during the COVID-19 period (24,869 [93.6%] vs. 23,064 [91%], P < 0.001), but among SGA and ETI, ETI was less prevalent (5.9% vs. 8.2%).
During the COVID-19 period, the rate of intravenous epinephrine administration was higher, and MCPR devices were applied more frequently than in the non-COVID-19 period. The number of cases wherein epinephrine and MCPR were used were 5,917 (22.3%) vs. 4,775 (18.8%) and 7,673(28.9%) vs. 5,775 (22.8%), respectively (P < 0.001).
As a result of the trend analysis, ETI showed a negative linear trend, and MCPR showed a positive linear trend, both of which were statistically significant (Fig. 2).
Main analysis
The prehospital ROSC decreased during the COVID-19 period compared with the non-COVID-19 period (10.2% vs. 11.1%, P = 0.001). This result was similar to that of the Utstein ROSC (48.8% vs. 52.4%, P = 0.020).
As a result of the multivariable logistic regression model (adjusted for age and gender), the AORs (95% CI) of ROSC and Utstein ROSC were 0.92 (0.87-0.97) and 0.84 (0.74-0.95), respectively.
In Model 2, adjustment variables (age, gender, location of arrest, witnessed status, bystander CPR, initial cardiac rhythm, EMS time interval [RTI, STI, and TTI], multi-tier response, prehospital treatment [advanced airway management, epinephrine administration, MCPR device]) were added and analyzed, and the AORs (95% CI) of COVID-19 period for ROSC and Utstein ROSC were 1.02 (0.96–1.09) and 1.05 (0.91–1.20), respectively, which was not statistically significant (Table 2).
Table 2
Multivariate logistic regression analysis for COVID-19 outbreak
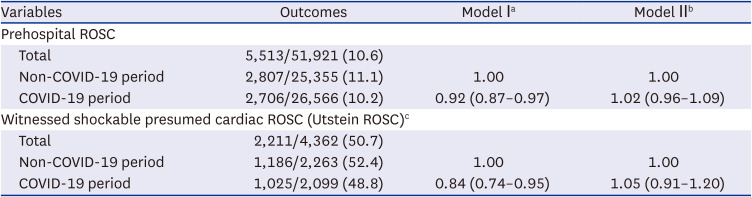
Values are presented as number/total number (%) or adjusted odds ratio (95% confidence interval).
COVID-19 = coronavirus disease 2019, ROSC = return of spontaneous circulation, CPR = cardiopulmonary resuscitation, RTI = response time interval, STI = scene time interval, TTI = transport time interval.
aAdjusted I for age (continuous), gender; bAdjusted II for age (continuous), gender, location of arrest, witnessed status, bystander CPR, initial cardiac rhythm, RTI/STI/TTI (continuous), mechanical CPR device, advanced airway management, epinephrine administration, multi-tier response; cUtstein ROSC Odd ratios were calculated adjusting for age (continuous), gender, location of arrest, bystander CPR, RTI/STI/TTI (continuous), mechanical CPR device, advanced airway management, epinephrine administration, multi-tier response.
Subgroup analysis
The prehospital ROSC was lowest in the third outbreak (9.1%), followed by the first (9.5%) and second (10.2%) outbreaks. The Utstein ROSC was lowest in the second outbreak, followed by the first and third outbreaks (47.6% vs. 47.9% vs. 48.8%, respectively; P = 0.106) (Table 3). When the non-pandemic period was used as a reference, the odds ratio (95% CI) of the multivariate logistic regression model adjusted for age, gender, location of arrest, witnessed status, bystander CPR, initial cardiac rhythm, and EMS time interval (RTI, STI, and TTI) was 0.89 (0.80–0.99), 0.98 (0.89–1.08), and 0.94 (0.84–1.05) for the first, second, and third outbreaks of prehospital ROSC, respectively (Table 4). Among these, only the first outbreak was significant. In the Utstein ROSC, no significant results were found during the entire outbreak.
Table 3
Demographics of sub-group study population according to large-scale outbreak of COVID-19 period
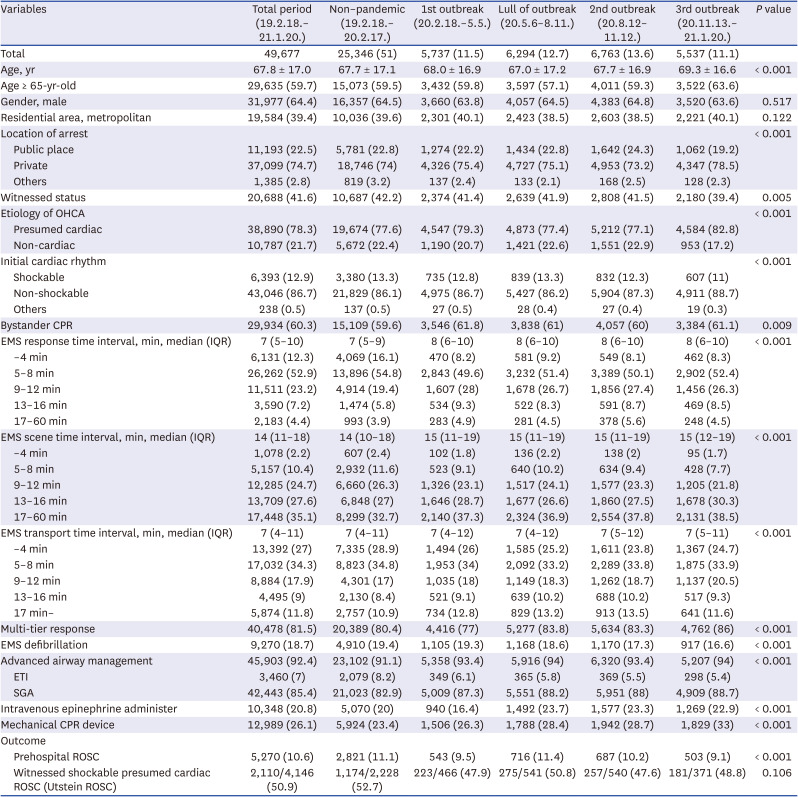
Values are presented as number (%) or mean ± standard deviation unless otherwise indicated.
COVID-19 = coronavirus disease 2019, OHCA = out-of-hospital cardiac arrest, CPR = cardiopulmonary resuscitation, EMS = emergency medical service, IQR = interquartile range, ETI = endotracheal intubation, SGA = supraglottic airway, ROSC = return-of-spontaneous circulation.
Table 4
Multivariate logistic regression analysis of sub-group according to large-scale outbreak of coronavirus disease 2019 period
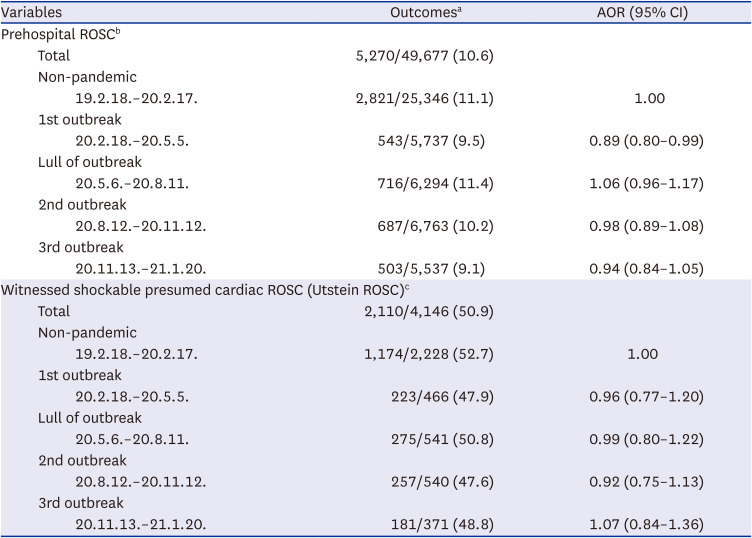
AOR = adjusted odds ratio, CI = confidence interval, ROSC = return-of-spontaneous circulation, CPR = cardiopulmonary resuscitation, RTI = response time interval, STI = scene time interval, TTI = transport time interval.
aValues are presented as number/total number (%); bPROSC ORs were calculated adjusting for age (continuous), gender, location of arrest, witnessed status, bystander CPR, initial cardiac rhythm, RTI/STI/TTI (continuous); cUtstein ROSC ORs were calculated adjusting for age (continuous), gender, location of arrest, bystander CPR, RTI/STI/TTI (continuous).
DISCUSSION
Our study evaluated changes in the characteristics, EMS responses, and outcomes of OHCA patients during the COVID-19 period using the nationwide EMS-assessed cardiac arrest registry for 2 years.
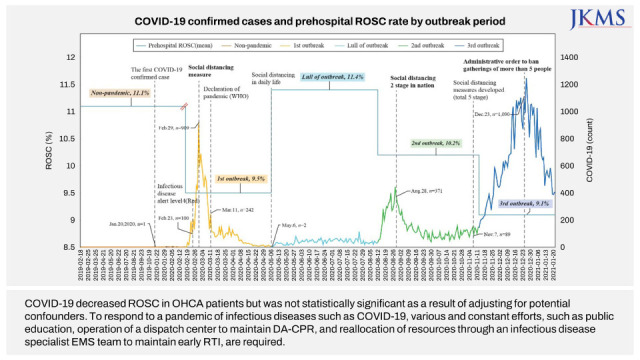
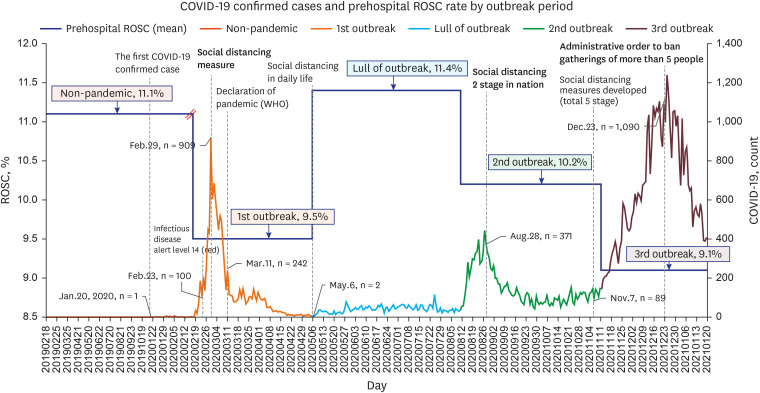
The location of arrest, witnessed status, etiology of arrest, initial cardiac rhythm, EMS time interval (RTI, STI, and TTI), and prehospital ROSC changed during the COVID-19 period. These results were also confirmed by the outbreak period, and the result was more prominent during the third outbreak, which had the highest number of confirmed cases (Fig. 3).
Fig. 3
The number of COVID-19 confirmed cases and the proportion of out-of-hospital cardiac arrest patients with prehospital ROSC by large-scale outbreak period.
COVID-19 = coronavirus disease 2019, ROSC = return of spontaneous circulation, WHO = World Health Organization.
However, in terms of the prehospital ROSC, no significant difference was found between the COVID-19 and non-COVID-19 periods when potential confounders were adjusted. Through subgroup analysis, only the first outbreak period, which started the COVID-19 outbreak, showed a causal relationship with the decrease in the prehospital ROSC rate with COVID-19.
Bystander CPR is a well-known factor that is conducive to improving OHCA survival. During the COVID-19 period, many studies reported that fear of infection reduced bystander CPR,2728 which was also associated with decreased survival rates. Unlike other studies, our study reported an increase in the bystander CPR rate.
During the COVID-19 period, continuous efforts were made to initiate DA-CPR in the dispatch center, and it is considered to be the reason the bystander CPR rate did not deteriorate. In addition, while CPR education decreased during the COVID-19 period, the increase in bystander CPR rates was due to the maintenance effect of previous efforts to improve bystander CPR, and more constant efforts are needed in the future.17293031
The COVID-19 period had an impact not only on bystander CPR but also on the response time of EMS providers. The RTI was delayed, and the STI and TTI increased. Among them, RTI is a factor that has been found to be critically related to the survival rate of OHCA patients3233343536 and to shorten RTI, it is necessary to maintain the priority response system in time-critical diseases such as cardiac arrest, even in infectious disease situations.
In addition, efficient allocation of limited resources is required through policies such as operating an infectious disease ambulance dedicated to transporting patients with mild infectious diseases, including patients with simple fever, or restricting the transport of patients with mild infectious diseases by applying a prehospital triage program.3738394041
COVID-19 is transmitted by direct contact or by droplets discharged through the respiratory tract, increasing the risk of infection during aerosol-generating procedures. CPR is a procedure that generates aerosols through chest compression and tracheal intubation; therefore, EMS providers are recommended to wear PPE before contact with cardiac arrest patients to prevent infection.424344 However, while wearing PPE reduces the risk of infection in EMS providers, it may increase RTI, cause communication difficulties between EMS providers, and reduce CPR quality due to increased fatigue.1745464748
Consequently, a mechanical chest compression device is recommended as an alternative, which has a great advantage in that EMS providers can minimize contact with OHCA patients with confirmed or suspected COVID-19, particularly during the COVID-19 period.49 However, the MCPR and survival rate of OHCA patients are still controversial; therefore, selective use is required.5051 An increase in MCPR can be identified in this study as well, which may be because of COVID-19; however, it may also be due to increased popularity of MCPR equipment, education, and an increase in transport time to hospitals; thus, additional research is needed.
Tracheal intubation is a procedure vulnerable to aerosol generation during CPR.52 However, the reliability of the seal is better than that of SGA and facial mask, and to prevent additional risk due to prolonged use of non-invasive ventilation, early intubation is recommended before SGA, if possible, in the guidelines.49 In addition, if the use of a video laryngoscope is available and EMS providers are trained, intubation through a video laryngoscope is recommended, which has the advantage of the EMS provider being farther away from the patient's airway than the conventional method.53
Successful ETI is one of the advanced skills that must be supported by past ETI experience and abundant training. However, it is not easy to perform ETI while wearing PPE during the COVID-19 period. We found that the use of ETI decreased, and the use of SGA increased during the COVID-19 period. Among the reasons that can explain this result, it is expected that SGA was more preferred over ETI by EMS providers who were not accustomed to wearing PPE.
Therefore, tracheal intubation using video laryngoscopy and MCPR education are required in a special environment, and efforts to improve the survival rate in OHCA patients through team CPR education by integrating them are needed.
An increase in OHCA incidence and a low survival rate are related during the COVID-19 period and affect the OHCA outcome despite the low COVID-19 incidence. However, previous studies had a short study period.1554555657
Our study was a relatively long-term study, and considering the overall low COVID-19 incidence area, no increase in the incidence of OHCA was observed. ROSC decreased during the COVID-19 period; however, when the multivariable analysis was performed, no statistical significance was observed except for the first outbreak.
This is because bystander CPR, which is the key to survival, was maintained, and the variables confounded by COVID-19 were adjusted, suggesting that it is possible to prepare for other pandemics by making various efforts, such as system operations that allocate dedicated ambulances for OHCA to improve RTI.
First, as a study conducted in Korea, it is challenging to generalize the EMS system to all situations because it is different for each country or region.24 In particular, Korea is a country with a relatively well-controlled COVID-19 situation, and the rapid increase in the number of confirmed cases that exceeds our surge capacity may lead to different results.
Second, due to the retrospective nature of this study, other variables that affect OHCA outcomes, such as socioeconomic status,58 CPR experience of the EMS provider,59 medical history, and quality of CPR, were not measured and adjusted. Also, because the National Fire Agency has the drive to convert on-site CPR from basic life support to advanced life support, there could be longer scene time interval, more placing advanced airway, and more administrating epinephrine. In order to exclude this effect, we performed multivariable logistic regression analysis in model 2 with the above variables adjusted.
Although we attempted to adjust for potential confounders, this adjustment may have been limited. However, well-controlled randomized control trials in situations such as the COVID-19 period are practically challenging.
Third, although prehospital management of OHCA patients with traumatic or other noncardiac etiology is different from that of OHCA patients with cardiac etiology, it was not considered in our study. If the research group is limited to OHCA of cardiac etiology, the effect of COVID-19 on OHCA may be under-interpreted.
Fourth, our study has limitations in evaluating survival outcomes using only the nationwide registry of EMS-assessed cardiac arrests. However, ROSC is correlated with the prognosis of survival to discharge from the hospital with a good neurological status, which is a long-term outcome, with ROSC being designated as a core variable in the Utstein outcome report.60
Fifth, we compared ROSC of patients with OHCA of presumed cardiac etiology, but COVID-19 could have changed the etiology of OHCA.616263 Actually, during the COVID-19 period, the number of patients withholding resuscitation cases increased from 32,236 to 37,931.4964 Further research is needed in this portion because of the limitations of our study dataset. In order to overcome this effect as much as possible, in our study, we compared the Utstein ROSC, and the result was observed identically.
In conclusion, COVID-19 decreased ROSC in OHCA patients but was not statistically significant as a result of adjusting for potential confounders. To respond to a pandemic of infectious diseases such as COVID-19, various and constant efforts, such as public education, operation of a dispatch center to maintain DA-CPR, and reallocation of resources through an infectious disease specialist EMS team to maintain early RTI, are required.
 XML Download
XML Download