

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As the global coronavirus disease 2019 (COVID-19) pandemic continues to sweep across the globe, reports of kidney involvement in adult patients with COVID-19 have been published, and recently, cases in pediatric patients have also been documented. In this report, we present the case of a formerly healthy 11-year-old male, who presented with rapidly progressive glomerulonephritis (RPGN) immediately after a COVID-19 infection.
CASE DESCRIPTION
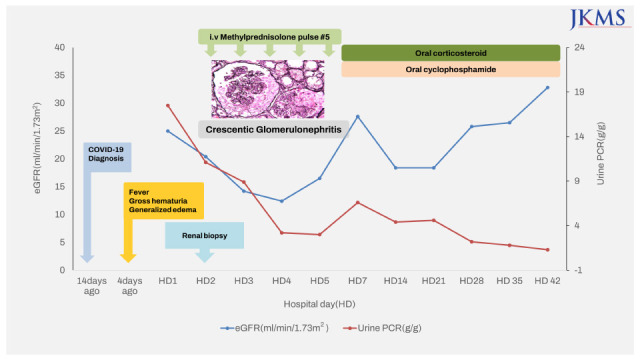
An 11-year-old boy presented to our hospital with gross hematuria, generalized edema, and fever of 3 days duration. He had a history of COVID-19 infection two weeks prior with a mild fever. He was not vaccinated against COVID-19 and had no other exhibiting symptoms of infection, such as upper respiratory tract infection or gastrointestinal symptoms. He had normal urinalysis results at a school medical check-up six months prior and had no underlying disease or family history. At the time of admission, the patient was febrile (body temperature, 39°C) and hypertensive at 139/89 mmHg (> 95th percentile). The patient’s laboratory test results upon admission were as follows: white blood cell count, 14,730/uL; erythrocyte sedimentation rate, 93 mm/h; C-reactive protein level, 6.9 mg/dL; blood urea nitrogen level, 39.4 mg/dL; serum creatinine level, 2.44 mg/dL; estimated glomerular filtration rate (eGFR, calculated by Schwartz bedside equation), 16.6 mL/min/1.73 m2; sodium, 130 mmol/L; potassium, 5.4 mmol/L; total protein content, 6.2 g/dL; albumin level, 3.6 g/dL; calcium, 8.3 mg/dL; phosphorus, 5.7 mg/dL; uric acid level, 10.6 mg/dL; spot urine protein/creatinine ratio, 17.5 g/g; creatinine and 24-hour urine protein excretion, 7,124.7 mg/day. Complement levels were within the normal ranges and autoantibodies including antineutrophil cytoplasmic antibody and anti-glomerular basement membrane (GBM) antibody were all absent. Ultrasonography of the kidney revealed increased parenchymal echogenicity and swelling. His urine output was within normal range without oliguria (600–1,200 mL/day). On hospital day 2, considering the patient’s clinical presentation (Fig. 1) of rapid and progressive acute kidney injury (AKI) accompanied by gross hematuria, proteinuria, and hypertension, methylprednisolone (MP) pulse therapy was initiated, and a renal biopsy was performed the next day. Renal biopsy specimens (Fig. 2) revealed crescentic immune-complex glomerulonephritis. Nineteen out of 36 glomeruli (53%) showed crescentic formation (17 cellular, 2 fibrocellular) and there was no tubulointerstitial change on light microscopy. Immunofluorescence revealed diffuse mesangial immunoglobulin (Ig)G, IgA, C3, Kappa and Lambda deposit. Electron microscopy demonstrated profuse subendothelial and mesangial electron-dense deposits, numerous leukocytes in the capillary lumen (endocapillary proliferation), extensive foot process effacement with microvillous transformation, and intraluminal leukocytes, ruling out IgA nephropathy. Consequently, we diagnosed the patient with post-COVID-19 infection-associated de novo crescentic immune-mediated glomerulonephritis. After five treatments of MP pulse, oral prednisolone and cyclophosphamide treatment for 12 weeks were started. On hospital day 10, we started antihypertensive treatment with calcium channel blocker due to persistent hypertension. After antihypertensive treatment, his systolic blood pressure was maintained around 120 mmHg. Azathioprine was added as the maintenance therapy after the induction therapy of cyclophosphamide treatment for 12 weeks. After these medical treatments for 5 weeks, his renal function began to recover gradually. Currently, 20 weeks later, his level of serum creatinine was 0.87 mg/dL and an eGFR of 69.5 mL/min/1.73 m2.
Fig. 1
Trend of laboratory test results of the patient during hospitalization.
eGFR = estimated glomerular filtration rate, PCR = protein creatinine ratio, i.v. = intravenous.
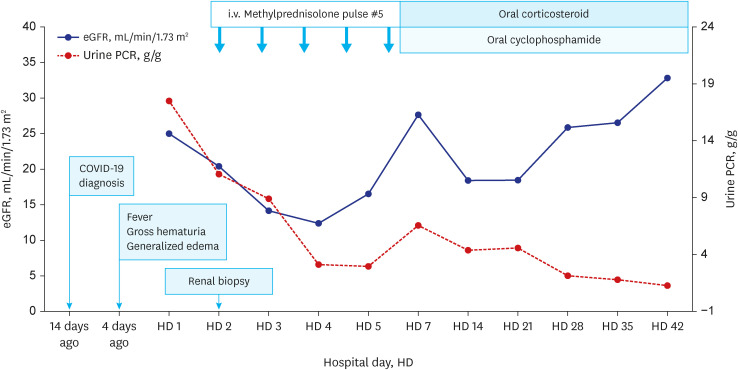
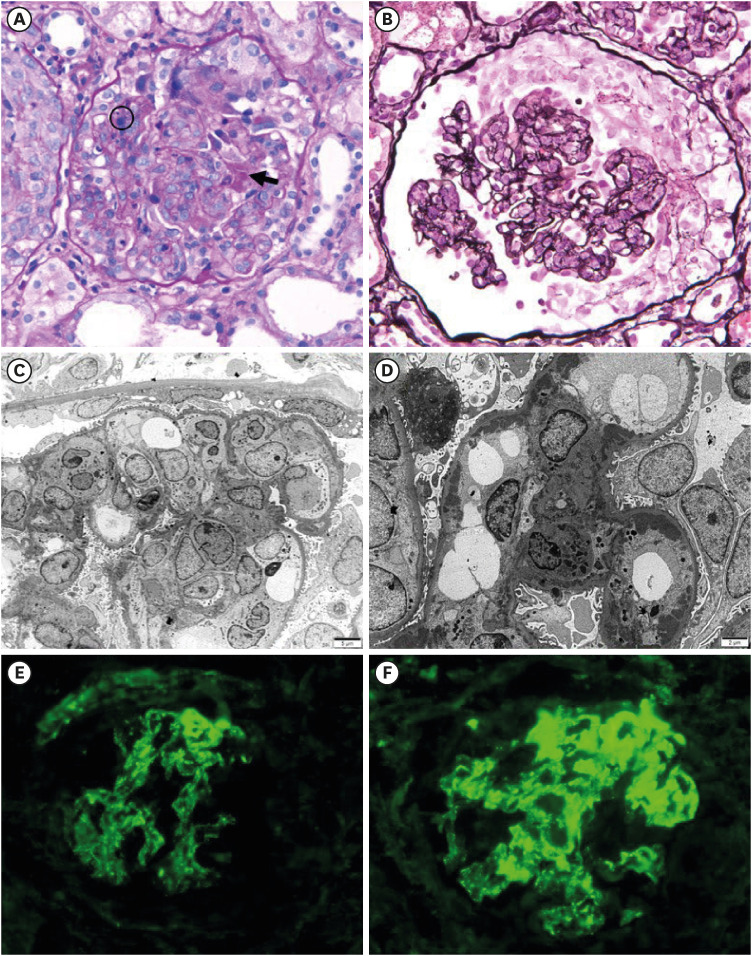
Fig. 2
Renal pathologic findings of the patient. (A) Endocapillary proliferation with some neutrophils and karyorrhexis (circle: karyorrhexis), fibrinoid necrosis and cellular crescent (arrow: fibrinoid necrosis) (H&E ×400). (B) Endocapillary proliferation with cellular crescents (PAM ×400). (C) Many leukocytes in the capillary lumens (endocapillary proliferation) and extensive foot process effacement with microvillous transformation. (D) Many subendothelial and mesangial electron dense deposits and intraluminal leukocyte. (E, F) Immunofluorescence revealed diffuse mesangial C3 (E) and IgA (F) deposit (×400).
H&E = hematoxylin and eosin, PAM = periodic acid methenamine silver.
DISCUSSION
RPGN begins with acute glomerulonephritis or nephropathy, as renal function continues to deteriorate by more than 50% from weeks to months. Histopathologically, it is a disease characterized by the formation of glomerular epithelial crescents invading more than 50% of the total glomeruli.1 RPGN is broadly classified into type I (anti-GBM nephritis), type II (immune-complex-mediated glomerulonephritis), and type III (pauci-immune glomerulonephritis), according to histopathology and immune-complex deposition. According to a previous Korean pediatric report on RPGN, among 12 pediatric patients diagnosed with RPGN, type II RPGN was identified in 10 patients, accounting for more than 80% of RPGN cases.1 The patient in this case was also subsequently diagnosed with type II RPGN.
Recent studies have documented various kidney complications that occur after a COVID-19 infection in children. Nomura et al.2 reported on a multi-institutional cohort of five unvaccinated pediatric patients with COVID-19 and associated kidney dysfunction with histological descriptions. Three patients with COVID-19 had multifactorial thrombotic microangiopathy with clinical features of hemolytic uremic syndrome (n = 2) or disseminated intravascular coagulation (n = 1). Two patients with COVID-19 in the study presented with nephrotic syndrome. After a brief follow-up period, the kidney function of none of the patients returned to its baseline level.2 N et al.3 presented a case of glomerulonephritis in the setting of AKI in a child with COVID-19. Kidney biopsy specimens showed IgA nephropathy with crescentic glomerulonephritis, acute tubular injury, and focal medium-artery vasculitis. The patient exhibited severe symptoms with rapid progression to end-stage kidney disease (ESKD).3
The mechanism of COVID-19 related renal complications is unclear. The postulated mechanisms of COVID-19 related renal injury include sepsis-associated AKI, dysregulation of immune system, complement activation of the microvascular system, activation of cytokine, and dysfunction of coagulation.2 In this case, we suggest that immune complex-mediated glomerular injury via immune system dysregulation can be the possible pathogenetic mechanism based on the pathologic findings of multiple immune complex deposits.
Furthermore, some studies have suggested that kidney complications can occur even after vaccination against COVID-19. In adults, cases of minimal change disease (MCD) have been reported following previous vaccination. In the current COVID-19 era, three cases of new-onset MCD following inoculation with the Pfizer-BioNTech COVID-19 vaccine were reported.456 Likewise, the Moderna COVID-19 vaccine has also been linked to a case of MCD.7 One notable pediatric case diagnosed with crescentic glomerulonephritis after the second dose of the Pfizer-BioNTech COVID-19 vaccine resulted in the patient eventually progressing to ESKD despite undergoing dialysis.8 In our case, his renal function was slowly recovering after MP pulse therapy and we continued oral corticosteroid and cyclophosphamide for 12 weeks without dialysis, based on the general treatment guideline of immune complex-mediated crescentic glomerulonephritis.
Based on the aforementioned studies, it appears that a variety of kidney complications can occur after COVID-19 infection or vaccination, although these cases are extremely rare. This report highlighted the first pediatric case of post-COVID-19 infection-associated de novo crescentic immune-mediated glomerulonephritis with RPGN. It is recommended to monitor renal function and do a thorough evaluation if renal symptoms appear after COVID-19 infection or vaccination.
 XML Download
XML Download