

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Asthma has various phenotypes, and neutrophilic asthma is one of the most representative forms of T-helper 2 (T2) low asthma.1 It presents with severe and persistent symptoms, and the prevalence of neutrophilic asthma has been reported in up to 30% of all asthma cases.2 However, the mechanism underlying neutrophilic asthma has not been fully elucidated.3 Some studies showed that the increased interleukin (IL)-17 pathway seems to be involved.14 Other studies commented that the nature of corticosteroid resistance is the key of controlling neutrophilic asthma, which is usually explained by histone deacetylase 2 (HDAC2) activity.56 HDAC2 regulates the acetylation of pro-inflammatory gene expression and plays a key role in controlling inflammatory cytokines.78 It is diminished in neutrophilic asthma compared with its activity levels in T2 high asthma.59
Tiotropium bromide (TIO) is a long-acting anticholinergic agent that improves chronic airway disease by improving the remodeling of airway smooth muscle and by controlling neuronal acetylcholine (ACh).10 The Global Initiative for Asthma (GINA) recommends TIO as an add-on therapy to moderate to high doses of inhaled corticosteroids with long acting β2 agonists in step 4 or step 5 treatment, as well as in T2 low neutrophilic asthma.11 The anti-inflammatory effect of TIO by modulating IL-8 and IL-17 with HDAC2 were shown in chronic obstructive pulmonary disease (COPD) study.1213 However, the role of TIO in neutrophilic asthma is not fully understood.
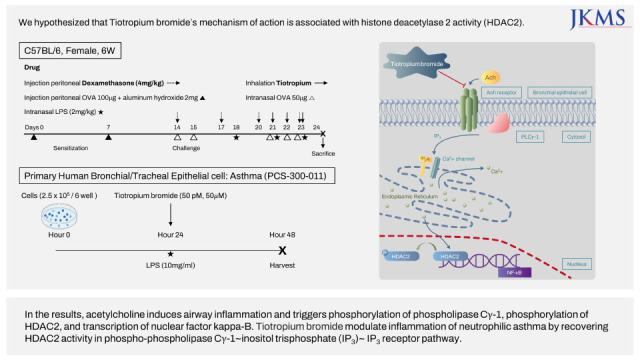
We developed the neutrophilic asthma mouse model and performed associated studies.5914 In the previous study, we showed the improvement of airway hyperresponsiveness and attenuation of airway inflammation after TIO was treated.9 In case of inflammatory cytokines, IL-17A and IL-5 were attenuated in TIO treated neutrophilic asthma mouse model.9 However, the association of reduced HDAC2 activity in neutrophilic asthma and the effect of TIO treatment remains controversial.1215 We hypothesized that TIO improves neutrophilic asthma by recovering HDAC2 activity.
METHODS
In-vivo mouse model and protocol of drug administration
We investigated in vivo study with TIO and dexamethasone (DEX) by using same protocol which was developed in previous studies (Fig. 1).9 T2 inflammation was induced by sensitizing the mice with ovalbumin (100 μg) (OVA; Sigma-Aldrich, St. Louis, MO, USA) and aluminum hydroxide (2 mg) (Sigma-Aldrich). It was dissolved in saline and injected into the peritoneum on days 0 and 7 in six-week-old female C57BL mice (Orient Bio., Seongnam, Korea). After sensitization, neutrophilic inflammation was induced by intranasal administration of OVA (50 μg) and lipopolysaccharide (LPS) (2 mg/kg). OVA was administered on days 14, 15, 21, 22, and 23, while LPS was administered on days 18, 21, and 23.
Fig. 1
Schematic flow of the acute neutrophilic asthma mouse model. The mice were sensitized with OVA on days 0 and 7. OVA was challenged intranasally on days 14, 15, 21, 22, and 23. Neutrophilic inflammation was induced by intranasal LPS which was administered on days 18, 21, and 23. Dexamethasone was intraperitoneally administered on days 14, 17, 20, and 23. Tiotropium bromide was inhaled on days 21, 22, and 23.
OVA = ovalbumin, LPS = lipopolysaccharides.
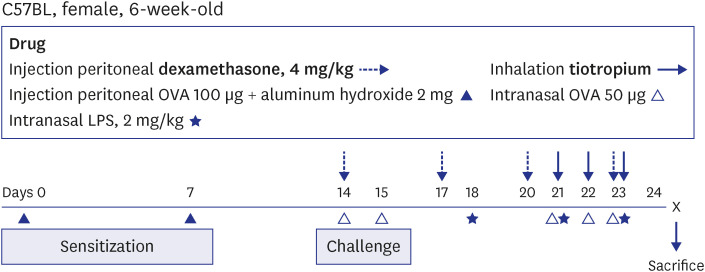
TIO (25 μg/mL) was inhaled for three minutes per mouse in the inhalation chamber on days 21, 22, and 23. DEX (4 mg/kg) was administered on days 14, 17, 20, and 23 via peritoneal injection. The five mice of each were randomly allocated into four groups: 1) control, 2) OVA + LPS (O+L), 3) OVA + LPS + DEX (O+L+D), and 4) OVA + LPS + TIO (O+L+T).
Broncho-alveolar lavage (BAL)
BAL was performed via the cannulated trachea with a silicon tube. We instilled 0.8 mL of cold sterile PBS into the lung and withdrew the BAL fluid. After ten minutes of centrifugation, the supernatant was stored at −80°C for further analyses. Then, 50 μL aliquots of BAL fluid were centrifuged at 750 rpm for five minutes and stained with Diff-Quick (Sysmax, Kobe, Japan). Total cell counts were obtained using the LUNA automated cell counter. The percentages of macrophages, eosinophils, lymphocytes, and neutrophils were measured by counting 500 leukocytes of the slides under a light microscope in the BAL fluid.
Measurement of HDAC2 activity
HDAC2 activity in the mouse lung tissue was measured using the colorimetric EpiQuik HDAC2 Activity Assay Kit (Epigentek, Farmingdale, NY, USA) according to the manufacturer’s instructions. Nuclear fractions were collected and incubated in a plate with an HDAC substrate for 90 minutes at 37°C. After washing the plate, the capture antibody was added for 60 minutes, and the detection antibody was added for 30 minutes at room temperature. The absorbance was recorded at 450 nm using a microplate reader (BioTek, Winooski, VT, USA).
Measurement of nuclear factor kappa B (NF-κB) and C-X-C motif chemokine ligand 1 (CXCL1)
Well-known cytokines such as NF-κB and CXCL1, which were associated with HDAC2 and neutrophilic inflammation, were measured in this study. Nuclear proteins were extracted and collected from tissue samples using a nuclear extraction kit (Abcam, Cambridge, UK). The activity of NF-κB was assessed using a NF-κB p65 transcription factor assay kit (Abcam) following the manufacturer’s protocol. We measured the levels of pro-inflammatory cytokines in the BAL fluid, such as CXCL1. Enzyme-linked immunosorbent assay kits were used for the analyses (R&D Systems, Minneapolis, MN, USA).
In-vitro model and protocol of drug administration
We subsequently conducted an in-vitro study to clarify the inflammation cascade of TIO with HDAC2 at the cellular level. In previous article, mechanism of action of TIO was explained by phospho-phospholipase Cγ-1 (p-PLCγ-1) and inositol trisphosphate (IP3)-mediated intracellular release of ionized calcium (Ca2+).16 Also, IP3-medicated nuclear Ca2+ signal was a well-known key factor which controls HDAC2 activity in various human cells, including airway epithelium.17 Therefore, we planned to evaluate the upper cascade signals of PLCγ-1 and IP3 receptor (IP3R). IP3R existed in the endoplasmic reticulum (ER) and associated with the conjugated with IP3 and adjacent Ca2+ efflux channel.18
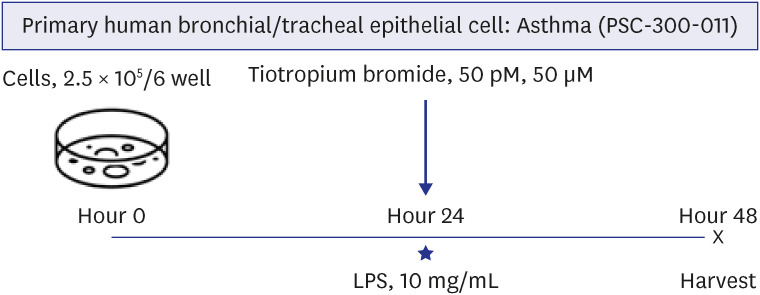
We used primary human bronchial/tracheal epithelial (HBE) cells from asthma patients (PCS-300-011; ATCC, Manassas, VA, USA). Cells were cultured in bronchial epithelial cell basal medium (ScienCell, San Diego, CA, USA) with Bronchial Epithelial Growth Kit (ATCC). A 0.1% penicillin-streptomycin 100X solution was used to control bacterial contamination. The cells (2.5 × 105/6well) were placed in the culture plates and cultivated. After 24 hours of culture, TIO was administered at concentrations of 50 pM and 50 μM in the culture medium. After 1 hour, LPS (10 mg/mL) was stimulated for 5 minutes. The cells were harvested after 24 hours of administration of LPS (Fig. 2).
Fig. 2
Schematic flow of in-vitro model for acute neutrophilic asthma. Primary human bronchial/tracheal epithelial Cell: Asthma (PCS-300-011) (ATCC, Manassas, VA, USA) was cultivated. After 24 hours of culture, Tiotropium bromide was administered to the culture medium (50 pM and 50 μM). After 1 hour, LPS (10 mg/mL) was stimulated for 5 minutes. After 48 hours, the cells were harvested for analyses.
LPS = lipopolysaccharide.
Western blot analysis
Western blot analyses were performed to detect the levels of p-PLCγ-1 and IP3R according to the treated medication (LPS, TIO 50 pM, and TIO 50 μm). HBE cells were lysed in PRO-PREP protein extraction solution (iNtRON Biotechnology, Seongnam, Korea) and centrifuged. Concentrations were assessed using the Bradford method. The protein samples were separated by 6% and 10% sodium dodecyl sulfate polyacrylamide gel electrophoresis and transferred to a nitrocellulose membrane (Amersham Pharmacia Biotech, Little Chalfont, UK). After blocking with 5% skimmed milk (Difco, BD, San Jose, CA, USA), the membrane was incubated overnight with a p-PLCγ-1 (Abcam), IP3R (Abcam), and β-actin (Santa Cruz Biotech, Dallas, TX, USA). The membrane was washed three times with TBST and incubated with a secondary antibody for 2 hours (Santa Cruz Biotech). The target proteins were detected using the ECL western blotting analysis system (Thermo Fisher Scientific, Rockford, IL, USA). Relative density was compared with β-actin in the western blot results. We either exposed the membrane to X-ray film or analyzed it with an LAS 3000 image analyzer (Fujifilm, Tokyo, Japan). The band intensity was quantified and compared with image software (Multi Gauge, Version 3.0, Fujifilm Life Science, Tokyo, Japan).
Statistical analyses
We used one-way analysis of variance to evaluate the effect of medication on HDAC2 activity, NF-κB activity, and BAL CXCL1 in in-vivo study. Same analyses were performed on p-PLCγ-1 and IP3R in in-vitro study. Post-hoc analyses using Dunnett’s multiple comparison tests were used to compare multiple groups both in in-vivo and in-vitro study. Statistical significance was set at P < 0.05. All analyses were performed using GraphPad Prism 5.01 (GraphPad Software, San Diego, CA, USA).
RESULTS
TIO improves NF-κB and CXCL1 in neutrophilic asthma mouse model
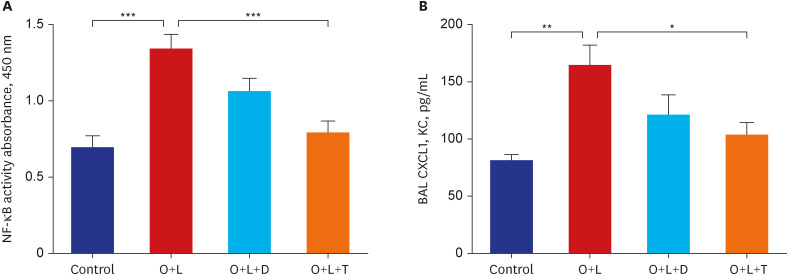
Neutrophilic asthma was well-induced in this study as well as in the previous articles.914 The O+L group (neutrophilic asthma-induced group) showed significant increases in NF-κB activity at 450 nm absorbance compared to that of the control (P < 0.001). The level of CXCL1 in the BAL fluid was also elevated in the O+L group compared with the control group (P < 0.01). These results reveal that inflammation in neutrophilic asthma is associated with NF-κB activity and CXCL1. In the drug challenges, DEX, a traditional drug for asthma, treated group (O+L+D group) did not improve levels of both NF-κB activity and CXCL1 compared with the O+L group. However, the TIO treated group (O+L+T group) showed statistically significant improvement in both NF-κB activity and CXCL1 compared with the O+L group (P < 0.001 and P < 0.05, respectively) (Fig. 3). TIO showed significant improvements in cytokines which were associated with neutrophil recruitment and their inflammation in this study.
Fig. 3
Measurement of nuclear factor kappa B activity and C-X-C motif chemokine ligand 1. Proinflammatory cytokines, such as NF-κB and CXCL1, were measured and compared among groups. Tests were conducted in four groups: control, O+L, O+L+D, and O+L+T. (A) The O+L group showed elevated NF-κB activity compared to that of the control (P < 0.001). The O+L+T group showed improvement in NF-κB activity compared to that of the O+L group (P < 0.001), which was not observed in the O+L+D group. (B) The BAL CXCL1 levels were higher in the O+L group than in the control group (P < 0.01). The O+L+T group showed lower BAL CXCL1 levels than those observed in the O+L group (P < 0.05), which was not observed in the O+L+D group. O+L vs. all (*P < 0.05, **P < 0.01, ***P < 0.001).
O = ovalbumin, L = lipopolysaccharides, D = dexamethasone, T = Tiotropium bromide, NF-κB = nuclear factor kappa B, CXCL1 = C-X-C motif chemokine ligand 1, BAL = bronchoalveolar lavage.
TIO recovers HDAC2 activity in neutrophilic asthma mouse model
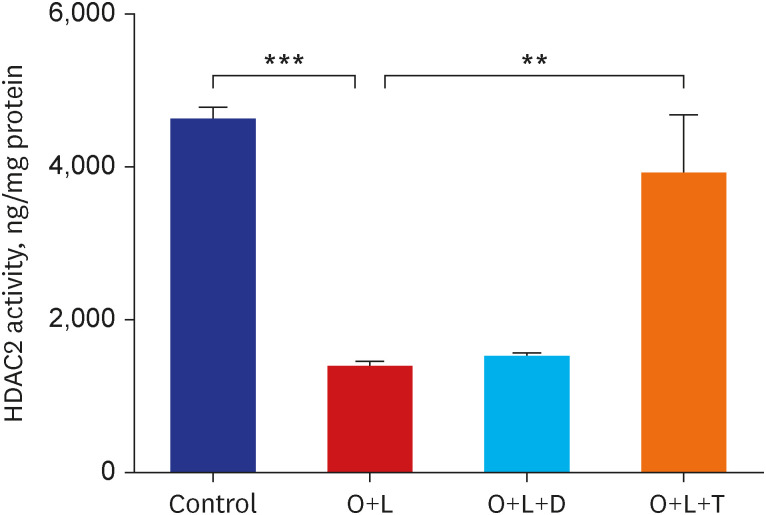
HDAC2 activity in the O+L group was significantly lower than that in the control group (P < 0.001). To analyze the effect of DEX and TIO on HDAC2 activity, both were administered after neutrophilic inflammation was induced. HDAC2 activity did not recover after DEX treatment (O+L+D group). However, it recovered dramatically after TIO treatment (O+L+T group) compared to that of O+L group (P < 0.01) (Fig. 4). These results indicate that TIO restored HDAC2 activity in neutrophilic asthma, which was not seen after DEX treatment.
Fig. 4
Measurement of histone deacetylase 2 activity. HDAC2 activity was measured. The tests were conducted in four groups: control, O+L, O+L+D, and O+L+T. It was decreased in the O+L group compared to that in the control group (P < 0.001). This did not improve after dexamethasone treatment. Unlike dexamethasone, Tiotropium bromide recovered HDAC2 activity compared to that of the O+L group (P < 0.01). O+L vs. all (**P < 0.01, ***P < 0.001).
HDAC2 = histone deacetylase 2, O = ovalbumin, L = lipopolysaccharides, D = dexamethasone, T = Tiotropium bromide.
TIO modulates p-PLCγ-1-IP3-IP3R pathway in neutrophilic inflammation-induced primary HBE cells from asthma patients
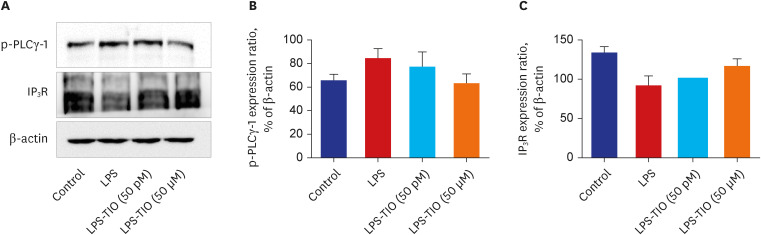
After inducing neutrophilic inflammation by LPS in HBE cells from asthma patients, the density of p-PLCγ-1 was elevated and that of IP3R was diminished relatively compared with those of control group although there was no statistical significance. After TIO was treated, the density of p-PLCγ-1 was attenuated and that of IP3R recovered compared with LPS-treated HBE cells from asthma patients. Those changes showed tendency with elevated TIO concentration from 50 pM to 50 μM (Fig. 5). These tendencies showed that TIO was associated with the p-PLCγ-1-IP3-IP3R pathway.
Fig. 5
Western blot analysis for a phospho-phospholipase Cγ-1 and inositol trisphosphate receptor. We used western blot analyses (A) to detect the levels of p-PLCγ-1 (B) and IP3R (C). These experiments were conducted in four groups: control, LPS, LPS-TIO (50 pM), and LPS-TIO (50 μM). Band intensity was quantified with image software (Multi Gauge, Version 3.0, Fujifilm Life Science, Tokyo, Japan). The p-PLCγ-1 expression ratio was increased and the IP3R expression ratio was reduced in the LPS group. Along with the increase in TIO concentration from 50 pM to 50 μM, those ratios were relatively recovered as in the control group.
p-PLCγ-1 = phospho-phospholipase Cγ-1, IP3R = inositol trisphosphate receptor, LPS = lipopolysaccharide, TIO = Tiotropium bromide.
DISCUSSION
Among the different types of severe asthma, neutrophilic asthma is characterized by corticosteroid-resistance, poor lung function, and frequent exacerbation.121920 Corticosteroid resistance is the reason why neutrophilic asthma is difficult to treat.21 The 2022 GINA guidelines have an isolated session for difficult-to-treat and severe asthma.22 They recommended alternative add-on therapy such as long-acting muscarinic antagonist (LAMA), azithromycin, leukotriene receptor antagonist (LTRA), low-dose oral corticosteroid (OCS), or bronchial thermoplasty for severe asthma.22
However, there is a lack of studies on which drugs are suitable for neutrophilic asthma. Macrolides showed no additive effect, but there are potential benefits for corticosteroid-sparing therapy in patients with neutrophilic asthma in our previous study.5 In the AMAZE and AZISAST trials, which were conducted to reveal the effect of azithromycin on difficult-to-treat or severe asthma, azithromycin showed benefits in controlling non-eosinophilic inflammation.2324 However, there are certain issues on antibiotic resistance, and these studies were not conduct for neutrophilic asthma only.2324 Moreover, LTRA did not significantly improve neutrophilic asthma.25 Currently available LTRAs are cysteinyl leukotriene 1 receptor antagonists, which usually does not preferentially bond to the leukotriene B4 receptor, which modulates neutrophilic inflammation.26 Low-dose add-on OCS is also not effective in treating “corticosteroid-resistant” neutrophilic asthma and usually has many side effects.12 Lastly, bronchial thermoplasty has not been studied enough to support its use in neutrophilic asthma or its long-term safety.27 Therefore, the emerging role of LAMA in neutrophilic asthma must be considered. Neutrophilic asthma has a mechanism similar to that of COPD.28 Neutrophilic inflammation induced by Th17 cells was upregulated in both neutrophilic asthma and COPD.28 In previous research, we already revealed that the TIO was significantly better in improving IL-17A level of neutrophilic asthma than systemic corticosteroids.9
In this study, we revealed some interesting aspects of TIO in neutrophilic asthma. First, we showed that TIO improved inflammation in neutrophilic asthma by improving HDAC2 activity. HDAC2 activity is a key step in controlling pro-inflammatory cytokines, which is diminished in neutrophilic asthma.82930 It suppressed the conjugation of p53 and NF-κB, which lead to transcription of NF-κB dependent inflammatory protein coding gene in nuclear DNA.31 The activity of HDAC2 was impaired in neutrophilic asthma and recovered after TIO was treated in this study. We showed the reasonable explanation of the effect of TIO in the neutrophilic asthma. Second, the improvement of HDAC2 activity was significant after TIO treatment, which was not seen after DEX treatment. Irresponsiveness of DEX was explained by diminished HDAC2 activity.5 Usually, corticosteroid acts as anti-inflammatory drugs by binding to glucocorticoid receptors binding with HDAC2 and cyclic adenosine monophosphate response element binding protein in nucleus.30 With the impaired HDAC2 activity in neutrophilic asthma, corticosteroids cannot much improve inflammation.530 On the other hand, a sole use of TIO recovered HDAC2 activity in this study. This effect of TIO might be independent with the use of corticosteroid according to the results of this study. Also, TIO consistently showed more benefits than corticosteroids in neutrophilic asthma from our previous and current studies.9 Based on these evidence, TIO should be considered as a preferred option for controlling T2 low neutrophilic asthma. Third, we showed that the tendency of p-PLCγ-1 and IP3R were improved with the elevation of TIO concentration in in-vitro study. The association of TIO, IP3/IP3R, and intracellular Ca2+ in various cells was showed in previous studies.1516173233 The association of IP3 and HDAC2 was also described previously.17 Intracellular Ca2+ and its associated Ca2+ channel were well-known steps of deciding HDAC2 activity.51618 However, there was no evidence of TIO, IP3/IP3R, and HDAC2 activity in neutrophilic asthma until now. Therefore, we can hypothesize a potential mechanism of action of TIO in neutrophilic asthma by inflammation cascade of TIO, IP3, IP3-medicated Ca2+, HDAC2, NF-κB, and CXCL1 as follows. Initially, it is associated with the ACh receptor on airway epithelial cells, which is the main target of TIO. ACh-stimulation leads to the subsequent phosphorylation of PLCγ-1 in the HBE cell membrane. When phosphorylated to p-PLCγ-1, it releases IP3 and combines with IP3R on the ER. After IP3 and IP3R are conjugated, Ca2+ is released from the ER to the cytoplasm. Endoplasmic Ca2+ depletion usually leads to a decrease in the level of HDAC2, which cannot modulate NF-κB activity and CXCL1. As far as we know, we firstly described the association of this inflammation cascade in neutrophilic asthma (Fig. 6).
Fig. 6
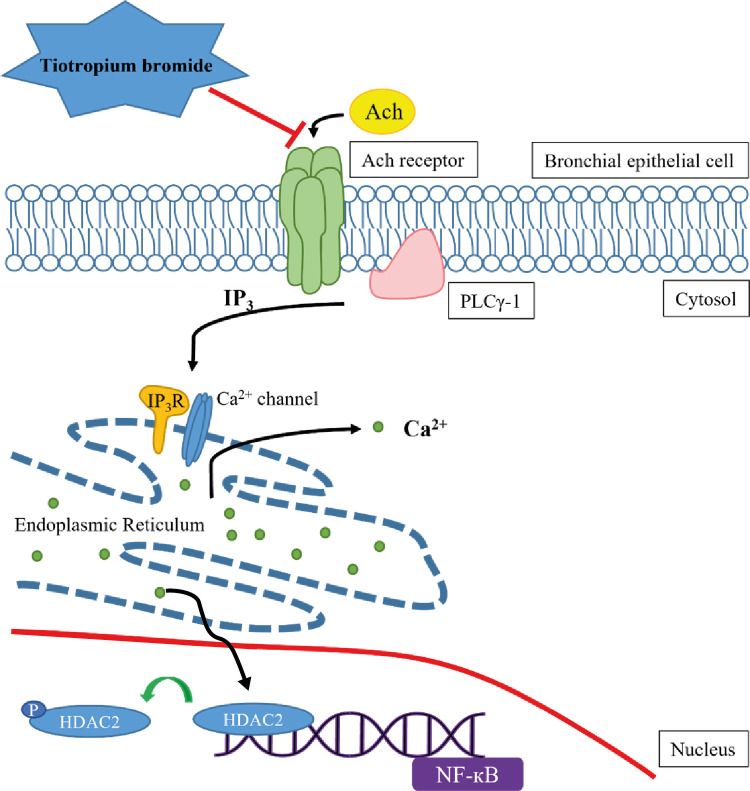
Proposal of possible mechanism of p-PLCγ-1-IP3-IP3R pathway controlled by TIO in neutrophilic asthma. ACh induces airway inflammation by attaching to its receptor in bronchial epithelial cells. It triggers phosphorylation of PLCγ-1, which leads to an increased level of IP3. It binds to IP3R and IP3-favor calcium channel in the ER. Ionized calcium ions are depleted in the ER. Then, HDAC2 is deactivated by phosphorylation, and NF-κB transcription is triggered in the nucleus. TIO blocks the ACh receptor, which is the highest level of controlling inflammation in neutrophilic asthma. It is mediated by the p-PLCγ-1-IP3-IP3R pathway.
ACh = Acetylcholine, PLCγ-1 = phospholipase Cγ-1, IP3 = inositol trisphosphate, IP3R = inositol trisphosphate receptor, ER = endoplasmic reticulum, HDAC2 = histone deacetylase 2, NF-κB = nuclear factor kappa B, TIO = Tiotropium bromide.
Our study had a few limitations. First, we did not explore the combined effects of corticosteroids and TIO in-vitro. We cannot describe the interaction between corticosteroids and TIO at the intracellular level. However, this study aimed to clarify the inflammatory mechanism of TIO in neutrophilic asthma. Therefore, we were able to discern the answer to this question. Second, we did not show the statistical significance in the western blot analyses. However, the tendency of the western blot band was obvious, and the result showed consistent tendency according to the elevation of concentration of TIO. More number of mice should be considered in future study for statistical validation. Third, we used the primary HBE cells from asthma patients and showed the indirect evidence of intracellular Ca2+-medicated inflammation cascade via p-PLCγ-1 and IP3/IP3R. However, we showed the key steps for this inflammation cascade, which was enough for explaining the involvement of intracellular Ca2+.161718 More direct measurement of intracellular Ca2+ and administration of IP3 agonist, such as adenophostin A, before and after TIO treatment should be considered in future in-vivo study.34
Conclusively, we demonstrated the potential intracellular mechanism of action of TIO in neutrophilic asthma. These data are valuable for reconsidering the position of TIO in managing neutrophilic asthma, which is preferred add-on option.
 XML Download
XML Download