

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gastritis is a condition with inflammation proven by esophagogastroduodenoscopy or biopsy of gastric mucosa, and is divided into acute and chronic gastritis according to the time course.1 In the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) classification, which has been used since 1994, the gastritis code (K29) was classified into acute gastritis and chronic gastritis. However, the concept of Helicobacter pylori, an important cause of gastritis and gastric ulcer, is not included at all, and it has a limitation as a classification in which the types and causes of gastritis are mixed.2 At the Kyoto consensus meeting held in 2014, gastritis classification was unified according to the causes of gastritis, and H. pylori gastritis was classified as an infectious gastritis and its importance was emphasized.3 In addition, the concept and algorithm for H. pylori-associated dyspepsia were presented and the importance of eradication treatment was emphasized. However, the description for endoscopic classification of gastritis is complex and has not yet been verified in many research studies.
Due to the spread of endoscopic equipment and the screening endoscopic practice, endoscopically diagnosed gastritis has become a common finding. According to a study that investigated the distribution of gastritis findings by dividing endoscopic gastritis into superficial gastritis, erosive gastritis, atrophic gastritis, and intestinal metaplasia among 25,536 people who visited health check-up centers of 40 institutions in Korea, 21,943 people (85.9%) had at least one gastritis, and only 3,593 (14.1%) had normal findings.4 Superficial gastritis was the most common with 31.3%, followed by atrophic gastritis (27.1%), erosive gastritis (23.7%), and intestinal metaplasia (7.1%). In the case of atrophic gastritis and intestinal epithelial metaplasia, there are not many studies in Korea that have investigated the prevalence in the general population through biopsy. In a study in which atrophic gastritis and intestinal metaplasia were diagnosed using the Sydney system in 389 adults without digestive disorders, the prevalence of atrophic gastritis was reported to be 42.5% in the antrum and 20.1% in the body, and the prevalence of intestinal epithelial metaplasia was 28.6% in the antrum and 21.2% in the body.5 Significant risk factors for intestinal metaplasia were H. pylori infection, age over 61, and smoking history. Since atrophic gastritis and intestinal metaplasia are known as premalignant lesions, accurate diagnosis, classification, treatment, and follow-up are particularly important in Korea, where the incidence of gastric cancer is the highest in the world.
Erosive gastritis is gastritis with damage to the mucosa limited to the mucosal layer and is caused by use of drugs such as non-steroidal anti-inflammatory drugs (NSAIDs), stress, drinking alcohol, and H. pylori infection.6 If there are symptoms with gastritis, erosive gastritis can be the target of treatment. The management of symptoms is covered in the functional dyspepsia guideline published in 2020.7 However, apart from symptoms, drugs are sometimes used to improve erosive gastritis lesions, so we included the effects of proton-pump inhibitors (PPIs) and mucoprotective agents on erosive gastritis in the key clinical question list.
H. pylori infection usually causes no symptoms, but it does cause chronic gastritis, is associated with atrophic gastritis and intestinal metaplasia, and is known to be an important risk factors for gastric cancer.8 There are studies that eradication of H. pylori is associated with a reduction in the incidence of gastric cancer, but there is disagreement as to whether eradication improves atrophic gastritis and intestinal epithelial metaplasia. Considering the high prevalence of atrophic gastritis and intestinal metaplasia and the high incidence of gastric cancer in Korea, recommendations on this issue based on the evidence are needed. Therefore, in this guideline, recommendations were developed to help physicians properly diagnose and treat erosive gastritis, atrophic gastritis, and intestinal epithelial metaplasia, which require treatment or follow-up. However, the scope of this guideline dealt with the controversial and clinically important topics rather than covering all of the above gastritis. Gastritis is a disease that is frequently encountered in primary care centers and screening settings, and in order to gather opinions from primary physicians and specialists together, a multi-disciplinary committee including the Korean College of Helicobacter and Upper Gastrointestinal Research (KCHUGR), the Korean Society of Gastroenterology, the Korean Gastric Cancer Association, the Korean Physicians’ Association, and the Korean Academy of Family Medicine was formed. Users of this guideline are intended for physicians of all medical institutions who will be in charge of the diagnosis and treatment of gastritis.
PROCESS OF DEVELOPMENT
Composition of the clinical practice guidelines committee
The clinical practice guidelines committee was composed of the steering committee and the working group. The steering committee led by the society president and executives established strategies and directions for guideline development, and reviewed and approved the budget. It also coordinated the stakeholders in the development of guidelines and oversaw the independence of the development. The working group was formed with the members of the KCHUGR, with members recommended by the Korean Society of Gastroenterology, the Korean Gastric Cancer Association, the Korean Physicians’ Association, and the Korean Academy of Family Medicine. One methodological expert also participated in the working group, making a total of 12 members. The internal and external reviewers consisted of two members each. The first meeting was held on May 26, 2020, and a total of 26 working group meetings, workshops, and working group voting meetings were held until December 2, 2021. A total of eight key questions were made, and eight recommendations were derived for key questions.
Clinical guideline development process
The clinical practice guidelines for gastritis were first attempted in Korea, and overseas guidelines were reviewed to establish the scope and target of the guidelines.3691011 Since the scope and quantity of the clinical practice guidelines of gastritis were very broad from the review of foreign guidelines, it was decided to limit the current practice guideline to topics that are important or controversial in clinical practice.
Selection of key questions
The selection of key questions on the recommendation of clinical practice guidelines was confirmed through a meeting attended by all members of the working group in consideration of foreign guidelines and the domestic practice situation. Key questions for each recommendation were selected under the principles of population, intervention, comparison, and outcome (PICO), and based on this, a systematic literature search was conducted. The key questions for each category are presented in Supplementary Table 1.
Literature search and selection
For the literature search, a search formula was established by deriving primary search terms through discussion between methodological experts and working group members in charge of each key question.
Based on this, a search was conducted in five databases: MEDLINE (PubMed), Embase, Cochrane Library, KoreaMed, and KMbase. In the case of gastritis, there are many papers published only in Korean, and it is expected that there will be many contents on those papers to be contributed in the guidelines, so KMbase search was added. All searches were performed in October 2020. In the search for all key questions, there was no exclusion based on year, language, or publication status. After the searched articles were merged using EndNote, duplicates were excluded through title, author name, publication year, and journal name. The final completed search formula was presented in the Supplementary Material 1.
In the process of selection of evidence, two working group members were assigned to each key question and performed selection of article according to inclusion criteria independently. The process of selection of literature was carried out according to the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) flow diagram.12 The individual selection process for each key questions was added in the Supplementary Figs. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20. The inclusion and exclusion criteria for each key question for literature selection were derived and applied in the form of each PICO.
Literature quality assessment and meta-analysis
The quality assessment of primary literature was used separately according to individual study design. Cochran Risk of Bias (ROB) 2.013 for randomized controlled trials, Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I)14 for the non-randomized study, Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2)15 for the diagnostic study, Quality in Prognostic Studies (QUIPS) for the prognostic study, and Assessing the Methodological Quality of Systematic Reviews (AMSTAR2)16 for the systematic review literature were used for quality assessment. The quality evaluation of literatures was independently performed by two working group members for each key question, and discrepancies in evaluation results were decided through consensus between the members in charge and methodological experts. To minimize the discrepancy between the assessment results among the working group members, a workshop on literature quality assessment was conducted. The evaluation results of the individual level of evidence were presented in each key question section.
A meta-analysis was performed when there was no unexplainable heterogeneity in the included studies and when two or more outcomes were included. However, if the study designs were different, they were presented separately instead of being analyzed by meta-analysis. In addition, when several articles were published in the same cohort study, the most recently published study or the article containing the most study subjects were selected and included in the final meta-analysis. For meta-analysis, a random effect model was applied because significant diversity exist in the cause of gastritis and the heterogeneity of the results was confirmed through I2. The meta-analysis included all outcomes of benefits and harms attributable to targeted interventions.
Derivation of recommendations and determination of recommendation strength and level of evidence
The strength of recommendation and level of evidence were evaluated according to the evaluation criteria of strength of recommendation and level of evidence presented by the grading of recommendations assessment, development, and evaluation (GRADE; http://www.gradeworkinggroup.org) group. The final treatment recommendation was decided through the internal and external review process. The recommendation grade was determined by evaluating the degree of benefits and harms of each intervention based on the evidence. The recommendation grade was determined by dividing it into 4 grades (general use [Do, Strong], selective use [Do, Conditional], limited use [Do not, Conditional], and general use restriction [Do not, Strong]) according to the strength and direction of the recommendation (Table 1). Recommended strength ‘strong’ means that most well-informed patients choose the intervention method when the desired effect of the intervention is clearly greater than the undesirable effect. Recommended strength ‘conditional’ means that it is uncertain whether the desired effect of an intervention outweighs the undesirable effect, and a well-informed patient can choose another intervention method. ‘Selective use’ means that the use of the treatment may vary depending on the clinical situation or the values and preference of the patient, so it is suggested to use it selectively or conditionally.

Table 1
Classification of recommendation strength and direction and the balance of benefits and harms of each recommendation class
![]()
The GRADE level of evidence was decided through a discussion process between methodological experts and members who in charge of individual key questions. Through the GRADE methodology, the objectivity of the level of evidence evaluation and the same evaluation criteria were maintained within the clinical practice guideline. All levels of evidence were assigned to individual clinical outcomes in key question, and the level of evidence presented for each recommendation was in accordance with the level of evidence for the most important outcome of key questions. The level of evidence was classified into four levels: high, moderate, low, and very low (Table 2). Once the level of evidence was classified according to the study design included in key questions, the lowering and higher certainty of evidence were considered as the following criteria. In the case of a randomized controlled trial, if there were 1) risk of bias, 2) inconsistency (heterogeneity), 3) indirectness, 4) imprecision, and 5) publication bias, the level of evidence was downgraded by level 1 to 3. In the case of observational studies, if 1) the size of the effect was large, 2) there was a dose-response relationship, or 3) all plausible confounding variables were adjusted or explained, the level of evidence was raised.17

Table 2
Level of evidence
![]()
Through a summary of findings and the level of evidence, the members in charge of key questions first developed the recommendation and recommendations grade with consideration of the strengths and limitations of the evidence included in the recommendation, the balance of benefits and harms, the values and preferences of patients, obstacles to implementation, and financial or technical applicability.
Consensus and adoption of recommendations
The principle of the recommendation grading process is that if more than 80% of all members in the working group participate and more than 70% vote in favor, the decision is evaluated as reaching consensus. If more than 70% of the votes were not in favor, a second round of voting was conducted by drafting an amendment through discussion among the members. As a result of the first vote, seven of the nine recommendations were passed and adopted, and the two recommendations that did not pass were revised and a second round of voting was conducted. At the second round of voting, the two revised recommendations reached consensus, and it was finally decided that the eight recommendations were agreed upon. The key questions and recommendations are presented in Table 3.
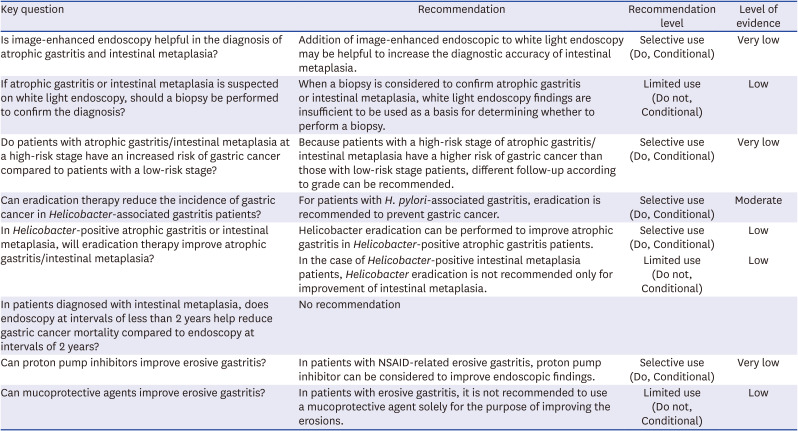
Table 3
Summary of key questions and recommendations
![]()
Internal and external review
For internal review, the manuscript prepared by the working group was peer-reviewed by two experts in the gastroenterology field who did not directly participate in the guideline development. The remarks pointed out in the expert evaluation were corrected and reflected through the internal discussion process of working group. In addition, an external review was conducted by two methodological experts, and corrections were made after internal discussion on the comments pointed out.
At the 2021 Fall Symposium and Postgraduate Course of the KCHUGR held on October 30, 2021, the draft clinical practice guidelines including all eight recommendations were presented to members composed of gastroenterologists, and opinions were collected through an open discussion.
Financial support of clinical guideline development and independence of development
Although this guideline was developed with the budget support from the KCHUGR without any external financial support, this clinical guideline development committee was operated independently of the academic society. The support from the KCHUGR did not directly, indirectly, or potentially affect the contents of the guidelines or the guideline development process. All members participating in the development conducted the following investigations to confirm that there is no conflict of interest or potential interest. 1) In the past two years, if you have received support or key money of more than 10 million won on a topic related to the development of guidelines, 2) If you have experience in conducting research with financial support from a specific institution or pharmaceutical company, 3) If the right to economic interests, such as stocks, is provided from an organization related to the development of the guideline, 4) If an official or unofficial title is provided by the organization related to the development of the guideline, and 5) If there were drugs to which you own intellectual property rights related to the development of the guideline. As a result of the investigation, it was confirmed that there were no conflicting or potential interests.
Dissemination of clinical guidelines and update plan
This guideline is published in domestic and international medical journals of gastroenterology or internal medicine and posted on the academic society website and Facebook so that any physician can easily download and use it. In addition, we plan to promote this guideline by registering on the website of the Korean Association of Internal Medicine and KCHUGR, and to make a booklet consisting of a summary and actively distribute it through future events or symposium of the academic society.
The academic committee and practice guideline committee of the KCHUGR plan to monitor the results of studies in related fields such as H. pylori, atrophic gastritis and intestinal metaplasia, as well as foreign clinical guidelines to be published in the future. If it is judged that it is necessary to add or change the recommendations due to the accumulation of new research results, this guideline can be revised. Periodic review and revision of this guideline will be done every five years.
RECOMMENDATIONS
1. Addition of image-enhanced endoscopic to white light endoscopy may be helpful to increase the diagnostic accuracy of intestinal metaplasia
Six articles were selected as a result of literature search for the efficacy of image-enhanced endoscopy in the diagnosis of intestinal metaplasia and atrophic gastritis (Supplementary Fig. 1).181920212223 Of these, one article was on atrophic gastritis, and five were on intestinal metaplasia. In atrophic gastritis, compared with white light endoscopy, image-enhanced endoscopy improved the sensitivity for the diagnosis, but did not show an improvement in specificity. The sensitivity and specificity of white light endoscopy for the diagnosis of atrophic gastritis were 0.13 (95% confidence interval [CI], 0.04–0.30) and 0.88 (95% CI, 0.72–0.97), respectively, and the sensitivity and specificity of imaging-enhanced endoscopy were 0.96 (95% CI, 0.90–0.99), 0.50 (95% CI, 0.29–0.71), respectively. On the other hand, the sensitivity and specificity of the diagnosis of intestinal epithelial metaplasia of the image-enhanced endoscopy were 0.79 (95% CI, 0.66–0.88) and 0.67 (95% CI, 0.47–0.83), respectively, and the sensitivity of the white light endoscope alone was 0.32 (95% CI, 0.24–0.41) and specificity 0.63 (95% CI, 0.27–0.89). In terms of sensitivity and specificity, image-enhanced endoscopy was superior to white light endoscopy alone (Supplementary Fig. 2). In particular, according to the results of meta-analysis of studies using narrow band image (NBI), the sensitivity of the diagnosis of intestinal metaplasia was 0.78 (95% CI, 0.69–0.89), and the specificity was 0.89 (95% CI, 0.84–0.92) without using magnifying endoscopy. When magnifying endoscopy is used, a light-blue crest in which the brush border of intestinal metaplasia is bright is characteristic. The diagnostic sensitivity and specificity of NBI endoscopy using magnifying endoscopy showed high values of 0.82 (95% CI, 0.67–0.92) and 0.97 (95% CI, 0.92–0.99), respectively.18 Therefore, image-enhanced endoscopy techniques such as NBI are expected to be very helpful in endoscopic diagnosis of intestinal epithelial metaplasia.
In the case of image-enhanced endoscopy, most of them are installed in white light endoscopy equipment, and physicians can simply operate it by pressing a button. Although the examination time may be longer than that of the white light endoscope alone, the difference in procedure time is considered to be insignificant and the benefit is expected to be relatively high as the number of times of biopsy can be reduced. However, in order to diagnose intestinal metaplasia using image-enhanced endoscopy, it is necessary to be familiar with various endoscopic findings and to be properly educated on image-enhanced endoscopy. Since there is no additional separate payment for image-enhanced endoscopy by insurance system, it seems necessary to discuss this issue in the future.
2. When a biopsy is considered to confirm atrophic gastritis or intestinal metaplasia, white light endoscopy findings are insufficient to be used as a basis for determining whether to perform a biopsy
There were a total of six articles comparing the endoscopic findings and pathological examination results in the diagnosis of atrophic gastritis or intestinal metaplasia, and all were cross-sectional studies.242526272829 Of these, three studies were on atrophic gastritis, and three studies on intestinal metaplasia. In the study of atrophic gastritis, the outcome results were obtained separately depending on whether the biopsy site was the antrum or the body, so a statistical analysis was also performed separately (Supplementary Table 2).
In the case of atrophy in antrum, a total of 3,446 patients who underwent endoscopic examination underwent biopsy. Among 3,446 patients, 1,863 patients were diagnosed as positive for atrophy on endoscopic findings, and among them, 1,231 patients were also diagnosed as positive for atrophy in the biopsy, and 632 patients were diagnosed as negative for atrophy. Among 1,582 patients diagnosed as negative for atrophy by endoscopic findings, 884 patients were also diagnosed as negative for atrophy in histological examination, and 698 patients were diagnosed as pathologically proven atrophy. As a result of meta-analysis of three studies, the sensitivity was 0.63 (95% CI, 0.60–0.67), the specificity was 0.58 (95% CI, 0.56–0.61), the positive predictive value was 0.66 (95% CI, 0.64–0.68), and the negative predictive value was 0.56 (95% CI, 0.52–0.60) (Supplementary Fig. 3). In case of atrophy in body, a biopsy was performed in 3,603 out of 4,022 patients who underwent endoscopic examination. Among them, 1,688 patients were diagnosed as positive for atrophy on endoscopic findings, of which 851 patients were also diagnosed as positive for atrophy in the biopsy, and 837 patients were diagnosed as negative in the pathological examination. Among 1,915 patients diagnosed as negative for atrophy by endoscopic findings, 1,413 patients were also diagnosed as negative in biopsy, however, 502 patients were diagnosed as positive. As a result of meta-analysis of three studies, sensitivity, specificity, positive predictive value, and negative predictive value were 0.67 (95% CI, 0.46–0.82), 0.67 (95% CI, 0.48–0.81), 0.58 (95% CI, 0.44–0.70), and 0.74 (95% CI, 0.68–0.80), respectively (Supplementary Fig. 4).
In the case of intestinal metaplasia, biopsy was performed in 1,521 patients who underwent endoscopic examination. Among 1,521 patients, 338 patients were diagnosed as positive for intestinal metaplasia by endoscopic findings. Among these, 274 patients were also diagnosed as positive on histological examination, while 64 patients were diagnosed negatively. Among 1,183 patients diagnosed as negative for intestinal metaplasia by endoscopic findings, 553 were also diagnosed as negative in histological examination and 630 as positive. The result of meta-analysis of three studies are as follows: the sensitivity 0.71 (95% CI, 0.19–0.96), specificity 0.80 (95% CI, 0.49–0.94), positive predictive value 0.79 (95% CI, 0.69–0.87), and negative predictive rate 0.71 (95% CI, 0.39–0.91) (Supplementary Fig. 5). Overall, in the case of diagnosing atrophy or intestinal metaplasia with only endoscopy findings, the accuracy of diagnosis is not high, and the meta-analysis results show that there is a large variation in diagnosis among physicians, considering the high heterogeneity in the meta-analysis. Therefore, it was concluded that it is not recommended to decide whether to perform a biopsy for the diagnosis of atrophy or intestinal metaplasia based on white light endoscopy findings.
Diagnosing atrophic gastritis and intestinal metaplasia is for the purpose of discriminating high-risk groups for gastric cancer. However, in current clinical practice, it is difficult to conduct more than five biopsies for the diagnosis of atrophic gastritis and intestinal metaplasia according to Sydney protocol. Currently, for adults over 40 years of age, regular gastroscopy once every two years is implemented as a national cancer screening program, so a differential screening protocol is not being applied according to the diagnosis of high-risk and low-risk groups. Therefore, pathological confirmation of atrophy and intestinal metaplasia is not an essential requirement, so random biopsy should be performed selectively.
3. Because patients with a high-risk stage (high grade) of atrophic gastritis/intestinal metaplasia have a higher risk of gastric cancer than those with low-risk stage (low grade) patients, different follow-up according to grade can be recommended
Seven cohort studies that followed up the occurrence of gastric cancer by grading atrophic gastritis or intestinal metaplasia were included in this recommendation, including studies included in systematic literature review and meta-analysis published in 2018 by Yue et al. (Supplementary Table 3).3031323334353637 Three studies divided atrophic gastritis and intestinal metaplasia by grade to determine risk of gastric cancer,313637 three studies divided atrophic gastritis into grade,323334 and one study divided intestinal metaplasia by grade to examine the development of gastric cancer.35 In this guideline, for the grade of atrophic gastritis, the Operative Link on Gastritis Assessment (OLGA) classification system proposed by Rugge and Genta38 was used, and for intestinal metaplasia, the Operative Link on Gastric Intestinal Metaplasia Assessment (OLGIM) classification system proposed by Capelle et al.31 was used. The OLGA and OLGIM classification systems were classified into 0, I, II, III, and IV according to the degree of inflammation in the antrum and body using the histological evaluation of the Sydney system. In the Kyoto Global Consensus on H. pylori gastritis (2014), it was suggested to use OLGA or OLGIM system for risk assessment of gastric cancer.3 In this guideline, stages 0, I, and II were classified as low-risk stage, and stages III and IV were classified as high-risk stage (Supplementary Table 4).
Overall, during the follow-up period of 5 to 20 years, 33 (6.5%) out of 510 patients with high-risk OLGA stage developed gastric tumors (gastric cancer or high dysplasia) and 26 (0.3%) of 10,296 patients with low-risk OLGA stage developed gastric tumors. As a result of meta-analysis of six studies, the incidence of gastric tumors was higher in patients with high-risk OLGA stage than in patients with low-risk stage (risk ratio [RR], 28.19; 95% CI, 3.61–220.32) (Supplementary Fig. 6). In addition, during the same period, gastric tumors occurred in 20 (6.2%) of 325 patients with high-risk OLGIM stage and 26 (1.8%) of 1,414 patients with low-risk OLGIM stage. As a result of meta-analysis of the four studies, the incidence of gastric tumor was also higher in high-risk OLGIM stage than those in low-risk stage patients (RR, 4.99; 95% CI, 1.44–17.33) (Supplementary Fig. 7).
In order to use the prognosis that patients with high-risk stage of atrophic gastritis and intestinal metaplasia has a 28-fold or 5-fold higher risk of gastric tumors compared to low-risk stage patients, high-risk stage was defined as the concept of diagnosis to predict the prognosis, that is, “prognostic diagnosis”. The sensitivity, specificity, true positive, true negative, false positive, and false negative of the gastric tumor prediction by a diagnosis of high-risk stage were as follows. Six studies in 10,806 patients with high-risk OLGA stage had a sensitivity of 56% (95% CI: 42%-69%) and a specificity of 96% (95% CI: 95%-96%) for development of gastric tumors (Supplementary Fig. 8). In addition, the sensitivity of high-risk OLGIM stage to gastric tumor development in 1,739 patients in 4 studies was 43% (95% CI: 29%-59%), and the specificity was 82% (95% CI: 80% -84%) (Supplementary Fig. 9).
Therefore, when predicting the risk of gastric tumors by dividing atrophic gastritis and intestinal epithelial metaplasia into risk stages, the sensitivity is not high, but the specificity is high. Close follow-up is necessary for patients with high-risk stage. In addition, follow-up is necessary because gastric cancer may occur even in patients diagnosed with a low-risk stage, but the method and interval of follow-up may vary depending on the risk stage. Although the appropriate interval for endoscopic examination in the high-risk and low-risk group for GCs is controversial, according to a study from Korea, more GCs were found when endoscopy was performed at 1-year intervals than at 2-year intervals in patients with severe intestinal metaplasia.39 In the study of screening endoscopy targeting the general population, endoscopy at 1-year intervals found more early GCs than endoscopy at 2-year intervals.40 However, since these are retrospective studies and do not report outcomes on survival or mortality, further research is needed on this issue.
4. For patients with H. pylori-associated gastritis, eradication is recommended to prevent gastric cancer
The studies included in this recommendation were seven randomized controlled trials comparing the effects of eradication treatment with placebo in patients with H. pylori-associated gastritis (Supplementary Table 5).41424344454647484950 You et al.,42 Ma et al.,43 and Li et al.44 was considered as a single study because the results of follow-up for the same cohort were published at 7.3 years, 14.7 years, and 22 years, respectively. Leung et al.45 and Zhou et al.46 was also considered as a single study, as it was a study in which follow-up results in the same cohort were published for the 5th and 10th years, respectively.
All seven included studies commonly reported the outcome of the incidence of gastric cancer after H. pylori eradication. However, in the study by Leung et al.45 and Zhou et al.,46 the number of registrations in 2014 was smaller than that in 2004, so it can be concluded that there was a number of missing data, but there was no explanation or information about this. Data on mortality were not reported in 2014, but were reported in 2004, so a selective report was suspected, but detailed information was not available. Study by Saito et al.48 was evaluated as high risk of bias because detailed information could not be obtained as an only abstract form submitted to Digestive Disease Week in 2005 and follow-up studies were not published. Study by Correa et al.50 reported data on overall mortality, but did not present data on mortality related to gastric cancer and follow-up loss rate was higher than 25%, but the effect on the study was not explained. It was evaluated as high-risk of bias. The remaining four studies were evaluated as low risk of bias (Supplementary Table 6).414243444749
Overall, during the follow-up period of 5 to 22 years, 68 (1.6%) gastric cancer cases developed in the 4,206 H. pylori eradication group, and 125 (3.0%) gastric cancer cases occurred in the 4,117 control group. As a result of meta-analysis of seven studies, H. pylori eradication lowered the incidence of gastric cancer compared to the control group (RR, 0.54; 95% CI, 0.40–0.72) (Supplementary Fig. 10).
For all-cause mortality, 315 (8.9%) deaths were reported in the 3,551 H. pylori eradication group and 323 (9.2%) deaths in the 3,528 control group during a follow-up period of 6 to 22 years. As a result of meta-analysis of the results of five studies, the eradication did not lower the frequency of all-cause mortality compared to the control group (RR, 0.97; 95% CI, 0.85–1.12) (Supplementary Fig. 11). On the other hand, in the case of gastric cancer-related mortality, 36 (1.1%) deaths were reported in the 3,154 H. pylori eradication group and 59 (1.9%) deaths in the 3,147 control group during the 5 to 22 year follow-up period. As a result of a meta-analysis of the results of four studies, it was calculated that eradication treatment reduced gastric cancer-related mortality (RR, 0.61; 95% CI, 0.40–0.92) (Supplementary Fig. 12).
Taken together, the above results show that H. pylori eradication reduced the incidence of gastric cancer and lowered gastric cancer-related mortality compared to the control group, but did not reduce the overall mortality rate. Therefore, based on these results, it was concluded that eradication is recommended for the prevention of gastric cancer in patients with H. pylori-associated gastritis.
5. Helicobacter eradication can be performed to improve atrophic gastritis in Helicobacter-positive atrophic gastritis patients
In the case of Helicobacter-positive intestinal metaplasia patients, Helicobacter eradication is not recommended only for improvement of intestinal metaplasia.
Titles, abstracts, and original texts were reviewed for a total of 1,924 articles found by hand search and search in domestic and foreign literature databases. Finally, a total of 4 randomized controlled studies were finally selected and the flowchart for selection process was presented in Supplementary Fig. 13.
A study by Sung et al.51 was conducted in asymptomatic volunteers and a study by Kamada et al.52 included dyspepsia patients. Subjects of study by Cho et al.53 were patients who underwent gastrectomy for gastric cancer, and those of study by Arkkila et al.54 were H. pylori-infected peptic ulcer patients. In all four studies, subjects were randomized into two groups: the group using the eradication treatment and the group using the placebo. In addition, initial scores for atrophic gastritis and intestinal metaplasia were assigned according to the updated Sydney classification. The follow-up period was 1 year in studies by Arkkila et al.54 and Sung et al.,51 and was 3 years in studies by Kamada et al.52 and Cho et al.53 (Supplementary Table 7).
As a result of analyzing four randomized control studies,51525354 atrophic gastritis showed improvement in the antrum (mean difference [MD], 0.34; 95% CI, 0.24−0.44; I2 = 95%, P < 0.0001) and body (MD, 0.11; 95% CI, 0.06−0.16; I2 = 0%, P < 0.00001) after H. pylori eradication (Supplementary Fig. 14).
In the case of intestinal metaplasia, the results of analysis of three randomized controlled studies515354 did not show significant improvement of intestinal metaplasia in antrum (MD, 0.04; 95% CI, −0.13–0.21; I2 = 0%, P = 0.65) and body (MD, 0.03; 95% CI, −0.03–0.10; I2 = 0%, P = 0.28) (Supplementary Fig. 15).
Therefore, it could be concluded that, for atrophic gastritis positive for H. pylori, atrophic gastritis can improve after eradication therapy, but in case of intestinal metaplasia, eradication therapy is not recommended for histological improvement only.
6. No recommendation
A literature search was conducted to determine if surveillance endoscopy at intervals shorter than 2 years in patients diagnosed with intestinal metaplasia can reduce gastric cancer mortality. As a result of literature search and selection, there were no randomized controlled or prospective studies that satisfied the inclusion criteria. As a result of retrospectively analyzing the period from the last endoscopy performed before the diagnosis of gastric cancer by conducting a questionnaire on 561 patients diagnosed with gastric cancer in Korea, endoscopy at intervals of 3 years in the group without intestinal metaplasia and at intervals of 2 years in the group with intestinal metaplasia was associated with an improvement of disease-free survival.55 In other words, frequent endoscopy was more likely to detect early gastric cancer in patients with intestinal metaplasia. However, endoscopy with shorter intervals than two years currently recommended by the national cancer screening program did not affect the survival rate of gastric cancer.
The appropriate endoscopic interval in intestinal metaplasia can be determined by considering the local prevalence of intestinal metaplasia, the risk of gastric cancer in the patients with intestinal metaplasia, and the benefits and harms of surveillance endoscopy. In a multicenter study in Korea that evaluated the presence or absence of intestinal metaplasia based on endoscopic findings on patients who underwent health screening, the prevalence of intestinal metaplasia was 12.5% in 2011 and 17.7% in 2016–2017.5657 As a result of a cohort study in which biopsies were performed from the antrum and body by endoscopy, 28.6% of the antrum specimens and 21.2% of the body specimens showed intestinal metaplasia.5 In a study evaluating the presence of intestinal metaplasia by biopsies of 1–4 tissues from antrum, lower body, middle body, and upper body, the age-standardized prevalence of intestinal metaplasia was 26.2% for men and 24.2% for women.58 In another study, the prevalence of intestinal metaplasia in patients with H. pylori infection was 34.4% and 27.9% in antrum and body, respectively, which were significantly higher than patients without H. pylori infection (10.7% and 9.5%, respectively).59 Taken together, the local prevalence of intestinal metaplasia is more than 9.5% and has been reported as high as 34%.5860
Intestinal metaplasia is well known as a precursor lesion of gastric cancer. According to the meta-analysis, the annual risk of progression from intestinal metaplasia to gastric cancer was 0.124%.59616263 In a Korean cohort study, 920 patients who underwent endoscopy for screening or peptic ulcer disease were followed for an average of 9.4 years, and gastric cancer was diagnosed in 5 patients.59
H. pylori infection was confirmed upon entering the cohort in all patients diagnosed with gastric cancer, and intestinal metaplasia was observed in 4 out of 5 patients. The incidence of gastric cancer in patients with intestinal metaplasia was 187.4 per 100,000 person-years, which was 10.9 times higher than 17.2 in patients without intestinal metaplasia, suggesting the need for surveillance.
Few studies investigated whether intestinal metaplasia progresses to gastric cancer in a shorter period of time than patients without intestinal metaplasia. As a result of follow-up of patients diagnosed with intestinal metaplasia in one study, they progressed to dysplasia or gastric cancer after a median 11–32 months, and incomplete intestinal metaplasia progressed to gastric neoplasia within a shorter period.64 In addition, more active surveillance may be considered for a high risk groups such as extensive intestinal metaplasia and a family history of gastric cancer, but domestic research result to support this are lacking.616465
In summary, intestinal metaplasia is associated with an increased risk of gastric cancer and requires appropriate screening and surveillance. However, direct evidence to support the key question of whether endoscopy at intervals shorter than 2 years can reduce gastric cancer mortality in patients with intestinal metaplasia is lacking. Even considering the indirect evidence, there is insufficient evidence to derive an appropriate surveillance endoscopy interval in patients with intestinal metaplasia. Therefore, in this guideline, it was concluded that there was insufficient evidence to recommend or not recommend an endoscopic surveillance at intervals of less than 2 years in patients with intestinal metaplasia.
7. In patients with NSAID-related erosive gastritis, PPI can be considered to improve endoscopic findings
We searched the literature to find the improvement effect of PPI in patients with erosive gastritis, but there was no randomized placebo-controlled study that met the inclusion criteria. Three randomized controlled study comparing PPI with other medication was searched.666768 Two of the three studies were double-blind studies in patients taking NSAIDs with gastric ulcer, duodenal ulcer, or 10 or more erosive gastritis. However, there was no specific description of the randomization method, so it was evaluated as some concern. One study, a comparative study, was evaluated as a high risk of bias because there was no mention of double-blindness or randomization. The characteristics of the three selected studies are summarized in Supplementary Table 8.
All three studies included gastric ulcer, duodenal ulcer, or multiple erosive gastritis. When patients with erosive gastritis were analyzed separately, the healing rate of misoprostol was higher than that of omeprazole at 8 weeks (misoprostol 87% vs. 20 mg omeprazole 77%, P < 0.001 and vs. 40 mg omeprazole 79%, P = 0.01).66 On the other hand, the healing rate was higher with omeprazole compared to ranitidine at 8 weeks (ranitidine 77% vs. 20 mg omeprazole 89%, P = 0.008 and vs. 40 mg omeprazole, 86%, P = 0.19).67 In a small Russian study, 4 and 6 patients in the omeprazole and misoprostol group had multiple erosive gastritis, respectively, and they all healed in both groups after 2 weeks of treatment.68 In this study, the number of patients with erosion was very small and there was no specific description of the study design, so it was excluded from the final meta-analysis.
There were no studies comparing the effects of PPI (omeprazole) with placebo on the endoscopic healing of erosive gastritis, but there were randomized controlled studies comparing the effects of H2 blocker (ranitidine) or misoprostol. A single arm meta-analysis was performed on the effects of PPI in these two studies (Supplementary Fig. 16). When omeprazole 20 mg was administered for 4 weeks, erosive gastritis improved by 68%, and when administered for 8 weeks, 83% improved. When omeprazole 40 mg was administered for 4 weeks, erosive gastritis improved by 67%, and after 8 weeks, 83% improved. Since there is little difference in the healing effects of 20 mg and 40 mg of omeprazole, omeprazole 20 mg can be used to treat erosive gastritis.
There was no placebo-controlled study that separately analyzed erosive gastritis, but in the OMNIUM study, the healing effect of omeprazole 20 mg at follow-up up to 26 weeks was significantly superior to that of the placebo group (P < 0.001) and the misoprostol group (P = 0.001) in the treatment of ulcers and multiple erosive gastritis.64 A randomized controlled study was searched for PPIs on improvement of erosive gastritis, but published randomized controlled studies have only described NSAID-related erosive gastritis. It is worth waiting for the results of the ongoing study for the effect of PPI on erosive gastritis.
8. In patients with erosive gastritis, it is not recommended to use a mucoprotective agent solely for the purpose of improving the erosions
Since gastric acid plays an important role in the development of gastric mucosal erosions, acid suppression therapies such as histamine-2 receptor antagonist (H2RA) are effective in healing of erosions and improving related symptoms and are recommended in many guidelines.67 However, as mentioned in the introduction, this guideline mainly dealt with controversial topics related to gastritis, so separate recommendations for H2RA were not made in this version of guideline.
Five randomized controlled trials comparing the effects of mucosal protective agents with placebo in patients with erosive gastritis were found (Supplementary Table 9).6970717273 Breaking down the results of these studies, there were three studies showing improvement in gastritis, one study showing improvement in atrophic gastritis, two studies showing improvement in intestinal metaplasia, and 2 studies examining the effect of dyspepsia symptoms. In addition, there were five randomized controlled studies comparing mucoprotective agents with H2RAs,7475767778 and there were 9 comparative studies comparing the effects between mucosal protective agents.798081828384858687 The characteristics of these studies were summarized in Supplementary Tables 10 and 11, respectively.
Out of five randomized controlled trials compared to placebo, there was only one study that showed improvement in endoscopic erosion.69 After administering sucralfate and placebo to 35 patients each for 6 weeks, endoscopic gastritis and erosion were observed. There was no significant difference between the two groups, as 43% of the sucralfate group showed improvement and 37% of the placebo group showed improvement. Among the comparative studies with placebo, there was only one study that showed improvement in endoscopic erosion and gastritis, and there was no significant difference between the two groups. So, in studies comparing mucoprotective agents and H2RAs and studies comparing mucoprotective agents, the healing rate and improvement rate of mucoprotective agents was pooled and compared with those of placebo group. The erosion healing rate of the placebo group was 37.1% (95% CI, 21.2–53.2), and that of the mucoprotective group was 45.3% (95% CI, 35.9–54.7), and there was no statistically significant difference between the two groups (Supplementary Fig. 17). The improvement rate of erosion was 57.1% (95% CI, 40.7–100.0) in the placebo group and 60.6% (95% CI, 50.0–71.2) in the mucoprotective group, and there was also no significant difference (Supplementary Fig. 18).
There were three studies on the improvement of atrophic gastritis or intestinal metaplasia after long-term use of mucoprotective agents for 6 months to 1 year. Atrophic gastritis was more progressive in the mucoprotective agent group (Supplementary Fig. 19), and intestinal metaplasia was not different between mucoprotective agent group and placebo group (Supplementary Fig. 20).
According to the results of two studies that reported the adverse events in the mucoprotective agent and placebo groups, there were no adverse events and serious adverse events in both groups.6869 All of these studies are relatively short-term studies with a study period of 4 or 6 weeks. Therefore, the relatively short-term use of mucoprotective agents is not considered to cause serious adverse events. Looking at the results of benefits, the use of mucoprotective agents did not have a significant effect compared to placebo on the improvement of endoscopic erosions, atrophic gastritis and intestinal metaplasia. Therefore, it is not recommended to administer mucoprotective agents for the relief of gastritis or erosions.
CONCLUSIONS
Gastritis is a very common disease in Korea. Proper diagnosis and treatment for atrophic gastritis and intestinal metaplasia, appropriate surveillance for pre-neoplastic lesions, and eradication of H. pylori play a very important role in the prevention and early diagnosis of gastric cancer. Therefore, considering the high incidence of gastric cancer in Korea, it is very important to publish guidelines for gastritis and related diseases, which are commonly seen in clinical practice. In addition, since the management for gastritis differs in each country, the recommendations were prepared by reflecting the current situation of Korea as much as possible. This is expected to be helpful to many clinician who care the patients with gastritis and gastrointestinal diseases.
This time, while making a guideline, we tried to make an evidence-based recommendation through a systematic review and meta-analysis, but the relevant evidence was not sufficient. Therefore, it was not possible to cover all the contents of gastritis, and only clinically important topics were covered in this guideline. In the future, many studies on diagnosis, treatment, and follow-up of many gastritis patients in Korea should be conducted, and we hope that treatment recommendations can be made based on local evidence.
 XML Download
XML Download