

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
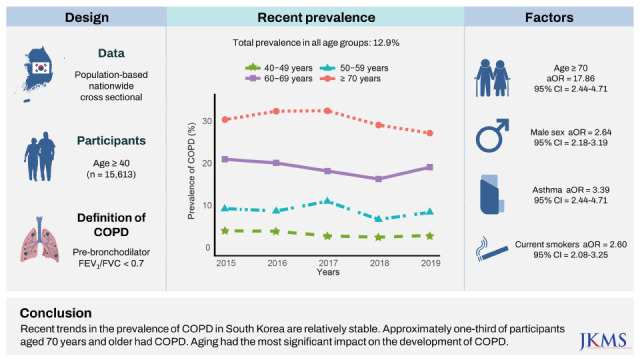
As a common chronic respiratory disease, chronic obstructive pulmonary disease (COPD) causes huge socioeconomic burdens worldwide.1 Considering global aging trends and the fact that advanced age is a significant risk factor for the development of COPD, the burden is expected to be more substantial in aged societies. Consequently, in aged societies, it is important to establish health service plans to alleviate the burden of COPD.2 To effectively plan health services, information on the prevalence of and potentially preventable factors associated with the disease should be thoroughly investigated.3
In rapidly aging societies, demographics and socioeconomics related to COPD can also change rapidly. For example, in Korea, a very rapidly aging society,4 the smoking rate has recently decreased in men and remained the same in women,5 and the prevalence of tuberculosis has decreased,6 among factors related to the prevalence of COPD.7 Thus, to accurately evaluate the prevalence of and factors associated with COPD, representative nationwide data reflecting factors associated with COPD are essential. However, few rapidly aging or aged societies have such nationwide representative databases. Fortunately, Korea does collect nationally representative data via the Korea National Health and Nutrition Examination Survey (NHANES), including pulmonary function measurements. The prevalence of COPD in Korea was 17.2% in 2002,8 higher than in Western countries. The prevalence of COPD decreased in the early 2010s from the early 2000s, but has not significantly changed from the 2010s until 2015.8910111213
With the rapid aging of the Korean population, a recent update on COPD prevalence in Korea is needed. Therefore, in this study, we investigate recent trends of and factors related to COPD in Korea, a rapidly aging country expected to be a super-aged country by 2025,14 using a nationwide database from 2015 to 2019.
METHODS
Study population
The Korea NHANES is a population-based nationwide survey to investigate the health and nutritional status of the civilian, non-institutionalized population of Korea, and has been conducted periodically since 1998. The Korea NHANES is performed using a multistage, stratified probability sampling method to represent the entire Korean population. In this study, we used Korea NHANES data from 2015 to 2019. Since lung function tests were performed for individuals aged 40 years or older in each survey, those aged less than 40 years were excluded. More detailed information on the Korea NHANES is provided in previous studies.15
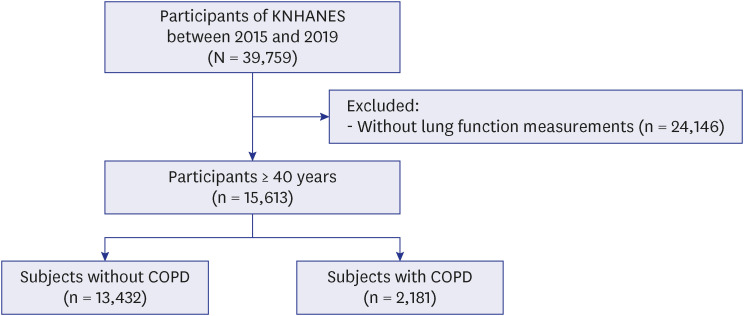
A flow chart of the selection of the study population is presented in Fig. 1. Among 39,759 participants, we excluded 24,146 participants without lung function measurements. Finally, 15,613 participants (13,432 participants without COPD and 2,181 participants with COPD) were included in the analysis.
Definition of COPD
COPD was defined as pre-bronchodilator value of forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 0.7. Lung function was measured by well-trained technicians using a spirometer (Vyntus Spiro; Care Fusion, San Diego, CA, USA; or dry rolling seal spirometer Model 2130; Sensormedics Corporation, Yorba Linda, CA, USA) according to the American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines.16
Measurements and other definitions
Income was assessed using monthly household income. Regular walking was defined as walking at least five times a week for ≥ 30 minutes at a time. Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or receiving antihypertensive medications. Dyslipidemia was defined as low-density lipoprotein cholesterol level ≥ 130 mg/dL, high-density lipoprotein cholesterol level ≤ 40 mg/dL, or receiving lipid-lowering medications. Diabetes mellitus was defined as a fasting plasma glucose level ≥ 126 mg/dL or receiving glucose-lowering medications. Symptoms, physical limitations, and other comorbidities (asthma, a history of pulmonary tuberculosis, allergic rhinitis, and cardiovascular disease) were assessed by self-questionnaire.17
Statistical analyses
Data were expressed as weight percentages with standard errors. Differences between participants with and without COPD were assessed using Pearson’s χ2 test. Multivariable logistic regression analysis was used to determine factors associated with COPD. The variables used for adjustment were selected considering clinical relevance and correlations between variables (Supplementary Table 1). In the final model, sociodemographic variables (age and sex), anthropometric measurement (body mass index [BMI]), personal habits (smoking status), income, performance status (physical limitation), lung function (FEV1%pred), and comorbidities (asthma and history of pulmonary tuberculosis) were included. Although the proportion of low BMI (< 18.5 kg/m2) was relatively small, we included this population in a multivariable model based on the significant effect of low BMI on COPD.1819
In all analyses, sample weights were assigned using the ‘survey’ package of R, and data for participants in the single primary survey unit were centered at the grand mean instead of the stratum mean. The missing indicator method was used to analyze missing values by grouping missing values into another category (missing category). All analyses were performed using R version 4.1.2 (R core Team 2021; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This study was conducted following the guidelines of the Declaration of Helsinki, and the Institutional Review Board (IRB) of the Korea Disease Control and Prevention Agency (KDCPA) approved the protocol (IRB No. 2018-01-03-P-A, 2018-01-03-C-A). Written informed consent was obtained from all Korea NHANES participants, and all data were anonymized before being provided.
RESULTS
Baseline characteristics
Table 1 depicts the baseline characteristics of study participants according to the presence or absence of COPD. Participants with COPD were more likely to be older (39.0% vs. 13.2% ≥ 70 years, P < 0.001), male (74.2% vs 44.4%, P < 0.001), current or ex-smokers (67.9% vs. 39.3%, P < 0.001), and had lower BMI (2.3% vs. 1.7% for BMI < 18.5 kg/m2, P < 0.001) than those without COPD. The proportions of low income (26.6% vs. 22.5% for Q1, P < 0.001) and low education level (33.8% vs. 18.1% for elementary school graduate, P < 0.001) were higher in participants with COPD than in those without COPD. However, participants with COPD had more respiratory symptoms (10.1% vs. 4.8%, P < 0.001) and less regular walking (37.3% vs. 38.1%, P = 0.006) than those without COPD. Regarding lung function, compared to participants without COPD, participants with COPD had a higher FVC (3.54 L vs. 3.46 L, P = 0.001), but lower FVC %-pred (87.5% vs. 90.6%, P < 0.001). FEV1 (2.26 L vs. 2.74 L, P < 0.001), FEV1%-pred (76.5% vs. 91.6%, P < 0.001), and FEV1/FVC (63.6% vs. 79.1%, P < 0.001) were also lower in participants with COPD than in those without COPD. All comorbidities were more prevalent in participants with COPD than in those without COPD, except allergic rhinitis.
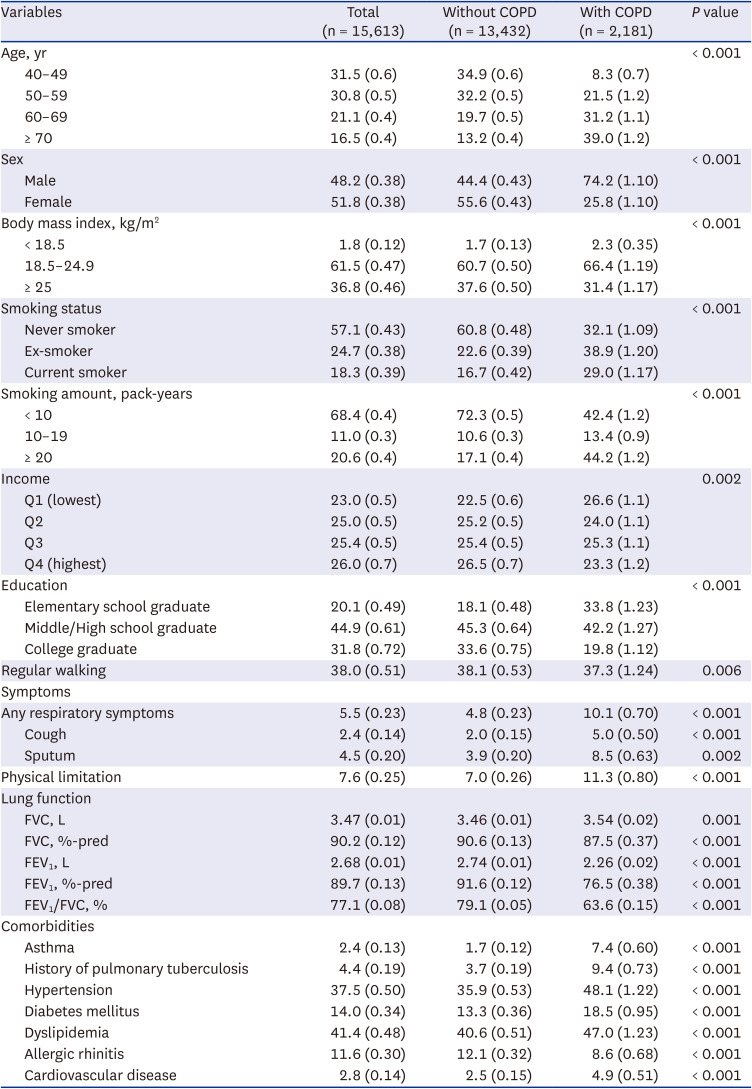
Table 1
Baseline characteristics of the study population
Data are expressed as weighted percentages (standard errors).
COPD = chronic obstructive pulmonary disease, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second.
![]()
Prevalence and yearly trends of COPD
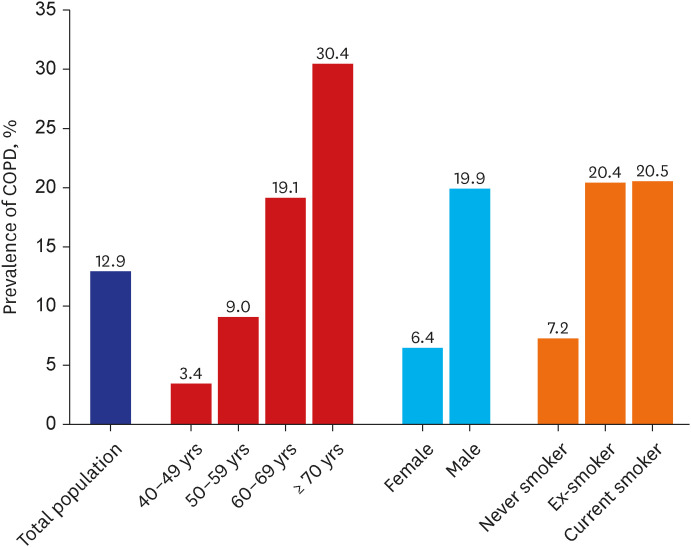
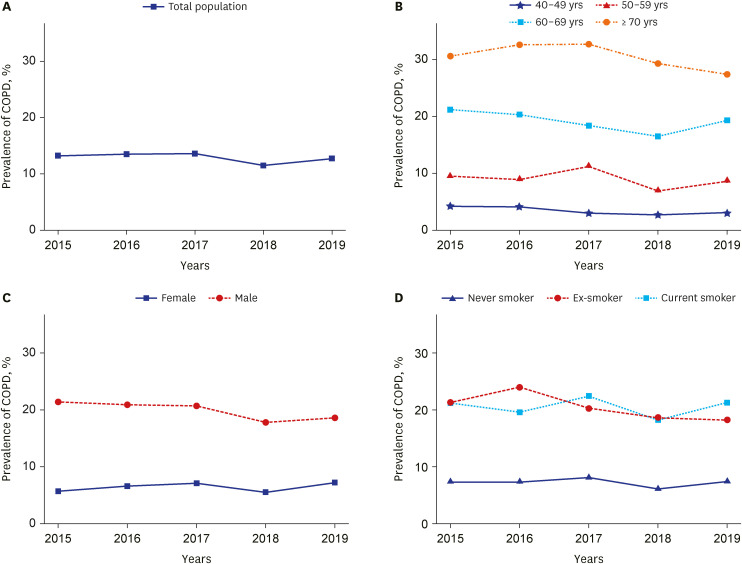
Over the last five years, the prevalence of COPD in Korea was 12.9%. In an analysis stratified for age, sex, and smoking status, the prevalence of COPD was higher in the elderly, males, and current or ex-smokers compared to younger individuals, females, and never-smokers, respectively (Fig. 2).
During the study period, the prevalence of COPD was relatively stable, ranging from 11.5% to 13.6% (Fig. 3). The prevalence of COPD in participants ≥ 70 years increased from 30.6% in 2015 to 32.6% in 2017 and then decreased, showing the lowest prevalence of 27.4% in 2019. Among those in their 60s, it continued to decrease to 16.5% in 2018, then increased to 19.3% in 2019. The prevalence of COPD in their 50s fluctuated from 6.9% to 11.2%. In their 40s, it was constant and low at 2.7–4.2%. The prevalence of COPD in men decreased, while that in women increased, narrowing the gender gap from 15.7% in 2015 to 11.4% in 2019. The prevalence of COPD among ex-smokers was the highest at 24.0% in 2016, but decreased to 18.2% in 2019. Meanwhile, the prevalence of COPD in current smokers fluctuated from 18.2% to 22.4%. A steadily lower prevalence was observed in never smokers, ranging from 6.1% to 8.1%.
Factors associated with COPD
In the multivariable analysis, age 70 years or older was the most significant factor associated with COPD (adjusted odds ratio [aOR], 17.86; 95% confidence interval [CI], 14.16–22.52; P < 0.001; compared with age 40–49) (Table 2). In addition, male sex (aOR, 2.64; 95% CI, 2.18–3.19; P < 0.001), ex-smoker (aOR, 1.59; 95% CI, 1.29–1.94; P < 0.001), current smoker (aOR, 2.60; 95% CI, 2.08–3.25; P < 0.001), low income (Q1) (aOR, 1.35; 95% CI, 1.11–1.65; P = 0.003; compared with the highest income [Q4]), asthma (aOR, 3.39; 95% CI, 2.44–4.71; P < 0.001), history of pulmonary tuberculosis (aOR, 1.40; 95% CI, 1.09–1.81; P = 0.009), and decreased FEV1%pred (aOR, 2.43; 95% CI, 2.28–2.59; P < 0.001 for 10% decrease) showed a significant association with COPD. On the other hand, BMI ≥ 25 kg/m2 (aOR, 0.62; 95% CI, 0.54–0.71; P < 0.001; compared with BMI 18.5–24.9 kg/m2) had an inverse association with COPD.
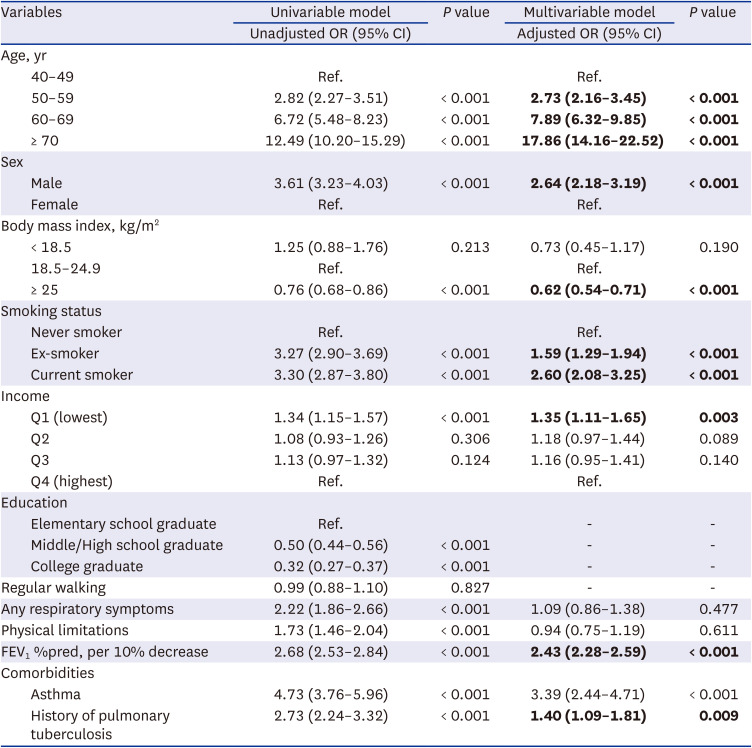
Table 2
Factors associated with chronic obstructive pulmonary disease
Bold font indicates significance in the multivariable analysis.
OR = odds ratio, CI = confidence interval, FEV1 = forced expiratory volume in 1 second.
![]()
DISCUSSION
In this study, we evaluated recent trends of and factors associated with COPD using representative nationwide survey data from Korea between 2015 and 2019. During the study period, the prevalence of COPD was approximately 13% and showed a fairly constant trend. Approximately one-third of participants over age 70 had COPD. COPD-related factors included age, male sex, smoking status, income, BMI, asthma, and history of pulmonary tuberculosis. Of these factors, old age (≥ 70 years) was most strongly associated with COPD.
The main finding of our study was that aging is the most strong factor associated with COPD. Although smoking has been regarded as the most potent etiologic driver of COPD,1 from an epidemiological perspective, the relationship between smoking and the development of COPD may not be as strong as previously believed. Since prevalence is calculated based on the entire population, cumulative effects should be considered to determine the impact of each factor.20 In this context, aging may have a more negligible effect per unit increase on the development of COPD than smoking, but the cumulative effect of aging could be significant. Therefore, it is required to examine the possibility of underestimating the effect of aging on the prevalence of COPD, especially in rapidly aging societies.
As with other organs, it is natural that lung function declines with age. There have been studies that aging-related oxidative stress affects the genesis of COPD.21 An excess of reactive oxygen species, a product of oxygen metabolism, may cause age-dependent molecular damage and induces chronic inflammation, which is associated with various chronic diseases, including COPD.22 Although the exact mechanism by which aging affects COPD development has not yet been established, genetic analysis may provide clues for this issue. For example, Zhong et al.23 showed that some age-related genes were upregulated in clinical COPD samples, suggesting a possible link between aging and COPD progression. Studies also have found that telomeres, a biomarker of aging, are shorter in the lung and in the peripheral blood obtained from COPD patients compared with age-matched healthy smoking and nonsmoking controls.2425262728 Further studies should be directed at determining how this link could be used in clinical practice.
The World Health Organization and United Nations define an aged society as one in which the proportion of people aged 65 or over exceeds 14% of the overall population.29 The world is aging rapidly, and by 2030 there will be tens of millions of people aged 65 and over.30 In 2019, 20 countries (2 North American countries, 3 Asia-Pacific countries, and 15 Europe countries) were recorded as aged societies.31 In the most populous of those countries, the proportion of elderly people (≥ 65 years) and the prevalence of COPD ranged from 16.0% to 28.2% and 6.4% to 25.0%, respectively (Supplementary Table 2).323334 South Korea, which became an aging society in 2017, is experiencing rapid aging.35 The prevalence of COPD in Korea was similar to those in the previously mentioned countries. Notably, among Koreans 60–69 years and over 70 years, there were no significant changes in the prevalence of COPD over time. However, with the rapid increase of the elderly population, the absolute number of elderly patients with COPD is increasing. Therefore, demographic changes should be considered when investigating trends of COPD prevalence.
COPD is heterogeneous.3637 In the recently updated Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the first COPD phenotype including an age criterion has emerged: “COPD in young people.”38 Although this is a concept more focused on the prevention of COPD, there may be other age-associated COPD phenotypes, the recognition of which could lead to better management. In this study, we discovered significantly increased odds ratio for COPD in those over 70 years compared with those aged 40–49 years, indicating the presence of a geriatric phenotype. Unlike the young population, elderly people have many comorbidities, usually take many prescription drugs, and their metabolism is slow.3940
In addition, compared to young patients, the symptom burden, healthcare utilization, and mortality risk are higher in elderly patients with COPD.4142 Another problem is that they are often unable to properly communicate with their caregivers.43 Regarding treatment, poor inhaler technique is also an important issue in elderly patients; studies have shown that there is a negative correlation between advancing age and appropriate inhaler technique regardless of inhaler type.44 Therefore, constant efforts are needed to overcome those fragile aspects of geriatric phenotype and future studies are also needed regarding this topic.
Another important finding is that the prevalence of COPD decreased in men, whereas it gradually increased in women over time. Although the overall smoking rate in Korea is decreasing, most of the decrease is in men, and the smoking rate of women has not changed until recent years.45 It is suggested that smoking may have a greater impact on women in terms of smoking-related morbidity and mortality than men.46 In Asia, men accounted for most smokers, but the number of female smokers has been steadily increasing in some countries.47 Therefore, more attention is needed to the development of COPD in women in these countries.
A recent systematic review found that previous pulmonary tuberculosis is a risk factor for COPD.48 Our study also showed that a history of pulmonary tuberculosis is associated with COPD. Pulmonary tuberculosis is considered a curable disease, but low-income countries still struggle to fight tuberculosis.49 The burden of tuberculosis has been reduced due to the consistent efforts of the World Health Organization (WHO) to eradicate tuberculosis and the increased investment in tuberculosis management in each country.50 However, the risk of COPD remains high even after pulmonary tuberculosis is successfully treated. Clinicians should pay more attention to manage tuberculosis sequelae, especially COPD, beyond biological treatment.
Moreover, this study identified factors previously known to be associated with COPD: a positive association with low income,51 male sex,52 low FEV1
53
, and low BMI.54 Since COPD is associated with various factors other than smoking, the need to identify risk factors for COPD is important. In line with this concept, a recently released GOLD suggested a new taxonomy, etiotypes for COPD considering the etiology of COPD (genetic, early-life events, environmental exposure, infection, asthma, etc.), to facilitate future research on this topic.1 As part of this effort, future studies are needed to identify the prevalence and burden of each etiotype for COPD in Korean population.
This study has some limitations. First, we used pre-bronchodilator lung function measurements to define COPD since the post-bronchodilator test was not performed in the Korea NHANES. This could lead to an overestimation of COPD prevalence. However, several high-quality papers used pre-bronchodilator measurements in COPD studies.5556 Second, the high prevalence of COPD in the elderly population may be due to the criteria for COPD used in our study.3233 It is well known that a fixed rate (FEV1/FVC < 70%) causes false-positive recognition of COPD with increasing age.57 However, the COPD guidelines still favor using a fixed ratio regardless of age.38 Third, there may be measurement bias because questionnaires were used to assess some variables which could lead to false recalls. Fourth, the spirometer was changed during the study period (June 2016), and there was a difference in sensitivity between the two machines. However, KDCPA performed quality control and adjustment to minimize possible differences. Fourth, to understand the effect of age on COPD clearly, it is necessary to investigate whether age is related to the incidence of COPD, not prevalence of COPD. However, since the Korea NHANES provides only cross-sectional data, we could not evaluate the incidence of COPD. Thus, the causal relationship between age and COPD is uncertain. Future studies based on prospective data will be required to solve this issue. Finally, some important contributing factors to the development of COPD, such as air pollution and history of biomass fuel exposure, were not included.
In conclusion, the recent prevalence of COPD was similar to past years, and approximately one-third of our sample aged over 70 years had COPD. The most strong factor associated with COPD was aging. Therefore, as the absolute number of COPD patients increases with the aging of the population, continuous attention is required to optimize the treatment and management of these patients.
 XML Download
XML Download