

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has enormously affected all spheres of human life and activity. As of September 28, 2022, 621,342,894 COVID-19 cases have been registered worldwide, with a death toll of 6,543,203.1 The USA leads the ranking of countries with the highest number of cases, followed by India and France.1 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has emerged as the most dreadful cytokine-mediated complication of the disease, contributing to high mortality and requiring powerful anti-cytokine therapies.
Rapid spread of the novel coronavirus and its continuing mutation activity have led to the emergence of new virus strains, requiring new approaches to COVID-19 vaccinations and therapies.2 The complexity of the novel coronavirus and systemic manifestations of the infection have all been reflected in diverse fundamental and clinical research directions.3 The deluge of COVID-19 reports and uncontrolled flow of related public discussions on open communication channels have created a new challenge for the global community–misinformation.4
One of the most debated and variably interpreted topics relates to comorbidities which confound COVID-19 course and exaggerate healthcare burden in the pandemic.5 Subjects with chronic comorbid conditions and exhausted immune responses are often more severely affected by the novel coronavirus than those without the burden of background clinical conditions.6 Despite the availability of numerous reports on comorbidities in COVID-19, questions of combined therapies, continuing clinical monitoring, and prevention of associated complications still remain unanswered.789
This bibliometric study is a snapshot Scopus-based analysis that aims to map publication activity and research directions in the field of COVID-19 and comorbidities. This is an attempt to explore scientific facts and perspectives on pathogenesis, clinical course, and outcomes of COVID-19 in subjects with the burden of common chronic background diseases.
METHODS
Searches through the Scopus database were employed on September 24, 2022 in line with previously published recommendations on comprehensive literature coverage.10 The following Medical Subject Heading (MeSH) keywords were used to retrieve and analyze tagged titles, abstracts, and keywords: “diabetes mellitus,” “cardiovascular diseases,” “rheumatic diseases,” “obesity,” “malignancies,” and “COVID-19.”
We used the Scopus database as the largest platform of peer-reviewed literature. Its user-friendly analytical tools allow visualizing the scientific context of big data.11 In the current study, the retrieved records were analyzed in view of their document type, authorship, source, citations, scientific area, country of origin, and indexed keywords. We retrieved and analyzed English only articles, most of which are openly accessible. All retrieved original articles, reviews, case reports, case series, letters, editorials, notes, errata on COVID-19 and accompanying pathologies and reports of pathogenic links between SARS-CoV-2 infection and other pathologies were covered. Conference papers, short surveys, and book chapters were excluded from analyses.
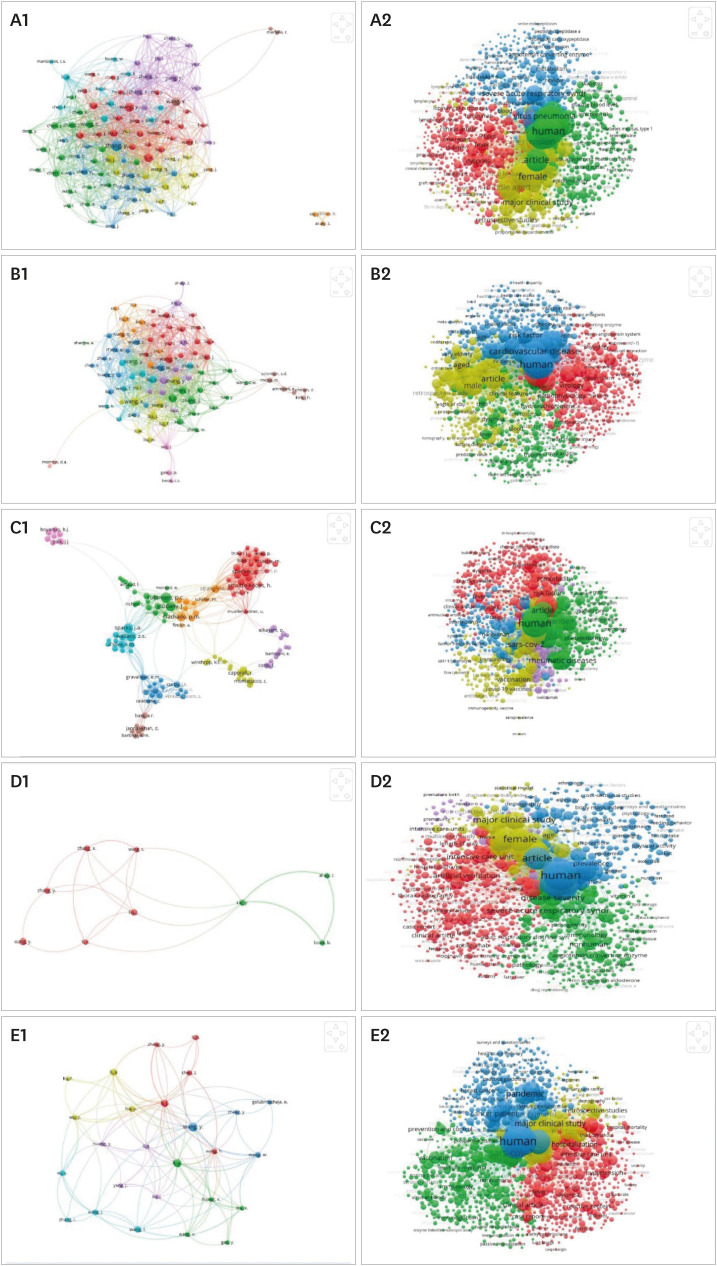
Currently available network visualization tools are widely used to reveal the most active (hot) topics in established and emerging scientific directions. As such, we have explored keywords and authors co-occurrence using the VOSviewer software (version 1.6.18). Related visualizations are depicted in Fig. 1. Nodes represent authors or keywords while lines convey interaction between them. Node size expresses the frequency of occurrence. Coloring helps to distinguish separate groups with stronger or weaker interactions. To make conceptualization more concise and transparent, we used a limited number of keywords and authors to convey the most representative ones (the minimum number for keyword occurrence is set at 10 and for authors occurrence—at 5).
Fig. 1
Depiction of interplay between COVID-19 and comorbid diseases. (A-E) Visualization of authors' network (1) and keywords' network (2) in COVID-19 and DM (A1, A2), COVID-19 and CVD (B1, B2), COVID-19 and RD (C1, C2), COVID-19 and obesity (D1, D2), and COVID-19 and malignancies.
COVID-19 = coronavirus disease 2019, DM = diabetes mellitus, CVD = cardiovascular disease, RD = rheumatic disease.
RESULTS
COVID-19 and diabetes mellitus (DM)
Top 5 journals in the field of COVID-19 and Diabetes Mellitus were Diabetes Metab Syndr Clin Res Rev (n = 203), PLOS One (n = 200), Diabetes Res Clin Pract (n =165), J Clin Med (n = 152), and J Med Virol (n = 129).
Top 5 countries with high publication activity were the USA (n = 3,005), the UK (n = 1,152), India (n = 1,110), Italy (n = 1,108), and China (n = 1,036).
Original articles (n = 8,247, 70.7%) were the most common documents followed by reviews (13.1%), letters (10.1%), notes (3.5%), editorials (2.5%), and errata (0.1%).
Top 5 authors in this field were the following scholars: Khunti, K (n = 45), Misra, A (n = 39), Pal, R (n = 27), Pranata, R (n = 26), and Cariou, B (n = 19).
The co-occurrence keywords network visualization map in COVID-19 and DM was presented in Fig. 1 A2 and can be summarized into categories representing 4 research scopes. The most frequently seen keywords are following: “Human” (n = 13,665), “Coronavirus Disease 2019” (n = 12,475), “COVID-19” (n = 11,299), “Diabetes Mellitus” (n = 10,555), “Humans” (n = 9,411), “Article” (n = 9,121), Male (n = 8,604), Female (n = 8,513), “Adult” (n = 8,081), and “Hypertension” (n = 7,290).
COVID-19 and cardiovascular diseases (CVDs)
Top 5 journals in the field of COVID-19 and CVDs were J Clin Med (n = 134), Int J Environ Res Public Health (n = 114), PLOS One (n = 107), Front Immunol (n = 99), and Eur Heart J (n = 80).
Top 5 countries were the USA (n = 2,626), Italy (n = 1,308), the UK (n = 1,015), China (n = 875), and India (n = 582).
Original articles (58.5%) were the most frequent documents followed by reviews (25.7%), letters (8%), editorials (4.3%), notes (3.3%), and errata (0.2%).
Top 5 authors in this field were Harky, A (n = 22), Banerjee, A (n = 20), Khunti, K (n = 19), Metra, M (n = 19), and Lavie, C (n = 18).
The co-occurrence keywords network visualization map in COVID-19 and CVDs were presented in Fig. 1 B2 and can be summarized into 4 clusters with different colors (red, green, blue, and yellow).
The most frequently seen keywords are the following: “Human” (n = 3,152), “Coronavirus Disease 2019” (n = 12,475), “COVID-19” (n = 3,035), “Coronavirus Disease 2019” (n = 2,573), “Humans” (n = 2,151), “Article” (n = 1,858), “Cardiovascular Disease” (n = 1,693), “Male” (n = 1,645), “Female” (n = 1,604), “Adult” (n = 1,476), “SARS-CoV-2” (n = 1,472), and “Major Clinical Study” (n = 1,052).
COVID-19 and rheumatic diseases (RDs)
Top 5 journals in the field of COVID-19 and RDs were Ann Rheum Dis (n = 157), Rheumatol Int (n = 61), Clin Rheumatol (n = 57), Lancet Rheumatol (n = 53), and RMD Open (n = 32).
Top 5 countries were the USA (n = 288), Italy (n = 190), the UK (n = 158), Germany (n = 110), and France (n = 99).
Original articles were the most frequent documents (n = 648, 55.3%) followed by reviews (18.9%), letters (16.5%), notes (4.9%), editorials (3.4%), and errata (1%).
Top 5 authors were Robinson, PC (n = 37), Wallace, ZC (n = 33), Sparks, JA (n = 33), Yazdany, J (n = 33), and Schulze-Koops, H (n = 24).
The co-occurrence keywords network visualization map in COVID-19 and RDs were presented in Fig. 1 C2 and can be summarized into 5 clusters with different colors (red, green, blue, yellow, and violet).
The most frequently seen keywords are the following: “Human” (n = 494), “COVID-19” (n = 459), “Coronavirus Disease 2019” (n = 384), “Rheumatic Disease” (n = 354), “Humans” (n = 351), “Female” (n = 305), “Article” (n = 289), “Male” (n = 285), “Adult” (n = 276), and “SARS-CoV-2” (n = 255).
COVID-19 and obesity
Top 5 journals in the field of COVID-19 and obesity were Nutrients (n = 137), Int J Environ Res Public Health (n = 113), PLOS One (n = 110), Obesity (n = 95), and Obes Surg (n = 94).
Top 5 countries were the USA (n = 2,151), Italy (n = 761), the UK (n = 714), Spain (n = 445), and France (n = 403).
Original articles were the most frequent documents (n = 4,445, 67%) followed by reviews (17%), letters (9.3%), notes (3.3%), editorials (3%), and errata (0.4%).
Top 5 authors in this field were Khunti, K (n = 19), Lavie, CJ (n = 17), Mahawar, K (n = 14), Arena, R (n = 13), Giustina, A (n = 13).
The co-occurrence keywords network visualization map in COVID-19 and obesity were presented in Fig. 1 D2 and can be summarized into 5 clusters with different colors (red, green, blue, yellow, and violet).
The most frequently seen keywords are the following: “Human” (n = 2,541), “COVID-19” (n = 2,468), “Obesity” (n = 2,246), “Coronavirus Disease 2019” (n = 2,067), “Humans” (n = 1,806), “Article” (n = 1,667), “Female” (n = 1,621), “Male” (n = 1,537), “Adult” (n = 1,481), and “SARS-CoV-2” (n = 1,293).
COVID-19 and malignancies
Top 5 journals in the field of COVID-19 and malignancies were Cancers (n = 29), Front Oncol (n = 29), Br J Haematol (n = 26), Eur J Cancer (n = 25), and Cancer Cell (n = 20).
Top 5 countries were the USA (n = 468), Italy (n = 221), the UK (n = 181), India (n = 127), and China (n = 111).
Original articles were the most frequent documents (70.8%) followed by reviews (17.2%), letters (8.4%), notes (2.2%), editorials (1.2%), and errata (0.2%).
Top 5 authors were Halmos, B (n = 12), Van Hemelrijck, M (n = 12), Bruna, R (n = 11), Corradini, P (n = 11), and Passamonti, F (n = 11).
The co-occurrence keywords network visualization map in COVID-19 and malignancies were presented in Fig. 1 E2 and can be summarized into 5 clusters with different colors (red, green, blue, yellow, and violet).
The most frequently seen keywords are the following: “Human” (n = 719), “COVID-19” (n = 692), “Coronavirus Disease 2019” (n = 599), “Humans” (n = 536), “Article” (n = 465), “SARS-CoV-2” (n = 426), “Female” (n = 416), “Male” (n = 406), “Adult” (n = 389), and “Hematologic Malignancy” (n = 319).
DISCUSSION
Patients with chronic health conditions comprise a vulnerable group for adverse clinical outcomes in SARS-CoV-2 infection.8 A retrospective, multicenter cohort study (n = 191) reported that about 48% of COVID-19 patients had comorbidities, including arterial hypertension (n = 58, 3%), DM (n = 36, 2%), and coronary heart diseases (CHDs) (n = 15, 8%).9 COVID-19 seems to be more frequent among older men with accompanying diseases, resulting in complicated or fatal outcomes.12
Examining the influence of comorbidities on the course and consequences of COVID-19 is crucially important.
Knowledge of pathogenic mechanisms of SARS-CoV-2 infection in subjects with comorbid pathologies would be helpful for risk stratification, organization of health services, and personalization of the services.
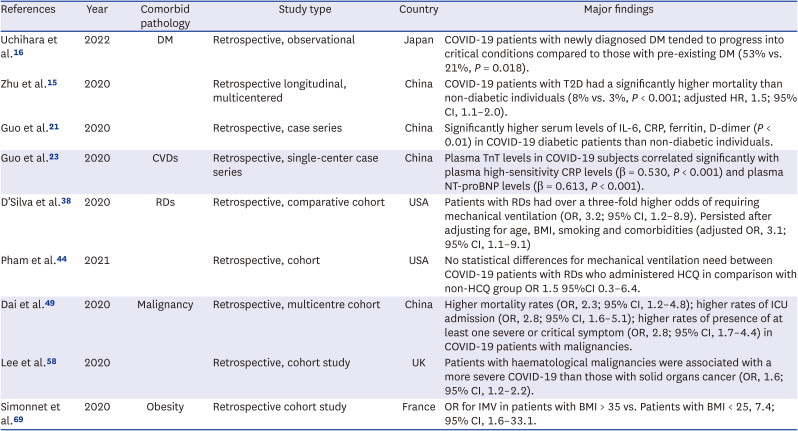
The most common clinical findings typically encountered in COVID patients with comorbidities are shown in Table 1.
Table 1
Peculiarities of comorbidities in COVID-19
| References | Year | Comorbid pathology | Study type | Country | Major findings |
|---|---|---|---|---|---|
| Uchihara et al.16 | 2022 | DM | Retrospective, observational | Japan | COVID-19 patients with newly diagnosed DM tended to progress into critical conditions compared to those with pre-existing DM (53% vs. 21%, P = 0.018). |
| Zhu et al.15 | 2020 | Retrospective longitudinal, multicentered | China | COVID-19 patients with T2D had a significantly higher mortality than non-diabetic individuals (8% vs. 3%, P < 0.001; adjusted HR, 1.5; 95% CI, 1.1–2.0). | |
| Guo et al.21 | 2020 | Retrospective, case series | China | Significantly higher serum levels of IL-6, CRP, ferritin, D-dimer (P < 0.01) in COVID-19 diabetic patients than non-diabetic individuals. | |
| Guo et al.23 | 2020 | CVDs | Retrospective, single-center case series | China | Plasma TnT levels in COVID-19 subjects correlated significantly with plasma high-sensitivity CRP levels (β = 0.530, P < 0.001) and plasma NT-proBNP levels (β = 0.613, P < 0.001). |
| D’Silva et al.38 | 2020 | RDs | Retrospective, comparative cohort | USA | Patients with RDs had over a three-fold higher odds of requiring mechanical ventilation (OR, 3.2; 95% CI, 1.2–8.9). Persisted after adjusting for age, BMI, smoking and comorbidities (adjusted OR, 3.1; 95% CI, 1.1–9.1) |
| Pham et al.44 | 2021 | Retrospective, cohort | USA | No statistical differences for mechanical ventilation need between COVID-19 patients with RDs who administered HCQ in comparison with non-HCQ group OR 1.5 95%CI 0.3–6.4. | |
| Dai et al.49 | 2020 | Malignancy | Retrospective, multicentre cohort | China | Higher mortality rates (OR, 2.3; 95% CI, 1.2–4.8); higher rates of ICU admission (OR, 2.8; 95% CI, 1.6–5.1); higher rates of presence of at least one severe or critical symptom (OR, 2.8; 95% CI, 1.7–4.4) in COVID-19 patients with malignancies. |
| Lee et al.58 | 2020 | Retrospective, cohort study | UK | Patients with haematological malignancies were associated with a more severe COVID-19 than those with solid organs cancer (OR, 1.6; 95% CI, 1.2–2.2). | |
| Simonnet et al.69 | 2020 | Obesity | Retrospective cohort study | France | OR for IMV in patients with BMI > 35 vs. Patients with BMI < 25, 7.4; 95% CI, 1.6–33.1. |
DM = diabetes mellitus, T2D = type 2 diabetes, HR = hazard ratio, CI = confidence interval, IL-6 = interleukin-6, CRP = C-reactive protein, TnT = troponin T, NT-proBNP = N-terminal pro-brain natriuretic peptide, RD = rheumatic disease, OR = odds ratio, HCQ = hydroxychloroquine, ICU = intensive care unit, IMV = invasive mechanical ventilation, BMI = body mass index.
COVID-19 and DM
Compared to other comorbidities, subjects with DM seem to be at a greater risk of severe COVID-19.13 Hyperglycemia with hemoglobin glycosylation may trigger the overly production of pro-inflammatory cytokines, oxygen radicals, underlying severe COVID-19 in DM.14 The resultant inflammatory response increases the invading potential of infectious agents and exhausts the immune system. Thus, tight blood glucose monitoring is a prerequisite for treating COVID-19 in subjects with new-onset DM.15
A retrospective study analyzed the course of SARS-CoV-2 in new-onset DM compared to the same in preexisting DM.16 Notably, new-onset DM presented with a more pronounced hyperglycemia at the beginning of COVID-19 and more frequently progressed into life-threatening conditions at the hospital admission.16 It is believed that hypoglycemic medications, such as glucagon-like peptide-1 agonists, thiazolidinediones, and sodium-glucose co-transporter-2 inhibitors, stimulate angiotensin-converting enzyme 2 (ACE-2) receptor overexpression, enabling SARS-CoV-2 entry into the host cells.1718 Overall, insulin-dependent conditions increase the risk of COVID-19 pneumonia compared to conditions treatable with oral antidiabetic agents.19
Another challenging factor is the combination of DM with arterial hypertension which adds to ACE-2 overexpression.20 Chronic subclinical inflammation in DM is yet another aggravating factor presenting with elevated neutrophil and lowered lymphocyte counts and contributing to cytokine storm syndromes.1521 COVID-19 in patients with DM often presents with high proinflammatory markers, including lactate dehydrogenase, C-reactive protein (CRP), ferritin, and D-dimer.1521 Clinical characteristics of COVID-19 and DM combination include high chest computer tomography scores suggestive of severe lung involvement.21 Finally, exposure to the infection in DM rarely stimulates production of anti-SARS-CoV-2 antibodies, predisposing these individuals to reinfections.
COVID-19 and CVDs
The association of SARS-CoV-2 with CVDs is well-established.2223 Subjects with severe COVID-19 had higher incidence of arterial hypertension than those with non-severe COVID-19.22 A meta-analysis revealed that the most common comorbid pathologies in COVID-19 were arterial hypertension (17%), cardiac and cerebrovascular diseases (16%), and DM (10%).22 Chen et al.12 reported that approximately 40% of patients infected with SARS-CoV-2 experience CVD or cerebrovascular disease. Cardiac magnetic resonance imaging in subjects who recently recovered from COVID-19 diagnosed new cardiac involvement in 78% of cases and myocardial inflammation in 60% of cases.24
SARS-CoV-2 infection may trigger new cardiac pathologies and/or exacerbate underlying CVD.25 It may directly and indirectly damage heart and vessels, presenting with acute coronary syndromes, cardiomyopathy, arrhythmias, and cardiogenic shock.26
Older age, DM, hyperlipidemia, and overexpression of ACE2 may confound severe COVID-19 in patients with CVD.32627 Viral dissemination from the respiratory tract to the blood stream may also act as a severity factor.28
Atrial and ventricular fibrillation, cardiac failure, myocarditis, and pulmonary embolic event have often been reported in COVID-19.2930 Accordingly, high-sensitivity cardiac troponin I (hs-cTnI), creatine kinase, N-terminal pro-brain natriuretic peptide (NT-proBNP), and D-dimer should be monitored in severe COVID-19 to timely diagnose cardiac damage.31
In a recent study, patients with increased troponin T (TnT) at hospitalization due to COVID-19 had poor clinical outcomes; they particularly developed malignant arrhythmias.23 The National Health Commission of China reported that about 12% of individuals with SARS-CoV-2 without established CVD were hospitalized with elevated TnT and cardiac arrest.32 More than half of COVID-19 patients with lethal outcomes also had high hs-cTnI at hospital admission.9
COVID-19 and RDs
SARS-CoV-2 triggers of Toll-like receptors and complement activation with formation of neutrophilic extracellular traps. All these factors may induce systemic autoimmune reactions in COVID-19.34 In fact, rheumatic patients infected with SARS-CoV-2 are likely to develop generalized microvascular thromboses mediated by complement activation, with a marked elevation of D-dimer.35
At the beginning of the COVID-19 pandemic, the European Alliance of Associations for Rheumatology (EULAR) reported no evidence of heightened risk of SARS-CoV-2 infection and severe COVID-19 in subjects with inflammatory rheumatic and musculoskeletal diseases.36 However, a survey of 494 RA patients revealed that 40% of them believed that the rheumatic disease and its treatment put them at risk of unfavorable course of COVID-19.37
Although subjects with RDs presented with the same clinical picture of COVID-19 as those without RDs, they often required mechanical ventilation (adjusted odds ratio [OR], 3.11).38 Increased age (OR, 4.83) and male gender (OR, 1.93) were independently associated with severe COVID-19 in patients with chronic inflammatory arthritis and connective tissue diseases compared to non-rheumatic controls.39
In the time of the pandemic, subjects with RDs have experienced unjustified discontinuation of disease-modifying antirheumatic drug (DMARD) therapies due to the short supply of hydroxychloroquine (HCQ) and tocilizumab.40 A multi-center patient survey revealed that 42% of respondents had difficulties with obtaining HCQ and 41% of them experienced worsened disease course due to the DMARDs shortage.41
The efficacy of HCQ has raised numerous questions and concerns during the COVID-19 pandemic.42 Arshad et al.43 reported that the therapy with HCQ alone or combined with azithromycin significantly reduced COVID-19 mortality rates. However, Pham et al.44 stated there were no statistical differences in mechanical ventilation between subjects with RDs who were treated with HCQ compared to those who were not treated with HCQ (OR, 1.5; 95% confidence interval [CI], 0.3–6.3). Similar results were reported in relation to in-hospital mortality (OR, 0.8; 95% CI, 0.1–4.6).44
Many other treatment strategies have been tried for SARS-CoV-2. The anti-inflammatory and immunomodulatory properties of glucocorticoids have been well explored.45 In multivariable models, prednisone dose ≥ 10 mg/day was associated with frequent hospital admissions (OR, 2.0; 95% CI, 1.1–4.0).46 Meanwhile, treating with conventional DMARDs alone or combined with biologics/Janus Kinase inhibitors was not linked to hospital admission (OR, 1.2; 95% CI, 0.7–2.2 and OR, 0.7; 95% CI, 0.4–1.5, respectively).46
Overall, in the wake of the COVID-19 pandemic, patients with RDs on long-term corticosteroid therapy were advised to continuing immunosuppressive therapy and to gradually lowering corticosteroid doses to 5–7.5 mg/daily.47
COVID-19 and neoplasms
Numerous studies have revealed that COVID-19 patients with preexisting or active malignancy are at a greater risk of severe disease and even death.4849505152 Higher mortality rates (OR, 2.3; 95% CI, 1.2–4.8) and higher rates of intensive care unit (ICU) admission (OR, 2.8; 95% CI, 1.6–5.1) were reported in COVID-19 subjects with malignancies.49
Logistic regression analyses have showed that several factors were associated with increased 30-day COVID-19-related mortality: older age, male gender, smoking, and active cancer.53 Some studies have determined risk factors of COVID-19 severity in subjects with malignancy.5455 A multicentre, retrospective cohort study reported that advanced cancer stage (OR, 2.6; 95% CI, 1.1–6.4), high levels of tumour necrosis factor-α (OR, 1.2; 95% CI, 1.0–1.5), elevated NT-proBNP (OR, 1.7; 95% CI, 1.03–2.8), reduced CD4+ T cells (OR, 0.8; 95% CI, 0.7–0.9), and reduced albumin–globulin ratio (OR, 0.1; 95% CI, 0.02–0.8) were all distinguished as severe disease factors.54 In a global database (TERAVOLT) older age (above 65) (OR, 1.9; 95% CI, 1.0–3.6), smoking (OR, 4.2; 95% CI, 1.7–12.9), and chemotherapy (OR, 2.5; 95% CI, 1.1–6.1) were also associated with risk of death in COVID-19 patients with cancer.55 There were no differences in COVID-19 mortality rates between subjects with active and inactive cancer treatments.56
COVID-19 patients with cancer were at risk of death due to delays in diagnosis and required therapies.57 There was about 10% higher risk of death in patients with breast malignancies during the pandemic compared to pre-pandemic period.57
COVID-19 severity differed widely across different cancers. Subjects with leukemia, lymphoma, and myeloma experienced more severe COVID-19 than those with solid cancer (OR, 1.6; 95% CI, 1.2–2.2).58 Case fatality rate for cohorts with cancer who died due to COVID-19 was about 37% for hematologic malignancies and 25% for solid cancers.59
Patients with cancer were susceptible to infections of the respiratory tract due to cancer-related immunosuppression, requiring more cautious approaches to immunosuppression therapies to mitigate risks of more severe outcomes.60
COVID-19 and obesity
Preliminary data suggest subjects with obesity experience more severe COVID-19.6162 Obesity has been reported as the second most common comorbidity in case series of COVID-19.7 Cai et al.61 reported that obese subjects often develop severe COVID-19 compared to those with normal weight (OR, 3.4; 95% CI, 1.4–2.9). Although COVID-19 pandemic generally led to the rise in body mass index (BMI) z-score (OR, 2.5; 95% CI, 2.0–2.9) to (OR, 2.6; 95% CI, 2.0–3.2) in children and adolescents with obesity,63 obese children presented with severe clinical course during the delta predominance (adjusted OR, 6.1; 95% CI, 1.2–29.6).64
Obese people demonstrate reduced pulmonary compliance and chest wall compliance due to high pulmonary blood volume.65 Fat accumulation in the diaphragm and abdomen facilitates viral entry due to activated ACE-2 receptors, increases viral load, and stimulates proinflammatory cytokines efflux with low-grade inflammatory response.66 The proinflammatory state may deteriorate pro- and anticoagulant dysbalance and lead to thromboses.67 Additionally, high plasma leptin levels in obesity may contribute to severe COVID-19. In fact, circulating levels of leptin, tumor necrosis factor-α, C-X-C motif chemokine ligand 10, and monocyte chemoattractant protein-4 were all significantly associated with severe COVID-19 compared to healthy controls.62
Obese patients with COVID-19 are at higher risk of hospitalization, ICU admission, and death.68 The need for invasive mechanical ventilation (IMV) increases with BMI.69 COVID-19 patients with BMI > 35 admitted to ICU have a 7-fold higher risk of IMV than those with BMI < 25.69 Patients below 60 years with BMI 30–34 were two times more likely to be hospitalized and admitted to ICU, compared to individuals with BMI < 30.70 Generally, age, gender, BMI ≥ 35 and smoking status predict oxygenation therapy.71
Our bibliometric analysis has several limitations. We searched through the Scopus database only and the articles in language other than English were filtered out and not included in the study. We also focused on few comorbidities. Nevertheless, we managed to emphasize the need for personalized data on risk factors, clinical course, possible complications, and outcomes of COVID-19.
In conclusion, comorbidities are typical in COVID-19 patients putting them at greater risk of adverse outcomes. Bibliometric analyses summarize available data and highlight directions of future research. Studies on specific types of chronic comorbidities need to be conducted. High priority should be placed on future studies of cohorts with comorbidities to provide specified clinical management.
 XML Download
XML Download