

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to WHO, the number of patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has exponentially increased with the spread of the global pandemic, with 595 million people having been infected worldwide as of August 25th, 2022.1 Although several vaccines and treatments have been developed for coronavirus disease 2019 (COVID-19), concerns regarding this disease remain. The sequelae of COVID-19, which go beyond infection and persist for a long time, are emerging as another social issue. COVID-19 sequelae may present in various forms, including not only systemic and respiratory symptoms, but also those affecting cardiovascular, nervous, and gastrointestinal systems.2 The most common symptoms of post-COVID-19 condition include fatigue, depression, and cognitive impairment.3 A prior study reported that 52.7% of patients showed sequelae of COVID-19 one year after acute infection with SARS-CoV-2; the most common symptoms were concentration difficulty, cognitive dysfunction, amnesia, depression, fatigue, and anxiety, in that order.45 Neurological and psychiatric symptoms persist for a particularly long time.67
Neurocognitive manifestations are also common in post-COVID-19 conditions. In a meta-analysis investigating the prevalence of neurological symptoms 3 months or more after SARS-CoV-2 infection, the prevalence of brain fog was 32.17% (95% confidence interval [CI], 10.31–54.03), that of memory impairment was 28.44% (95% CI, 21.52–35.35), and that of concentration difficulty was 21.84% (95% CI, 7.30–36.38).48 Brain fog refers to a state in which a feeling of emptiness persists along with the inability to express thoughts and expressions clearly, which is commonly described as a fog in the head.6 There has been an increasing number of reports discussing neurocognitive impairments in COVID-19 patients, including decreased concentration and memory impairment. Such patients often show few abnormalities in cognitive tests, which may not be severe enough to limit daily life. Moreover, a recent study reported structural changes in the brain following SARS-CoV-2 infection, which indicates that monitoring of long-term prognosis is important in such cases.9
Headache is a common symptom of COVID-19, with a prevalence varying from 14% to 60%.8 Even after the acute phase of SARS-CoV-2 infection, headache may persist for weeks.10 In one meta-analysis, the rate of complaints of headache even after 3 months of infection with COVID-19 was reported to be 15.13% (95% CI, 4.47–25.79).8
In the present study, we investigated the factors associated with neurological manifestations of post-COVID-19 conditions based on data from a specialized clinic.
Go to : 
METHODS
Study participants
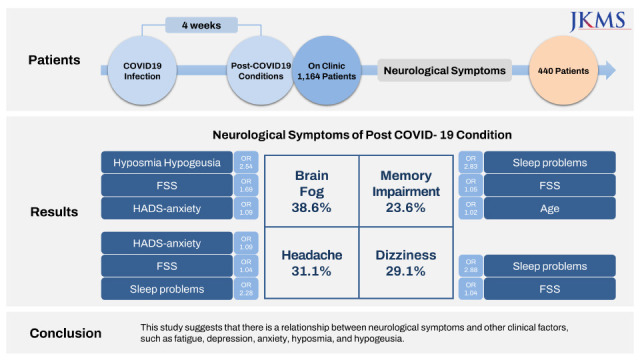
We retrospectively collected the data of 1,164 patients registered at the “Post-COVID-19 Clinic” of Myongji Hospital in Goyang, Republic of Korea between March 21, 2022 and April 22, 2022. All participants provided a detailed medical history, including the date of diagnosis of COVID-19, physical examination, and a questionnaire on their symptoms. The Hospital Anxiety and Depression Scale (HADS) was used to evaluate anxiety and depression, and the Fatigue Severity Scale (FSS) was applied to evaluate fatigue. The administered questionnaire queried patients about the post-COVID-19 symptoms they were experiencing, including headache, dizziness, memory impairment, brain fog (cloudy-headed feeling), hyposmia, hypogeusia, and sleep problems. The exclusion criteria were as follows: visit to the clinic less than 4 weeks after diagnosis of COVID-19, uncertainty regarding the date of diagnosis, refusal to answer the questionnaire, and missing data in the FSS, HADS-Depression, or HADS-Anxiety. Among 1,164 patients, 440 patients who visited the clinic after a period longer than 4 weeks were included and investigated for neurological and psychiatric manifestation.
Assessment of depression and anxiety
Anxiety and depression symptoms were assessed using the seven-item subscales of the HADS-Anxiety and HADS-Depression).11 The HADS is designed to minimize reporting of somatic symptoms of anxiety and depression in medically ill people and is considered to have a sensitivity and specificity of approximately 0.80 when applying a cut-off score of > 7 from a total possible score of 21 for both HADS-Anxiety and HADS-Depression.12 Each item of the HADS was scored from 0 to 3. The seven-item scores were summed to obtain the final HADS-anxiety and HADS-depression scores.
Assessment of fatigue
Fatigue is defined as a sense of physical tiredness and lack of energy distinguishable from sadness or weakness.13 The FSS, developed by Krupp et al., is the most commonly used self-report questionnaire to measure fatigue.1314 It consists of nine items scored on a Likert scale from 1 to 7. The mean of all scores was taken as the final score, with a higher score indicating a higher level of fatigue.
Statistical analysis
To evaluate differences in demographic and clinical characteristics, we performed analysis of variance (ANOVA) for continuous variables and χ2 testing for categorical variables. The prevalence of symptoms in post-COVID-19 conditions was compared using the χ2 test.
Logistic regression analysis was performed to identify whether each neurological and psychiatric symptom was associated with various risk factors (age, sex, hospitalization, presence of pneumonia, HADS-Anxiety, HADS-Depression, FSS, the presence of sleep problems, and the presence of hyposmia or hypogeusia). The results of multivariate logistic regression analyses are presented as odds ratios (ORs) with 95% CIs. We also calculated the variance inflation factors of those variables to rule out the possibility of multicollinearity. To determine whether fatigue, depression, and anxiety were independent variables contributing to each neurological and psychiatric symptom in post-COVID-19 conditions, we calculated the multivariable-adjusted ORs and 95% CIs after adjusting for potential covariates. The χ2 test was performed to compare the rate of accompanying hyposmia and hypogeusia between dichotomous groups (group with each symptom vs. group without each symptom). Statistical significance was set at P ≤ 0.05. All analyses were performed using SPSS software (SPSS 22 Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board of Myongji Hospital and was performed in accordance with the approved protocols and guidelines (MJH-2022-07-015). The requirement for informed consent was waived by the Institutional Review Board of Myongji Hospital since the study used retrospective de-identified data collected during health examination visits.
Go to :
RESULTS
Baseline characteristics of participants
Overall, we analyzed the data of 440 participants, of whom 292 (66.4%) were female. The most prevalent age group was the 60s (n = 120, 27.3%), followed by the 50s (n = 111, 25.2%), and the 40s (n = 85, 19.3%). The mean value of the HADS-Anxiety was 6.0 ± 4.7, that of the HADS-Depression was 7.5 ± 4.7, and that of FSS was 4.2 ± 1.7 (Table 1).
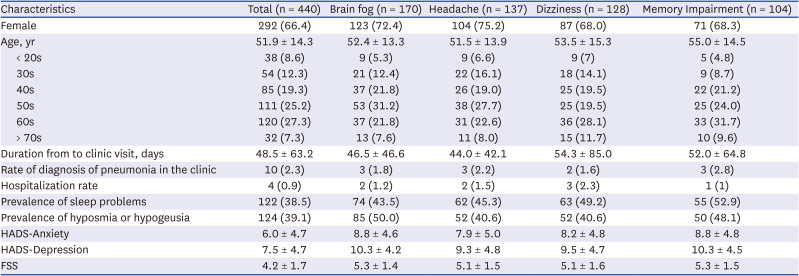
Table 1
Demographic and clinical characteristics of study participants
Values are presented as mean ± standard deviation or number (%).
HADS = Hospital Anxiety and Depression Scale, FSS = Fatigue Severity Scale.
![]()
Brain fog was the most common symptom in 170 patients (38.6%), followed by headache in 137 (31.1%), dizziness in 128 (29.1%), and memory impairment in 104 (23.6%) (Fig. 1). Among those who complained of neurological and psychiatric symptoms, brain magnetic resonance imaging was performed in six patients and brain computerized tomography was performed in 12 patients; no structural problems were observed that may cause associated neurological and psychiatric symptoms.

Association between symptoms and potential risk factors
Logistic regression analysis showed that brain fog was associated with hyposmia or hypogeusia (OR, 2.54; 95% CI, 1.51–4.27; P < 0.001), FSS (OR, 1.06; 95% CI, 1.04–1.09; P < 0.001), and HADS-Anxiety (OR, 1.09; 95% CI, 1.01–1.18; P = 0.037). Memory impairment was associated with sleep problems (OR, 2.83; 95% CI, 1.69–4.74; P < 0.001), FSS (OR, 1.05; 95% CI, 1.02–1.07; P < 0.001), and age (OR, 1.02; 95% CI, 1.00–1.04; P = 0.015). Headache was associated with sleep problems (OR, 2.28; 95% CI, 1.42–3.68; P = 0.001), sex (OR, 1.68; 95% CI, 1.02–2.77; P = 0.042), and FSS (OR, 1.04; 95% CI, 1.02–1.06; P < 0.001). Dizziness was associated with sleep problems (OR, 2.88; 95% CI, 1.77–4.68; P < 0.001), and FSS (OR, 1.04; 95% CI, 1.02–1.06; P < 0.001) (Table 2).
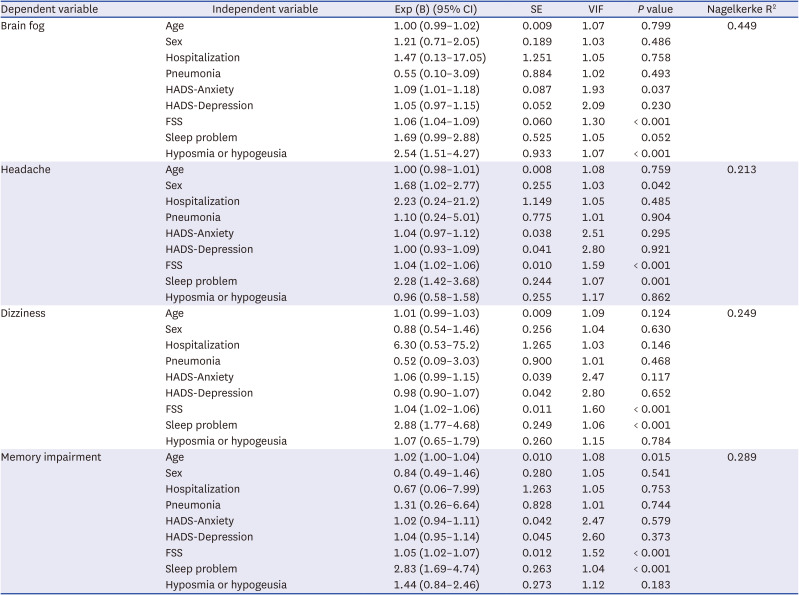
Table 2
Logistic regression using neurological and psychiatric symptoms of post-COVID-19 conditions as dependent variables
COVID-19 = coronavirus disease 2019, CI = confidence interval, SE = standardized error, VIF = variance inflation factor, HADS = Hospital Anxiety and Depression Scale, FSS = Fatigue Severity Scale.
![]()
Association between symptoms of post-COVID-19 conditions with hyposmia and hypogeusia
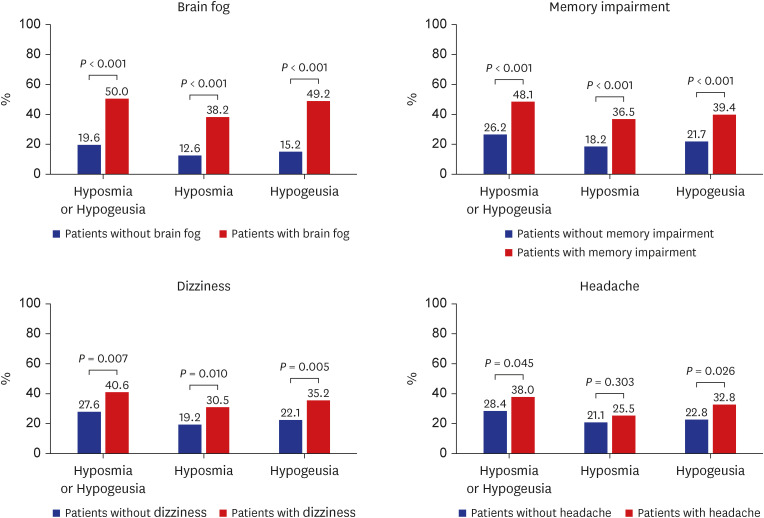
In the group of patients with brain fog, 50% of patients had hyposmia or hypogeusia (P < 0.001). When the prevalence of hyposmia and hypogeusia were retrospectively compared, 38.2% were found to have had hyposmia (P < 0.001) and 49.2% had hypogeusia (P < 0.001); both of these prevalences were significantly higher than those in patients without brain fog. In the group of patients with memory impairment, 48.1% had hyposmia or hypogeusia (P < 0.001); overall, 36.5% of patients with memory impairment had hyposmia (P < 0.001) and 39.4% had hypogeusia (P < 0.001), showing a significantly higher prevalence than that in those without memory impairment. In the group with dizziness, 40.6% had hyposmia or hypogeusia (P = 0.007). In addition, 30.5% of patients with dizziness had hyposmia (P = 0.010) and 35.2% had hypogeusia (P = 0.005), which were all significantly higher than the prevalences in those without dizziness. In the group with headache, 38.0% had hyposmia or hypogeusia (P = 0.045), including 32.8% of patients with hypogeusia (P = 0.026), which was higher than the corresponding prevalence in those without headache. The prevalence of hyposmia did not significantly different between patients with and without headaches (P = 0.303) (Fig. 2).
Association of symptoms of post-COVID-19 conditions with fatigue
In patients with definite fatigue defined as an FFS score of 5 or more, after controlling for age, sex, HADS-Depression, HADS-Anxiety, presence of hyposmia or hypogeusia, and presence of sleep problems, the adjusted OR was 3.84 (95% CI, 2.26–6.51; P < 0.001) for brain fog, 2.76 (95% CI, 1.51–5.05; P = 0.001) for memory impairment, 1.85 (95% CI, 1.12–3.05; P = 0.016) for headache, and 2.07 (95% CI, 1.23–3.47; P = 0.006) for dizziness (Table 3).

Table 3
Association between the symptoms of post-COVID-19 condition and fatigue
Adjusted for age, sex, HADS-Depression, HADS-Anxiety, hyposmia or hypogeusia, and sleep problems.
COVID-19 = coronavirus disease 2019, FSS = Fatigue Severity Scale, OR = odds ratio, CI = confidence interval, HADS = Hospital Anxiety and Depression Scale.
![]()
Association symptoms with anxiety and depression
Patients with any anxiety (HADS-Anxiety score ≥ 8) were correlated with brain fog (OR, 3.36; 95% CI, 2.18–5.52; P < 0.001), dizziness (OR, 2.24; 95% CI, 1.42–3.53; P = 0.001), memory impairment (OR, 2.11; 95% CI, 1.27–3.52; P = 0.004) and headache (OR, 1.94; 95% CI, 1.24–3.04; P = 0.004). Patients with severe anxiety (HADS-Anxiety score ≥ 11) were correlated with dizziness (OR, 3.05; 95% CI, 1.78–5.24; P < 0.001), brain fog (OR, 2.50; 95% CI, 1.42–4.40; P = 0.002), memory impairment (OR, 2.50; 95% CI, 1.41–4.40; P < 0.001) and headache (OR, 2.29; 95% CI, 1.34–3.91; P = 0.003) (Table 4). When patients had any depression (HADS-Depression score ≥ 8), there was a correlation with brain fog (OR, 4.64; 95% CI, 2.94–7.33; P < 0.001), memory impairment (OR, 3.37; 95% CI, 2.13–5.97; P < 0.001), dizziness (OR, 2.22; 95% CI, 1.41–3.49; P = 0.001), and headache (OR, 1.82; 95% CI, 1.17–2.82; P = 0.008). When the patients had severe depression (HADS-Depression score ≥ 11), there was a correlation with brain fog (OR, 4.27; 95% CI, 2.62–6.95; P < 0.001), memory impairment (OR, 2.72; 95% CI, 1.63–4.54; P < 0.001), dizziness (OR, 2.16; 95% CI, 1.35–3.44; P = 0.001), and headache (OR, 2.00; 95% CI, 1.26–3.18; P = 0.003).

Table 4
Association between symptoms of post-COVID-19 condition with anxiety and depression
The OR was adjusted for age, sex, hyposmia or hypogeusia, and sleep problems.
COVID-19 = coronavirus disease 2019, HADS = Hospital Anxiety and Depression Scale, OR = odds ratio, CI = confidence interval.
![]()
Go to :
DISCUSSION
In the present study, we investigated the factors associated with neurological and psychiatric symptoms of post-COVID-19 conditions in 440 patients with symptoms persisting for longer than 4 weeks after SARS-CoV-2 infection. Brain fog was the most common neuropsychiatric symptom, followed by headache, dizziness, and memory impairment. Neurocognitive symptoms, including brain fog, memory impairment, headache, and dizziness, were found to be associated with hyposmia or hypogeusia, high FSS scores, sleep problems, high HADS scores, and advanced age. The patients with neurological and psychiatric symptoms showed a higher rate of accompanying hyposmia or hypogeusia than those without.
Numerous prior studies have investigated neurocognitive symptoms associated with post-COVID-19 conditions. In neuropsychological test, patients who recovered after SARS-CoV-2 infection and had no history of dementia showed a decline in performance in information processing speed (18%), executive function (16%), phonological fluency (15%), categorical fluency (20%), and memory encoding (24%).15 In addition, when cognitive function changes were followed 1 year later in people aged older than 60 infected with SARS-CoV-2, the infected group had significantly lower cognitive test scores than the control group.16 Moreover, compared to the mildly infected or control group, the group with severe infection had a lower cognitive function score and a higher risk of progressive cognitive decline.16 Recent studies on the brain imaging findings of patients infected with SARS-CoV-2 have also been published. A study of a cohort from the UK Brain Bank revealed that the gray matter thickness of the orbitofrontal cortex and parahippocampal gyrus was decreased, and markers related to tissue damage were more varied in the primary olfactory cortex and functionally connected areas, with a greater decrease in global brain size in the severe group.9 Among these studies on neurocognitive symptoms of post-COVID-19 conditions, our study is unique in that it suggests that memory impairment or brain fog in post-COVID-19 conditions may be related to sleep problems, depression or anxiety, fatigue, and hyposmia or hypogeusia.
Headache after SARS-CoV-2 infection is also related to the immune response activated during infection.7 Prior studies have indicated that the inflammatory reaction that occurs during infection may cause or worsen or chronicize existing headaches.1718 It is reasonable to consider that post-COVID-19 syndrome-related headaches are symptoms that can persist for a long time after general viral infection, rather than being directly related to SARS-CoV-2 infection.1019 Furthermore, there are reports of new daily persistent headache after infection with Epstein-Barr virus and following the Russian flu pandemic of 1890.1920 However, these previous reports did not suggest which factors were related to headache. Our study suggests that headache is associated with sleeping problems and fatigue. This knowledge may help physicians consider interventions for fatigue and sleep problems in conjunction, which would improve the management of patients with headache after SARS-CoV-2 infection.
In the present study, fatigue was found to be associated with all symptoms, including brain fog, memory impairment, headaches, and dizziness. According to a recent study, post-COVID-19 fatigue is associated with cognitive and neuropsychiatric symptoms, which is consistent with our study results.21 Moreover, previous studies have reported that viral infection is associated with fatigue syndrome, not only in SARS-CoV-2 infection, but also in infection with severe acute respiratory syndrome, Epstein-Barr virus, and other viruses.2223 The mechanism by which fatigue persists after infection may involve a decrease in neurotransmission due to the accumulation of inflammatory cytokines.2425
The mechanisms underlying neuropsychiatric symptoms persisting after SARS-CoV-2 infection may be associated with neuroinflammation.26 According to a previous study, when cytokine levels were measured 1-3 months after SARS-CoV-2 infection, interleukin (IL)-4 levels were increased in all participants, and the presence of persistent neurological and psychiatric symptoms showed a positive correlation with the IL-6 levels.27 According to the meta-analysis, even 12 weeks after SARS-CoV-2 infection, one-third of patients complained of fatigue, and more than one-fifth complained of cognitive decline, and the inflammatory parameters were high in patients complaining of fatigue and cognitive impairment.23 This suggests that both persistent neuropsychiatric symptoms and fatigue in post-COVID-19 conditions may be associated with inflammatory response.23 In addition, high C-reactive protein level was associated with depression, sleep problems, fatigue, and anxiety, while high IL-6 activity was associated with fatigue and sleep in 14,748 patients from the UK Biobank and 2,905 patients from the Netherlands.28 This suggests that activation of immune response after SARS-CoV-2 infection causes neuroinflammation, which may cause various neurological and psychiatric sequelae.
In addition, similar to our study, several reports have indicated that post-COVID-19 brain fog is associated with hyposmia.29 There are several possible hypotheses to explain this: 1) olfactory circuits are adjacent to memory circuits such as the hippocampus, and 2) the virus can directly invade nerves through the CSF, vasculature, or nervus terminalis.30
This study is noteworthy as it shows the factors associated with neurological and psychiatric symptoms of post-COVID-19 conditions in 440 patients. This study may guide physicians to identify and intervene in the management of patients with persistent symptoms after SARS-CoV-2 infection. However, our study had some limitations. First, subjective complaints of symptoms were acquired using a questionnaire and only a few objective cognitive tests or brain images were performed. Second, as there is no definite consensus in defining post-COVID-19 conditions, all patients who presented to the clinic with varying subjective symptoms were included for data acquisition. Especially, there is no diagnostic criteria or evaluation tool for brain fog, it was difficult to be clearly defined or quantified. Future studies are warranted to substantiate the criteria and analysis of associated symptoms in depth. Third, because our study was based on single-centered, retrospective, cross-sectional data from the designated clinic, there might be selection bias. The patients with severe infections who were admitted to the hospital may not have visited the clinic. In addition, those with severe memory impairment due to post-COVID-19 symptoms would have visited the neurology department directly, and not included in this study. A prospective longitudinal cohort study design will also provide more clear findings than a retrospective, cross-sectional design.
In conclusion, even 4 weeks after acute infection with SARS-CoV-2, patients continued to complain of neurological and psychiatric symptoms, such as brain fog, memory impairment, headache, and dizziness. In the present study, brain fog was found to be associated with hyposmia or hypogeusia, fatigue, and anxiety. Memory impairment is associated with fatigue, sleep problems, and aging. Headache is associated with sex, fatigue, and sleep disorders. Dizziness is associated with fatigue and sleep problems. Follow-up studies of the long-term prognosis of post-COVID-19 conditions are warranted in the future.
Go to :
 XML Download
XML Download