

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
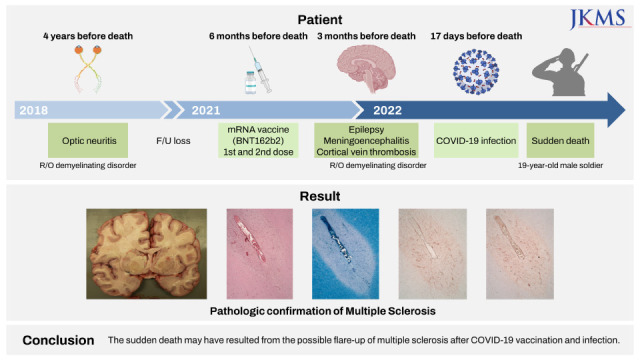
Despite the unknown causal relationship, several studies have reported that the first manifestation or relapse of multiple sclerosis (MS) is temporally associated with coronavirus disease 2019 (COVID-19) vaccination or infection.12345678910111213141516 Recently, we encountered an autopsy case of a young Korean male with undiagnosed MS of which possible flare-ups were preceded by both COVID-19 vaccination and infection. Herein, we present the detailed clinical and histopathological findings of an autopsy case and review the literature.
Go to : 
CASE DESCRIPTION
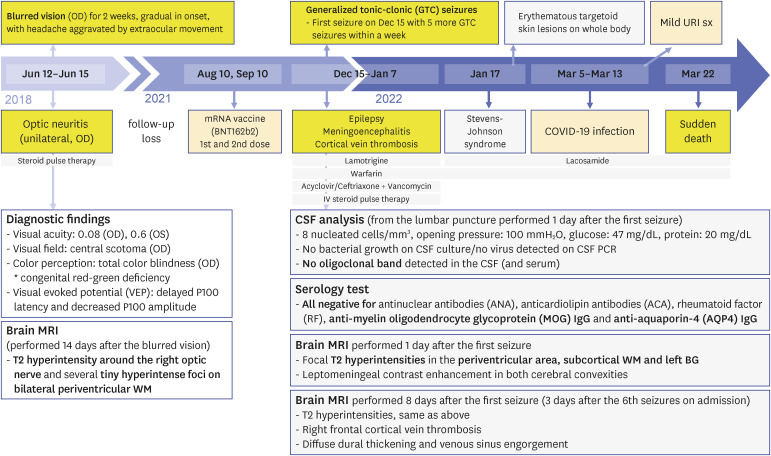
On the morning of March 22, 2022, a 19-year-old male soldier was found dead in the barrack. The body was located in a sleeping bag under the bed. The deceased’s posture was supine, with his head slightly turned to the right and his right arm raised. The sleeping bag was wet with urine. During the last few days before his sudden death, he had been suffering from left finger numbness at night and because of this, he asked his company commander for exemption from night duty. One day before the sudden death, the deceased said to his colleague “I cannot sleep well these days and I feel like I'm having a seizure at night.”
The medical history of the deceased is summarized in Fig. 1. About 4 years before death, he had been diagnosed with unilateral ON. Demyelinating disease was suspected in the brain magnetic resonance imaging (MRI), but he was lost to further follow up after his vision recovered. Six months before death, he had received the second dose of the COVID-19 vaccine (Pfizer-BioNTech), and 3 months later, he started experiencing epileptic seizures during sleep and was admitted to an outside hospital. Since the first seizure, he presented with 5 more generalized tonic-clonic seizures within a week. Besides seizures, he presented with no other symptoms or signs of meningeal irritation. Cerebrospinal fluid (CSF) analysis including culture and viral polymerase chain reaction revealed no abnormalities except for mild pleocytosis. Oligoclonal band and aquaporin-4 antibodies were not detected in the CSF and serum. Brain MRI performed 1 day after the seizure revealed T2 hyperintensities in the periventricular region, subcortical white matter, and left basal ganglia, raising a suspicion of demyelinating disorder, and leptomeningeal enhancement of cerebral convexities. Additional brain MRI performed 8 days after the first seizure revealed diffuse dural thickening and venous sinus engorgement with focal cortical venous thrombosis, which were suggestive of cerebral venous thrombosis (CVT) due to intracranial hypotension. Under the clinical impression of epilepsy, meningoencephalitis and focal cortical venous thrombosis, he was treated with empirical antiviral/antibiotic medications, anticonvulsant and anticoagulant for 3 weeks and was discharged after symptom improvement. Seizures seemed to be controlled with medication management. During regular follow-up, he suffered Stevens-Johnson syndrome (SJS). As a cause, an anticonvulsant (lamotrigine) was suspected and replaced with lacosamide. No recurrence of epileptic seizure was observed after the change of anticonvulsant. Seventeen days before his death, he developed a sore throat without fever, and tested positive for COVID-19 while he was on leave, being with his family. Eight days before his death, he returned to duty after conservative follow-up on home isolation. Additional brain MRI was not performed during this follow-up period.
An autopsy was conducted 1 day after death. External examination revealed diffuse dyschromic macules on trunk and limbs which were suspected to be old sequelae of SJS. Teeth imprints on both ventral and dorsal sides of the tongue were present. The brain weighed 1,550 g (age-matched normal value: 1,450 ± 20 g) and showed no gross abnormalities, including hemorrhage or meningitis. No intravascular or venous sinus thrombi were identified. Coronal sections of the brain showed multifocal, relatively well-circumscribed, gray-tan, irregular-shaped discoloration in the periventricular areas, cerebral deep white matter (frontal, parietal, and temporal lobes), internal capsule, and corpus callosum (Fig. 2). Cerebellum and brainstem were grossly unremarkable. Histologically, multifocal white matter lesions exhibited loss of myelin with Luxol fast blue and relatively preserved neuropils by immunostaining for phosphorylated neurofilaments, consistent with demyelinated plaques (Figs. 3 and 4). Active plaques characterized by abundant myelin-containing macrophages and perivenous lymphocytic infiltrates were mostly identified in the cerebral white matter and internal capsule. Inactive plaques characterized by reactive gliosis, sharply demarcated demyelination, and virtually no macrophages were mainly located in the periventricular areas, optic nerve, and corpus callosum. Microglial cell proliferation was noted in the peri-plaque and distant normal-appearing cerebral cortex and white matter. Perivascular lymphocytic cuffing in the parenchyma was frequently observed, and immunostaining for CD20, CD4, and CD8 demonstrated a mixed population of B- and T-lymphocytes, with CD8+ T-lymphocytes predominance. Additionally, multifocal lymphocytic infiltration was observed in the subarachnoid space of the cerebrum and was associated with subpial cortical band-like vacuolation, which was suspected to be cortical demyelination. Demyelinated plaques were not observed in cerebellum and brainstem. The other major organs including heart and lungs were unremarkable in both macroscopic and microscopic examination.
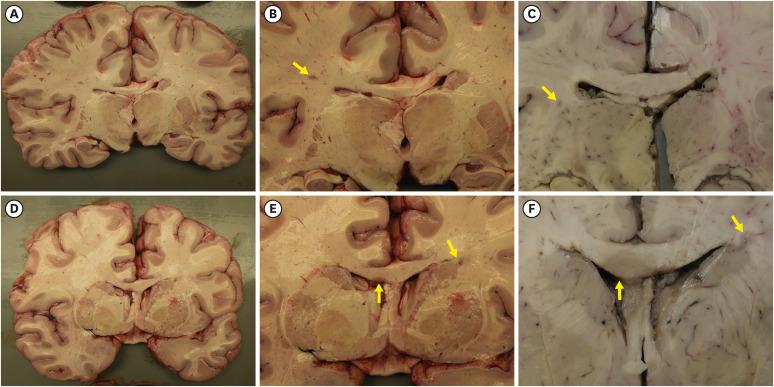 | Fig. 2Gross findings of the brain.(A-F) Coronal sections of the brain revealed multifocal, well-demarcated, gray-tan, demyelinated plaques (indicated by yellow arrows) in the deep white matter (B, C), corpus callosum and periventricular area (E, F). (B, E) are close-up photographs of sections in (A, D) respectively. The demyelinated plaques are different in their size and shape (B, C, E, and F). Sections in (C, F) are formalin-fixed. The venocentric distribution of the demyelinated plaques is grossly identified.
|
 | Fig. 3Gross-microscopic correlation of the multifocal lesions of the brain.The demyelinated plaque shown in (A-D) located at periventricular area and abuts basal ganglia. Local infiltrates of macrophages and lymphocytes are present in the plaque (B). LFB stain revealed myelin loss in the plaque, and a finger-like appearance of perivascular demyelination (C). Gliotic fibers are densely condensed within the plaques (D). The demyelinated plaque shown in (E-H) is hypercellular (F), sharply demarcated (G) and contains abundant macrophages and CD45-positive perivascular lymphocytic infiltrations in the plaque (H). The demyelinated plaque shown in (I-L) is a chronic active plaque and consists of central hypocellular inactive center and peripheral rim of macrophage. The macrophage infiltration as shown by CD68 immunostain is not evenly distributed but located preferentially in the peripheral edge of the plaque forming a “rim” (L).
Types of staining: (B, F, and J) H&E; (C, G and K) LFB; (D, H, and L) IHC staining for GFAP, CD45 and CD68. Original magnification: (B-D) ×25; (F-H) ×25; (J-L) ×25.
H&E = hematoxylin and eosin, LFB = Luxol fast blue, IHC = immunohistochemical, GFAP = Glial fibrillary acidic protein.
|
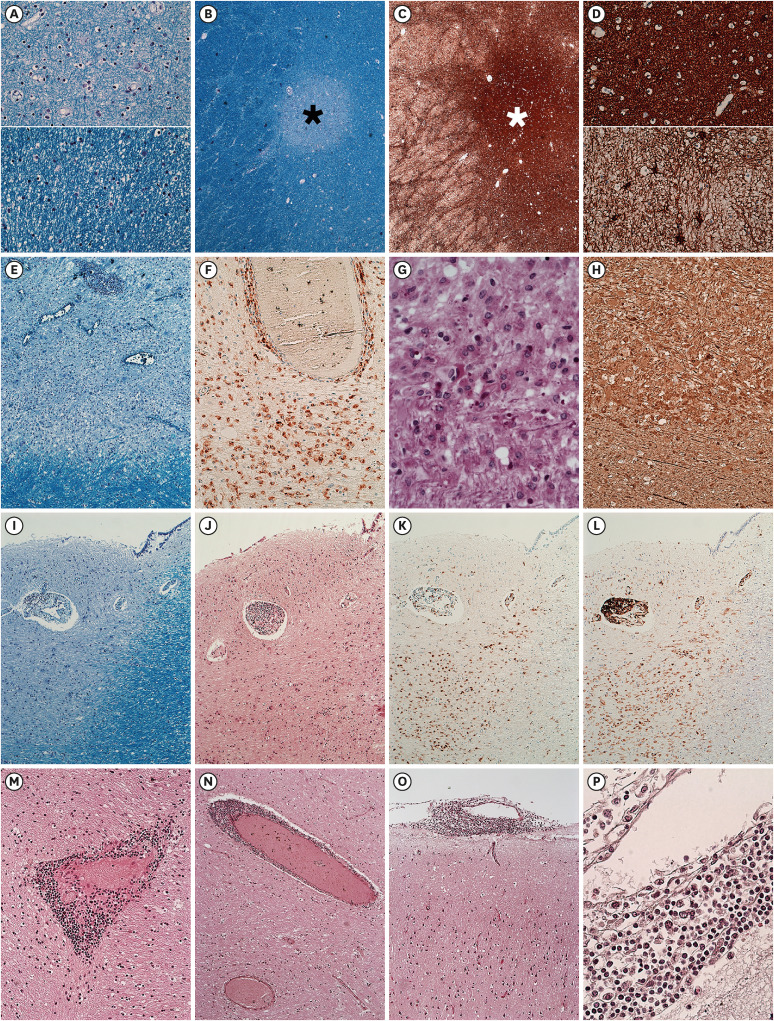 | Fig. 4Demyelinating plaque of different stages.The upper (A) and upper (D) correspond to the center of the plaques, (black asterisk of B and white asterisk of C) while the lower (A) and lower (D) correspond to the peri-plaque area. The center of the plaque shows diminished but not absent myelin fiber (A) and dense gliotic fiber (D). The lesion shown in (E-H) has abundant and evenly distributed macrophages in the plaque. The myelin loss of the plaque is identified (E). CD68-positive macrophages are abundant in the plaque (F). PAS-positive debris in the macrophage are identified (G). Immunohistochemical stain for phosphorylated NF revealed the relative axonal preservation in the plaque (H). The lesion shown in (I-L) abuts the lateral ventricle. Relatively well-defined demyelination is observed and highlighted on LFB (I-J). A peripheral rim of CD68-positive macrophage is observed (K). CD45-positive lymphocytes are located in the edge of the plaque (L). Perivascular lymphocytic cuffing in the parenchyma was frequently observed (M, N) along with lymphocytic infiltration in the leptomeninges (O, P).
Types of staining: (A, B, E, and I) LFB; (C, D) GFAP; (F, K) CD68; (G) PAS; (H) phosphorylated NF; (J, M, N, O, and P) H&E; (L) CD45. Original magnification: (A) ×50; (B, C) ×25; (D) ×50; (E) ×50; (F) ×200; (G) ×400; (H) ×200; (I-L) ×25; (M) ×200; (N, O) ×100; (P) ×400.
LFB = Luxol fast blue, GFAP = Glial fibrillary acidic protein, PAS = Periodic acid Schiff, NF = neurofilament, H&E = hematoxylin and eosin.
|
Toxicological examination revealed positive results for anticonvulsant (lacosamide) and anticoagulant (warfarin) within the therapeutic range.
Based on autopsy, histologic, and toxicological findings and medical records, the cause of death was determined to be MS with suspected exacerbation.
Ethics statement
Informed consent for publication of clinical data was obtained from the deceased’s family.
Go to :
DISCUSSION
The pathological hallmark of MS is spatially and temporally disseminated inflammatory demyelinating lesions in the central nervous system (CNS).1718 Although there is no single definite diagnostic test for MS, identification of the typical clinical presentations supported by MRI findings and CSF analysis can lead to an early and accurate diagnosis of MS.1819 However, in cases of atypical clinical presentation, the diagnosis of MS can be challenging.
ON is the initial manifestation in approximately one-fifth of patients with MS and may occur at least once in approximately half of them.20 ON with “typical” features tend to show unilateral involvement, spontaneous visual recovery within a month, favorable prognosis, and no deterioration after steroid withdrawal. The presence of white matter lesions found on T2-weighted brain MRI, even in asymptomatic patients, was strongly associated with an MS diagnosis in patients with ON.181921 Four years before death, the deceased had a history of unilateral ON and the brain MRI revealed T2 hyperintense lesions in the periventricular white matter at that time. Therefore, ON might have been the first manifestation of MS.
Acute disseminated encephalomyelitis (ADEM) is a rare inflammatory demyelinating disease of the CNS that may occur in young adults after viral infection or vaccination, which is the most important differential diagnosis in this case.17 Multiple demyelinated plaques centered on venules and inflammatory infiltrates including myelin-laden macrophages are supportive findings for ADEM. However, the presence of demyelinated plaques of different stages supports the diagnosis of MS, while ADEM is a monophasic inflammatory demyelinating process.
In addition to the MS lesion, brain MRI after his first seizure attack revealed slight leptomeningeal enhancement, which was suspected to be meningoencephalitis. As both acute meningoencephalitis and its long-term sequelae can induce epileptic seizures, the brain was thoroughly examined during autopsy for meningoencephalitis; however, leptomeninges were grossly unremarkable. Histologically, multifocal lymphocytic infiltration of the subarachnoid space, and perivascular lymphocytic cuffing in the parenchyma were identified, which can be seen in meningoencephalitis; however, typical pathological findings of viral encephalitis including microglial nodules and neuronophagia were absent. In fact, lymphocytic meningitis is another feature of particularly active MS.
An increased frequency of seizures has been noted in patients with MS. Clinically, the occurrence of epileptic seizures in MS does not correlate with the disease duration or severity.22 Although the underlying pathological mechanism of seizures in MS remain unelucidated, advanced imaging techniques suggest that cortical lesions are responsible for epileptogenesis.22 Multifocal leptomeningeal lymphocytic infiltration with subpial vacuolation in this case suggests cortical demyelination; however, confirmation by immunohistochemistry for myelin basic protein was not available. Whenever exacerbated, MS may have resulted in recurrent seizures via either inflammatory infiltration or suspected cortical demyelination.
Increased risk of epileptic seizure following CVT has been noted.23 However, in this case, the onset of seizure preceded the identification of CVT via brain MRI. A few cases of CVT without thrombocytopenia after receiving the COVID-19 mRNA vaccine have been reported although most post-vaccination thrombotic events occurred after the administration of viral vector-based vaccines, and an alternative explanation of the thrombotic event such as intracranial hypotension should be considered in this case.2425
The deceased’s death occurred unexpectedly in the benign circumstances. The deceased had a history of epilepsy, and the occurrence of terminal epileptic seizure is suspected, although his death was unwitnessed. No other structural abnormality except MS with suspected exacerbation is identified in the autopsy. From a forensic pathologist’s perspective, seizure in MS does matter because sudden unexpected death in epilepsy (SUDEP) is one of the most important direct causes of death in epilepsy patients.26 SUDEP is a heterogeneous category of death with many possible explanations for death including fatal arrhythmia or laryngospasm.27 Additionally, the occurrence of status epilepticus, an exclusion criterion for SUDEP, would be another possible explanation for his death. Suffocation due to positional impediment seems less likely considering the given situational information.28
Infection has long been recognized as etiologic factor for MS.29 Vaccines are designed to stimulate immune response against pathogen, but occasionally trigger autoimmune response. Since the COVID-19 pandemic, several cases of MS temporally associated with COVID-19 vaccination have been published. Cases reporting the first manifestation or relapse of MS after COVID-19 vaccination or infection are listed in Tables 1 and 2, respectively. Neither epileptic seizure as a symptom nor death as a clinical outcome has been documented in the previous reports. In this case, the initial onset of epileptic seizure is 96 days after the second dose of mRNA vaccination. Multifocal active demyelinated plaques may explain the onset of seizure and would be a manifestation of MS flare-up. Thus, relatively longer duration than previous reports would not completely exclude the possible causality between the vaccination and MS flare-up. Additionally, the deceased tested positive for COVID-19, 176 days after the second dose of the vaccine, and that is where “vaccine-induced immunity” could come in. Deterioration of previously well-controlled seizure might be another MS flare-up which occurred 17 days after the possible activation of vaccine-induced immunity.
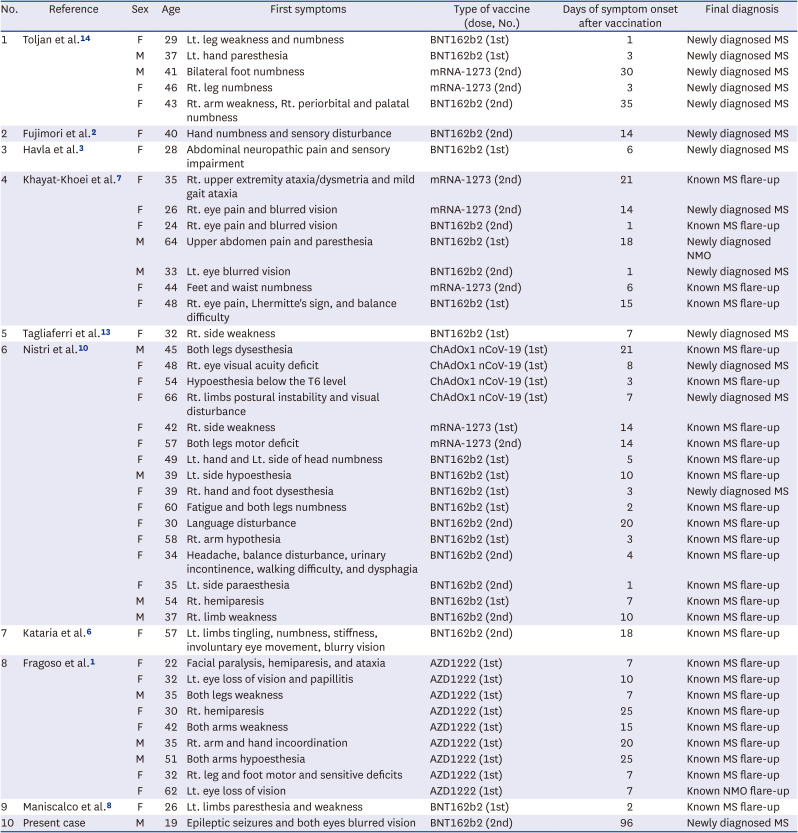
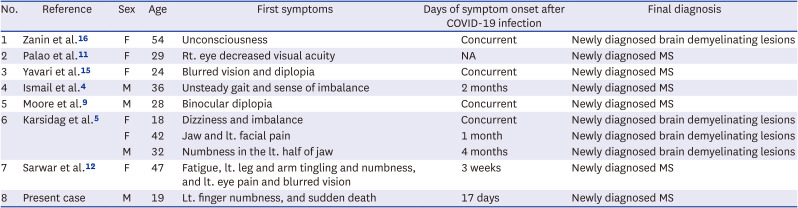
Table 1
Demographic and clinical features of previously reported demyelinating disease relapse cases following COVID-19 vaccination
| No. | Reference | Sex | Age | First symptoms | Type of vaccine (dose, No.) | Days of symptom onset after vaccination | Final diagnosis |
|---|---|---|---|---|---|---|---|
| 1 | Toljan et al.14 | F | 29 | Lt. leg weakness and numbness | BNT162b2 (1st) | 1 | Newly diagnosed MS |
| M | 37 | Lt. hand paresthesia | BNT162b2 (1st) | 3 | Newly diagnosed MS | ||
| M | 41 | Bilateral foot numbness | mRNA-1273 (2nd) | 30 | Newly diagnosed MS | ||
| F | 46 | Rt. leg numbness | mRNA-1273 (2nd) | 3 | Newly diagnosed MS | ||
| F | 43 | Rt. arm weakness, Rt. periorbital and palatal numbness | BNT162b2 (2nd) | 35 | Newly diagnosed MS | ||
| 2 | Fujimori et al.2 | F | 40 | Hand numbness and sensory disturbance | BNT162b2 (2nd) | 14 | Newly diagnosed MS |
| 3 | Havla et al.3 | F | 28 | Abdominal neuropathic pain and sensory impairment | BNT162b2 (1st) | 6 | Newly diagnosed MS |
| 4 | Khayat-Khoei et al.7 | F | 35 | Rt. upper extremity ataxia/dysmetria and mild gait ataxia | mRNA-1273 (2nd) | 21 | Known MS flare-up |
| F | 26 | Rt. eye pain and blurred vision | mRNA-1273 (2nd) | 14 | Newly diagnosed MS | ||
| F | 24 | Rt. eye pain and blurred vision | BNT162b2 (2nd) | 1 | Known MS flare-up | ||
| M | 64 | Upper abdomen pain and paresthesia | BNT162b2 (1st) | 18 | Newly diagnosed NMO | ||
| M | 33 | Lt. eye blurred vision | BNT162b2 (2nd) | 1 | Newly diagnosed MS | ||
| F | 44 | Feet and waist numbness | mRNA-1273 (2nd) | 6 | Known MS flare-up | ||
| F | 48 | Rt. eye pain, Lhermitte's sign, and balance difficulty | BNT162b2 (1st) | 15 | Known MS flare-up | ||
| 5 | Tagliaferri et al.13 | F | 32 | Rt. side weakness | BNT162b2 (1st) | 7 | Newly diagnosed MS |
| 6 | Nistri et al.10 | M | 45 | Both legs dysesthesia | ChAdOx1 nCoV-19 (1st) | 21 | Known MS flare-up |
| F | 48 | Rt. eye visual acuity deficit | ChAdOx1 nCoV-19 (1st) | 8 | Newly diagnosed MS | ||
| F | 54 | Hypoesthesia below the T6 level | ChAdOx1 nCoV-19 (1st) | 3 | Known MS flare-up | ||
| F | 66 | Rt. limbs postural instability and visual disturbance | ChAdOx1 nCoV-19 (1st) | 7 | Newly diagnosed MS | ||
| F | 42 | Rt. side weakness | mRNA-1273 (1st) | 14 | Known MS flare-up | ||
| F | 57 | Both legs motor deficit | mRNA-1273 (2nd) | 14 | Known MS flare-up | ||
| F | 49 | Lt. hand and Lt. side of head numbness | BNT162b2 (1st) | 5 | Known MS flare-up | ||
| M | 39 | Lt. side hypoesthesia | BNT162b2 (1st) | 10 | Known MS flare-up | ||
| F | 39 | Rt. hand and foot dysesthesia | BNT162b2 (1st) | 3 | Newly diagnosed MS | ||
| F | 60 | Fatigue and both legs numbness | BNT162b2 (1st) | 2 | Known MS flare-up | ||
| F | 30 | Language disturbance | BNT162b2 (2nd) | 20 | Known MS flare-up | ||
| F | 58 | Rt. arm hypothesia | BNT162b2 (1st) | 3 | Known MS flare-up | ||
| F | 34 | Headache, balance disturbance, urinary incontinence, walking difficulty, and dysphagia | BNT162b2 (2nd) | 4 | Known MS flare-up | ||
| F | 35 | Lt. side paraesthesia | BNT162b2 (2nd) | 1 | Known MS flare-up | ||
| M | 54 | Rt. hemiparesis | BNT162b2 (1st) | 7 | Known MS flare-up | ||
| M | 37 | Rt. limb weakness | BNT162b2 (2nd) | 10 | Known MS flare-up | ||
| 7 | Kataria et al.6 | F | 57 | Lt. limbs tingling, numbness, stiffness, involuntary eye movement, blurry vision | BNT162b2 (2nd) | 18 | Known MS flare-up |
| 8 | Fragoso et al.1 | F | 22 | Facial paralysis, hemiparesis, and ataxia | AZD1222 (1st) | 7 | Known MS flare-up |
| F | 32 | Lt. eye loss of vision and papillitis | AZD1222 (1st) | 10 | Known MS flare-up | ||
| M | 35 | Both legs weakness | AZD1222 (1st) | 7 | Known MS flare-up | ||
| F | 30 | Rt. hemiparesis | AZD1222 (1st) | 25 | Known MS flare-up | ||
| F | 42 | Both arms weakness | AZD1222 (1st) | 15 | Known MS flare-up | ||
| M | 35 | Rt. arm and hand incoordination | AZD1222 (1st) | 20 | Known MS flare-up | ||
| M | 51 | Both arms hypoesthesia | AZD1222 (1st) | 25 | Known MS flare-up | ||
| F | 32 | Rt. leg and foot motor and sensitive deficits | AZD1222 (1st) | 7 | Known MS flare-up | ||
| F | 62 | Lt. eye loss of vision | AZD1222 (1st) | 7 | Known NMO flare-up | ||
| 9 | Maniscalco et al.8 | F | 26 | Lt. limbs paresthesia and weakness | BNT162b2 (1st) | 2 | Known MS flare-up |
| 10 | Present case | M | 19 | Epileptic seizures and both eyes blurred vision | BNT162b2 (2nd) | 96 | Newly diagnosed MS |
![]()
Table 2
Demographic and clinical features of previously reported demyelinating disease relapse cases following COVID-19 infection
| No. | Reference | Sex | Age | First symptoms | Days of symptom onset after COVID-19 infection | Final diagnosis |
|---|---|---|---|---|---|---|
| 1 | Zanin et al.16 | F | 54 | Unconsciousness | Concurrent | Newly diagnosed brain demyelinating lesions |
| 2 | Palao et al.11 | F | 29 | Rt. eye decreased visual acuity | NA | Newly diagnosed MS |
| 3 | Yavari et al.15 | F | 24 | Blurred vision and diplopia | Concurrent | Newly diagnosed MS |
| 4 | Ismail et al.4 | M | 36 | Unsteady gait and sense of imbalance | 2 months | Newly diagnosed MS |
| 5 | Moore et al.9 | M | 28 | Binocular diplopia | Concurrent | Newly diagnosed MS |
| 6 | Karsidag et al.5 | F | 18 | Dizziness and imbalance | Concurrent | Newly diagnosed brain demyelinating lesions |
| F | 42 | Jaw and lt. facial pain | 1 month | Newly diagnosed brain demyelinating lesions | ||
| M | 32 | Numbness in the lt. half of jaw | 4 months | Newly diagnosed brain demyelinating lesions | ||
| 7 | Sarwar et al.12 | F | 47 | Fatigue, lt. leg and arm tingling and numbness, and lt. eye pain and blurred vision | 3 weeks | Newly diagnosed MS |
| 8 | Present case | M | 19 | Lt. finger numbness, and sudden death | 17 days | Newly diagnosed MS |
![]()
The underlying pathogenic mechanism of the flare-up of MS after COVID-19 vaccination or infection remains unclear due to small number of reported cases. Both COVID-19 vaccination and infection can induce certain immune responses and may consequently trigger the exacerbation of the preexisting MS. In addition, vaccination against COVID-19 and infection may cause rise in core body temperature for some time, which may modify the structural and physiologic conditions of the demyelinated axons of the CNS, leading to worsening of the neurological function of the MS patient. Further studies with larger cohort on the effect of COVID-19 infection and vaccines on MS pathology are needed.
Go to :
 XML Download
XML Download