

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sepsis is a life-threatening condition caused by a dysregulated host response to infection and is associated with multiorgan failure and high mortality.1 Delayed initiation of adequate antimicrobial therapy is implicated in poor patient outcomes23; thus, antimicrobials should be administered immediately after recognizing sepsis or septic shock.4 Empirical antimicrobials targeting multidrug-resistant (MDR) pathogens should be considered in high-risk patients because of their poor survival.567
Despite previous efforts,8910 no uniform tool can assess the risk of MDR pathogen. The location of onset of infection can be a risk factor for MDR pathogen, but previous studies have controversial results.1112 Moreover, recent pneumonia guidelines have abandoned the concept of “healthcare-associated” infection,1314 which included residence in long-term care facilities as a risk factor for MDR pathogen. However, in real-world practice, residence in long-term care facilities is still regarded as a significant risk factor for MDR pathogen. Therefore, local information about the resistance patterns of the causative agents of sepsis is necessary to choose the most suitable empiric therapy.4
Long-term care residents are highly likely to experience sepsis than other patients; therefore, the risk of MDR pathogens should be thoroughly evaluated.15 South Korea is famous for many long-term care facilities such as nursing homes and long-term-care hospitals. It has the highest number of long-term-care hospitals among the Organization for Economic Co-operation and Development countries.16 Long-term-care hospitals function as an intermediate facility between nursing homes and hospitals in South Korea and are experienced with simple medical care including administration of intravenous antibiotics and oxygen. Patients admitted to long-term-care hospitals have more medically complex conditions than those admitted to nursing homes,17 leading to more frequent admissions to the emergency department (ED) or the intensive care unit. In this context, we aimed to describe the antibiogram of MDR bacteria and the risk factors according to the locations of sepsis onset, including nursing homes and long-term-care hospitals.
METHODS
Study population
This study used data from an ongoing nationwide multicenter prospective observational cohort organized by the Korean Sepsis Alliance from 19 centers (13 tertiary referral centers and 6 university-affiliated general hospitals) in South Korea.18 The centers are in the central region (11 centers), southern region (6 centers), and Jeju-do (1 center) of South Korea. Details of the included centers are presented in Supplementary Fig. 1.
Patients who presented to the ED or those detected by in-hospital rapid response teams were screened for eligibility in each center. Adult patients (age ≥ 19 years) with sepsis or septic shock diagnosed according to the Third International Consensus Definition for Sepsis and Septic Shock were included.1 Patient information, including demographics, comorbidities, severity of illness, treatment, and clinical outcomes, was recorded until hospital discharge or death. Details are available from our previous studies.181920212223 To verify data quality, research committee members conducted regular audits twice a year: primarily by Asan Medical Center and then by the Center for Clinical Epidemiology of Samsung Medical Center. Any errors or discrepancies were resolved after a discussion with the investigators responsible for data collection.
Study coordinators in each center collected data prospectively using a standardized electronic case report form (http://sepsis.crf.kr/; accessed February 9, 2022).
Patient eligibility and data extraction
We included patients screened from September 1, 2019 to December 31, 2020. Patients who did not undergo blood culture were excluded from analysis. The following patient data were retrieved from the cohort: demographic data including age, sex, and body mass index; comorbidities and Charlson comorbidity index; Eastern Cooperative Oncology Group performance status (ECOG PS); location and tier of the center; suspected site of primary infection; use of initial antibiotics. Microbiological data were collected, including species and specimens used for bacterial detection. Any bacteria detected from all sample (i.e., blood culture, respiratory specimen culture, urine culture) within 48 hours of diagnosis of sepsis were included.
Definition
Patients were divided into four groups according to the location of sepsis onset: community-acquired, nursing home-acquired, long-term-care hospital-acquired, and hospital-acquired. Community-acquired infection was defined as an infection that occurred in the community setting. Nursing home- and long-term-care hospital-acquired infection were defined as infections in for those residing in such facilities before admission to the ED. Long-term-care hospitals, also known as long-term-acute care hospitals, differ from nursing homes; it is a halfway facility between nursing homes and hospitals that is capable of simple medical care such as administration of antibiotics and oxygen. Hospital-acquired infection was defined as an infection that developed any time during the hospital stay, except for long-term-care hospitals. The classification was determined according to the attending researcher in each center.
Bacteria detected from any type of specimen within 48 hours of “time zero” were considered pathogens for sepsis. “Time zero” was defined as the time of triage in the ED for patients with community-, nursing home-, and long-term-care hospital-acquired sepsis patients. For hospital-acquired sepsis, time zero was defined as the time of sepsis diagnosis by the rapid response system physician or nurse in each center.
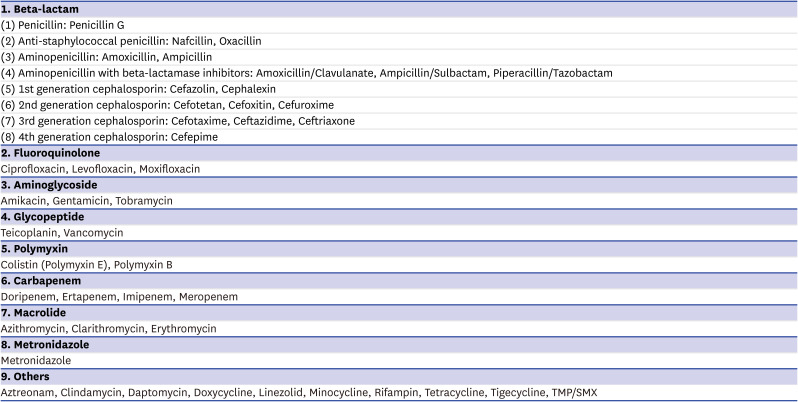
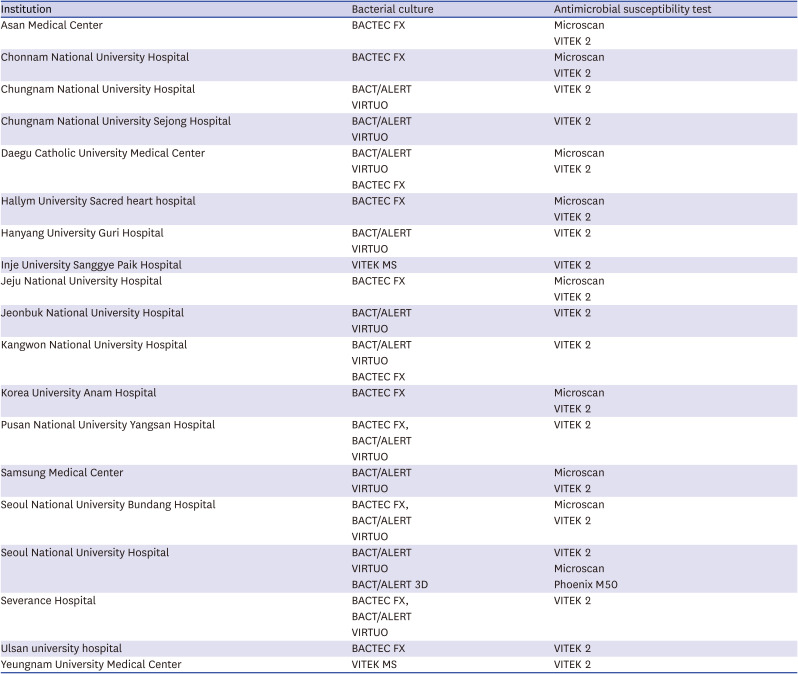
MDR was defined as bacteria resistant to at least three antimicrobial categories (Supplementary Appendix 2).24 We divided the initial antibiotics into eight categories (Supplementary Appendix 3). Carbapenem, glycopeptide, and colistin were the usual antibiotics administrated for the treatment of MDR pathogens. The drug-bug match was defined as appropriate initial antibiotics based on drug susceptibility testing results, for those with at least ≥ 1 positive bacterial culture results. The methods of bacterial culture and antimicrobial susceptibility testing of each center are described in Supplementary Appendix 4.
Statistical considerations
Categorical variables are presented as numbers with percentages and compared using chi-square test or Fisher’s exact test as appropriate. Continuous variables are presented as median with interquartile range and compared using the Kruskal-Wallis test. A logistic regression model calculated odds ratios (ORs) with 95% confidence intervals (CIs) for MDR pathogen detection. Statistically significant (P < 0.05) variables from univariate analyses were included in the multivariate analyses. Confidence intervals are presented within square brackets throughout the text. All tests were two-sided, and a P-value < 0.05 was considered significant. All statistical analyses were performed using R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) and Stata version 16 (StataCorp, College Station, TX, USA).
Ethics statement
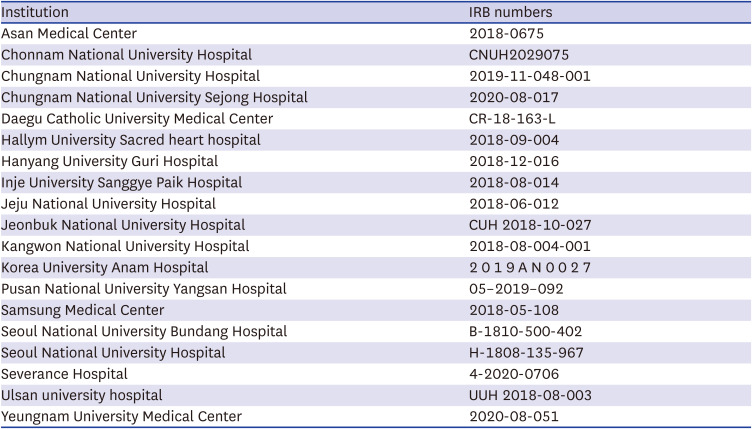
The Institutional Review Boards of each participating center approved this study (Supplementary Appendix 1). Informed consent was waived due to the noninterventional observational nature of the cohort. Our study was conducted in accordance with the amended Declaration of Helsinki.
RESULTS
Patient characteristics
A total of 7,113 patients were screened. After excluding 89 patients without blood culture results, 7,024 patients were included in this study (Supplementary Fig. 2). Sepsis was diagnosed in patients from the community (n = 3,918, 55.8%), nursing homes (n = 403, 5.7%), long-term-care hospitals (n = 926, 13.2%), and hospitals (n = 1,777, 25.3%). Patients’ median age was 73.0 years (interquartile range 62.0–81.0), with male predominance (58.4%). Common comorbidities included diabetes mellitus (35.9%), solid organ malignancy (35.6%), cardiovascular disease (24.6%), and chronic neurological disease (15.9%). Only 15.2% of patients were ECOG PS 0. The most common site of primary infection was the lung (43.6%), followed by the abdomen (28.0%) and the urinary tract (18.1%). Centers were mostly in the central region of South Korea (59.0%) and were tertiary referral centers (76.8%). Approximately 25.7% of patients used antibiotics before the onset of sepsis.
Patients with nursing home- and long-term-care hospital-acquired sepsis were older (P < 0.001), had lower body mass index (P < 0.001), and had poorer ECOG PS (P < 0.001) than those with community- and hospital-acquired sepsis. The in-hospital mortality rates were higher in patients with hospital- (31.4%), nursing home- (30.0%), and long-term-care hospital-acquired (28.6%) sepsis than in those with community-acquired (25.2%) sepsis (P < 0.001) (Table 1).
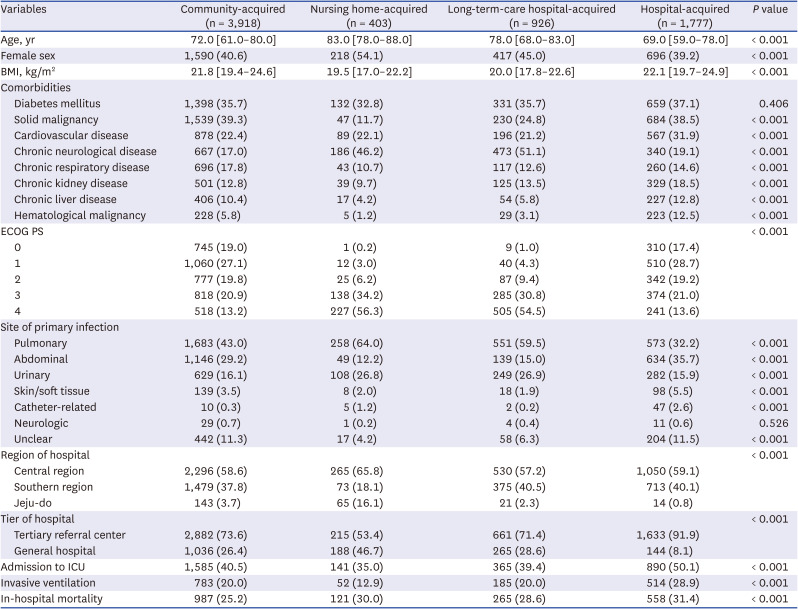
Table 1
Baseline characteristics
Numbers are presented as count (percentage) or median [interquartile range].
BMI = body mass index, ECOG PS = Eastern Cooperative Oncology Group Performance Status, ICU = intensive care unit.
![]()
Detection of bacteria
Bacteria were detected among 4,113 (58.6%) of 7,024 patients with sepsis. Gram-positive bacteria were common in patients with hospital-acquired sepsis (414 of 1,777 patients, 23.3%), whereas gram-negative bacteria were common in patients with nursing home-acquired sepsis (228 of 403 patients, 56.6%). Bacteria were mostly detected from blood culture (2,116 patients, 30.8%), urine sample (1,268 patients, 18.1%), and respiratory specimen (902 patients, 12.8%) (Table 2). The details of detected bacteria are presented in Supplementary Table 1.
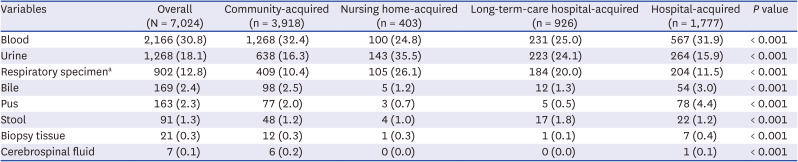
Table 2
Types of specimens of detected bacteria among sepsis patients
aRespiratory specimen culture refers to sputum, endotracheal aspirate, and bronchoalveolar lavage fluid.
![]()
MDR bacteria were detected among 1,596 (22.7%) of 7,024 patients. MDR gram-negative bacteria (n = 1,264, 18.0%) were more dominant than MDR gram-positive bacteria (n = 414, 5.9%), and 82 patients (1.2%) had both MDR gram-positive and gram-negative bacteria. The most common species were MDR Enterobacteriaceae (n = 976, 13.9%), followed by MDR Staphylococcus aureus (n = 219, 3.1%), MDR Enterococcus spp. (n = 212, 3.0%), MDR Pseudomonas spp. (n = 168, 2.4%), and MDR Acinetobacter spp. (n = 162, 2.3%).
The overall prevalence of the MDR bacteria was the highest among those with long-term-care hospital-acquired sepsis (35.9%), followed by those with nursing home- (29.5%), hospital- (26.5%), and community-acquired sepsis (17.2%) (P < 0.001). MDR gram-positive bacteria were more prevalent in patients with hospital-acquired sepsis (10.9%), followed by those with long-term-care hospital- (6.7%), nursing home- (4.2%), and community-acquired (3.6%) sepsis (P < 0.001). Meanwhile, MDR gram-negative bacteria were more commonly isolated from patients with long-term-care hospital- (30.4%) and nursing home-acquired (26.3%) sepsis, than patients with hospital- (17.6%) and community-acquired (14.4%) sepsis (P < 0.001) (Fig. 1, Table 3).
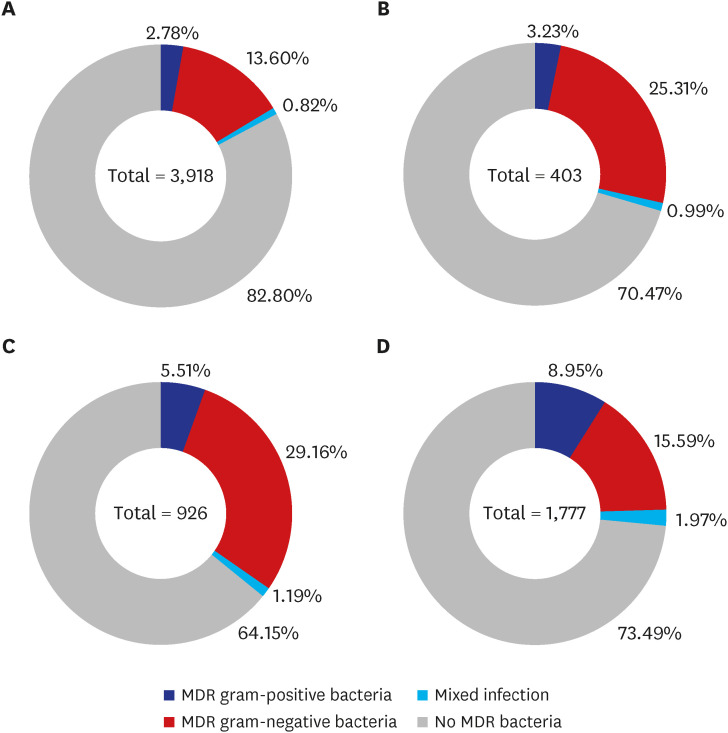
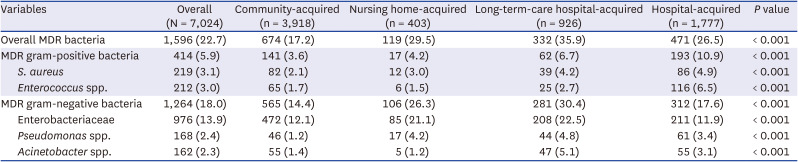
Fig. 1
Detected multidrug-resistant pathogens according to the onset of sepsis. The prevalence of multidrug-resistant pathogens differed according to the location of sepsis onset: (A) community-acquired, (B) nursing home-acquired, (C) long-term-care hospital-acquired, and (D) hospital-acquired sepsis. Long-term-care hospital- (C) and nursing home-acquired (B) sepsis revealed the highest prevalence, predominantly gram-negative bacteria.
MDR = multidrug-resistant.
![]()
Table 3
Prevalence of MDR bacteria in the overall population
![]()
We performed various subgroup analyses according to the region and tier of hospitals and the primary site of infection. The overall detection rate of MDR bacteria was 23.8% in the central region of South Korea, followed by 21.8% in Jeju-do, and 21.1% in the southern region of South Korea. The prevalence of MDR gram-negative bacteria was 21.0% in Jeju-do, 19.8% in the central region, and 15.0% in the southern region. Meanwhile, the prevalence of MDR gram-positive bacteria was 7.5% in the southern region, 5.1% in the central region, and 0.8% in Jeju-do (Fig. 2A). According to the tier of each center, general hospitals and tertiary referral centers had an overall prevalence of MDR bacteria of 21.0% and 23.2%, respectively. The prevalence of MDR gram-negative bacteria was similar (18.2% and 17.9%, respectively), whereas that of MDR gram-positive bacteria was slightly higher in tertiary referral centers (6.7%) than general hospitals (3.1%) (Fig. 2B).
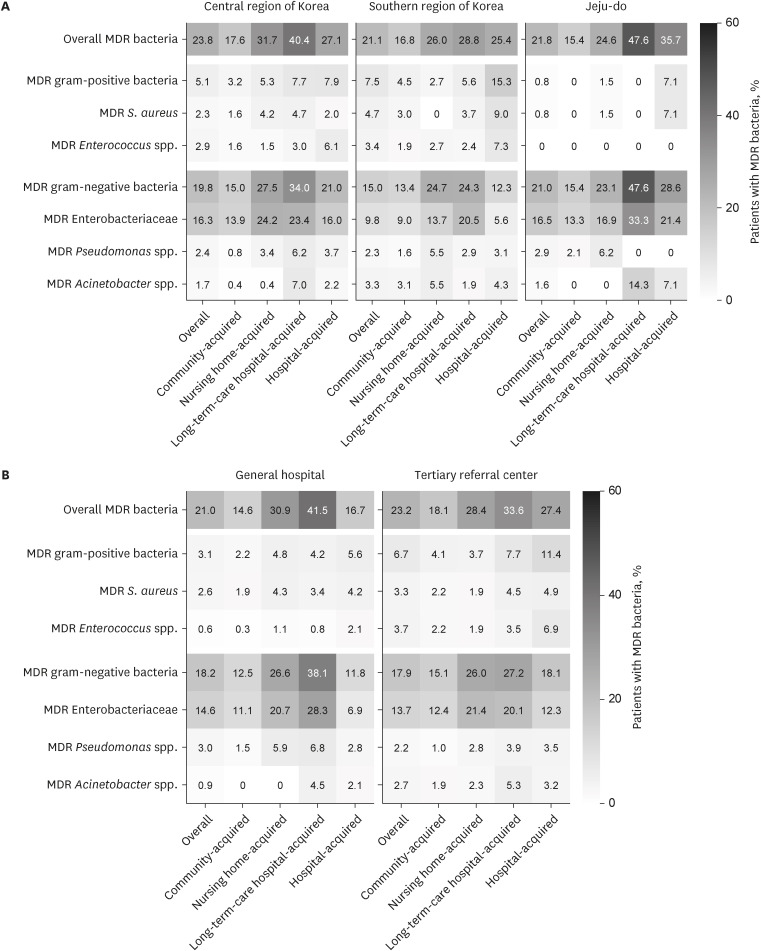
Fig. 2
Prevalence of multidrug-resistant pathogen among sepsis patients according to the region and tier of hospitals. Multidrug-resistant pathogens were most predominant in patients with long-term-care hospital-acquired sepsis regardless of the (A) region and (B) tier of each center. The central region of South Korea refers to Seoul, Gyeonggi-do, Gangwon-do, and Chungcheong-do. The southern region of South Korea refers to Jeolla-do and Gyeongsang-do. Numbers indicate the proportion of patients with MDR bacteria. Higher ratios are shown with a darker color.
MDR = multidrug-resistant.
![]()
The overall prevalence of MDR bacteria was highest in urinary tract infection (38.2%) and lowest in pulmonary infection (19.9%). The prevalence of MDR gram-positive bacteria was highest in skin or soft tissue infection (14.8%) and lowest in abdominal infection (5.4%). In contrast, the prevalence of MDR gram-negative bacteria was highest in urinary tract infection (32.0%) and the lowest in pulmonary infection (15.3%) (Fig. 3). In general, MDR gram-negative bacteria were dominant in patients with long-term-care hospital-acquired sepsis, whereas MDR gram-positive bacteria were dominant in patients with hospital-acquired sepsis.
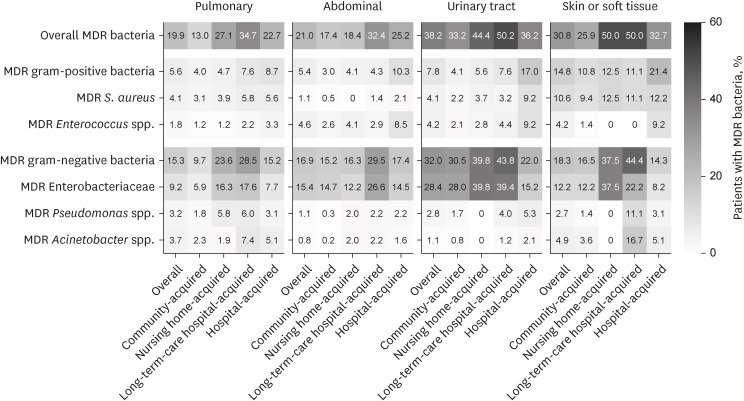
Fig. 3
Prevalence of multidrug-resistant pathogen among sepsis patients according to the primary site of infection. Multidrug-resistant pathogens were most predominant in patients with long-term-care hospital-acquired sepsis regardless of the primary site of infection. Patients with urinary tract infection had the highest rate of MDR gram-negative infection, whereas those with skin or soft tissue infection had the highest rate of MDR gram-positive bacteria. Higher ratios are shown with a darker color.
MDR = multidrug-resistant.
![]()
Risk factors for MDR bacteria
Variables including patient demographics, comorbidities, ECOG PS, site of primary infection, centers’ region and tier, use of antibiotics before sepsis, and onset settings were used to assess the risk factors for MDR pathogen. Compared with community-acquired sepsis, nursing home- (adjusted OR, 1.63; 95% CI, 1.26–2.12), nursing hospital- (adjusted OR, 2.06; 95% CI, 1.70–2.50), and hospital-acquired (adjusted OR, 1.45; 95% CI, 1.23–1.71) sepsis had a higher risk of MDR pathogen after multivariate adjustment. The nursing hospital-acquired group had the highest risk of MDR pathogen detection, with a significantly higher risk than the hospital-acquired sepsis group (adjusted OR, 1.42; 95% CI, 1.15–1.75). Other than the onset of sepsis, underlying cardiovascular disease (adjusted OR, 1.18; 95% CI, 1.02–1.36), chronic neurological disease (adjusted OR, 1.18; 95% CI, 1.02–1.37), immune-compromised status (adjusted OR, 1.67; 95% CI, 1.25–2.25), poorer ECOG PS, abdominal infection (adjusted OR, 1.34; 95% CI, 1.12–1.61), urinary tract infection (adjusted OR, 2.88; 95% CI, 2.40–3.45), skin or soft tissue infection (adjusted OR, 2.13; 95% CI, 1.57–2.90), and use of antibiotics before the diagnosis of sepsis (adjusted OR, 1.33; 95% CI, 1.15–1.55) were all associated with the higher risk of MDR pathogen (Table 4).
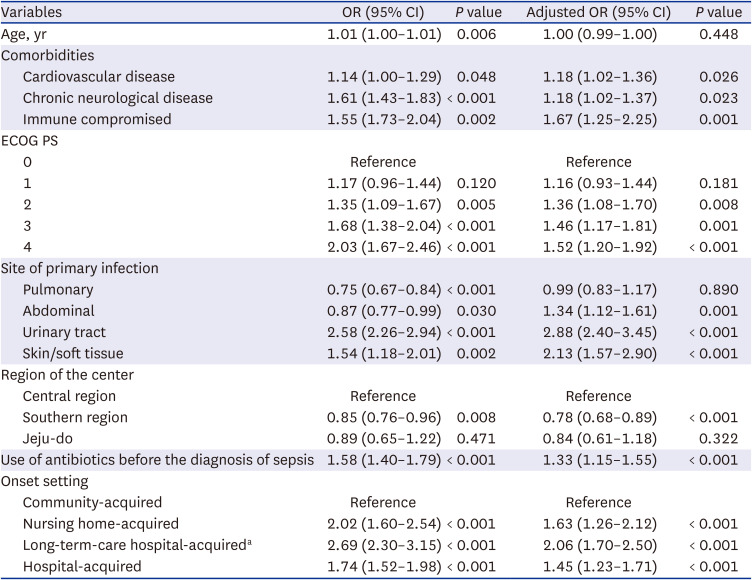
Table 4
Risk factors for detection of multidrug-resistant pathogen in sepsis patients
Numbers are presented with odds ratio with 95% confidence intervals.
OR = odds ratio, CI = confidence interval, ECOG PS = Eastern Cooperative Oncology Group Performance Status.
aSignificantly higher risk than hospital-acquired sepsis (adjusted OR, 1.42; 95% CI, 1.15–1.75).
![]()
We performed a sensitivity analysis since the information about recent hospitalization within 90 days, antibiotics or chemotherapy within 30 days, and wound care within 30 days was only available from 5,027 patients who presented via the ED. After adjustment of additional factors including recent hospitalization (< 90 days), recent administration of antibiotics or chemotherapy (< 30 days), and recent wound care (< 30 days), patients with nursing home- and long-term-care hospital-acquired sepsis had a persistently higher risk of MDR pathogen than patients with community-acquired sepsis (adjusted OR, 1.59; 95% CI, 1.22–2.08; and 1.62, 95% CI, 1.31–2.00, respectively) (Supplementary Table 2).
The risk factors for MDR gram-positive and gram-negative factors were also analyzed. After multivariate analysis, urinary tract infection (adjusted OR, 1.45; 95% CI, 1.12–1.87), skin or soft tissue infection (adjusted OR, 2.53; 95% CI, 1.72–3.74), southern region of South Korea (adjusted OR, 1.48; 95% CI, 1.17–1.89, compared to the central region), tertiary referral center (adjusted OR, 1.73; 95% CI, 1.25–2.39), and hospital-acquired sepsis (adjusted OR, 2.18; 95% CI, 1.67–2.85; compared with community-acquired sepsis) were significant risk factors for MDR gram-positive bacterial detection (Supplementary Table 3). For the MDR gram-negative bacteria, urinary tract infection (adjusted OR, 2.41; 95% CI, 2.06–2.83), central region of South Korea (adjusted OR, 1.55; 95% CI, 1.34–1.80; compared with the southern region), nursing home- and long-term-care hospital-acquired sepsis (adjusted OR, 1.66; 95% CI, 1.26–2.18; and 2.15, 95% CI, 1.75–2.63]; respectively, compared with community-acquired sepsis) were significant risk factors (Supplementary Table 4).
Antibiotics use
As an initial antibiotic, β-lactam was most commonly used (74.6%), followed by fluoroquinolone (31.1%), carbapenem (28.2%), and glycopeptide (18.1%). The antibiotics usually administered for the treatment of MDR pathogens, such as carbapenem, glycopeptide, and colistin, were more commonly used in patients with hospital-acquired sepsis (50.6%, 39.4%, and 2.4%, respectively) than in other groups. Furthermore, patients with hospital-acquired sepsis received a combination of two or more antibiotics more frequently (70.1%) than those with the community-, nursing home-, and long-term-care hospital-acquired sepsis (57.0%, 51.6%, and 59.7%, respectively) (Supplementary Table 5).
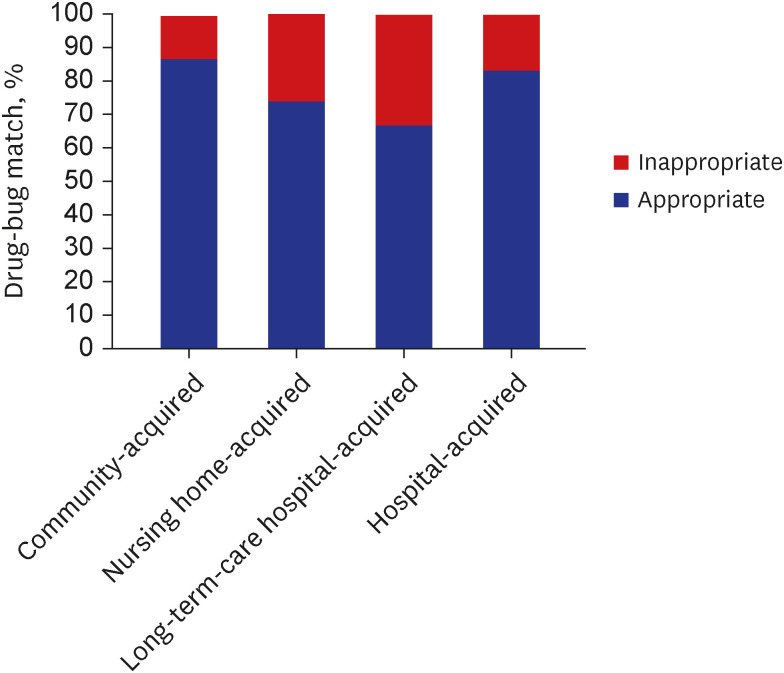
The evaluation of drug-bug match of initial antibiotic administration showed a higher match in community- (86.4%) and hospital-acquired (83.1%) sepsis, whereas that of nursing home- (73.9%) and long-term-care hospital-acquired (66.8%) sepsis was much lower (P < 0.001) (Fig. 4).
DISCUSSION
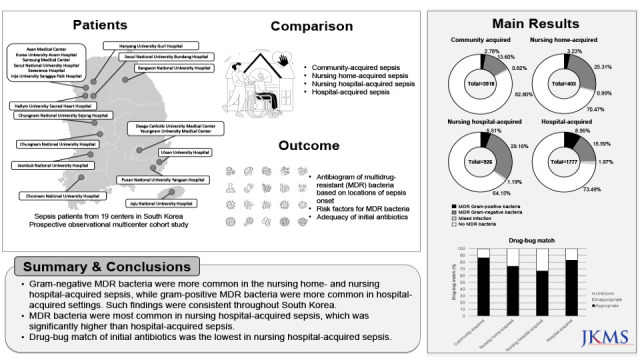
This was the first large-scale multicenter study to investigate the prevalence of MDR bacteria among sepsis patients in various onset locations. MDR bacteria were detected in 22.7% of patients, and long-term-care hospital-acquired sepsis had the highest prevalence of MDR pathogen. The results were consistent regardless of the centers’ region and tier. Sepsis acquired from long-term-care hospitals and nursing homes were independent risk factors for detecting MDR bacteria. The strength of our study is that it is a well-established multicenter cohort study from various regions across the country, including detailed information about detected microorganisms, resistance patterns, and antibiotics use.
The present study showed a predominance of gram-negative bacteria among sepsis patients in South Korea. Such a finding is novel, but it is also in agreement with previous reports from Asia. In a multinational cross-sectional study from Southeast Asia, Escherichia coli was the most common pathogen of sepsis.25 A systematic review of 17 studies from South and Southeast Asia reported that gram-negative bacteremia was more common than gram-positive bacteremia.26 Recently, the proportion of gram-negative bacteria has been increasing in intensive care units in western countries.2728 Special attention is required for this gram-negative sepsis, considering the higher levels of inflammatory biomarkers such as C-reactive protein and procalcitonin,2930 and pro-inflammatory cytokines, such as tumor necrosis factor-α, interferon-γ, and interleukins 8, 4, and 10 than those in gram-positive sepsis.31 Sepsis caused by gram-negative bacteria is accompanied by the release of endotoxin from bacteria, inducing inflammatory cells to express proinflammatory cytokines. Acute exposure to endotoxins may lead to life-threatening sepsis.32 Gram-negative bacteria also reveal high rates of antimicrobial resistance. Of the ESKAPE (Enterococci, S. aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp.) pathogens known to have antimicrobial resistance, the majority consists of gram-negative bacteria.33 In particular, extended-spectrum beta-lactamase-positive Enterobacteriaceae is one of the most common MDR bacteria causing sepsis.34 Such characteristics of the MDR gram-negative bacteria have been associated with high mortality rates (30–70%).35 Fortunately, novel drugs targeted against such MDR gram-negative bacteria are being developed.36 Further national support regarding antimicrobial stewardship and infection control is needed to reduce the spread of MDR gram-negative bacteria.37
Our results showed significantly higher rates of MDR bacteria among sepsis patients from long-term care facilities. This can be explained as follows. First, residents of nursing homes and long-term-care hospitals can be living reservoirs for MDR bacteria, and they frequently move around the health care network, leading to a high risk of MDR bacterial colonization and transmission.38 Moreover, patients often have invasive medical devices such as urinary catheters and feeding tubes, which break the natural physical barrier. These patients have histories of frequent ED visits or critical illness,1539 which is a potential risk for MDR bacterial colonization.101738 The influx of MDR bacteria from long-term care facilities to hospitals have been suggested in several studies from South Korea. A surveillance study performed in long-term care facilities suggested that the prevalence of extended-spectrum beta-lactamase-producing E. coli and K. pneumoniae is approximately 45%.40 Approximately one-third of patients transferred from long-term care facilities to hospitals carried MDR organisms,41 and patients with MDR gram-negative bacteria within 48 hours of hospital admission had a higher rate of mortality.42 Second, poor adherence to personal protective equipment, cleaning, and disinfection in long-term care facilities can contribute to the high MDR risk.43 In a previous study from the United States, the prevalence of MDR pathogens was estimated to have a median of 65% in nursing homes and 80% in long-term acute care facilities from random samples,44 which is remarkably higher than what we anticipate in real-world practice. The underestimation of MDR bacteria is reflected in our study as well: almost twice as many antibiotics were inadequate in patients with nursing home- and long-term-care hospital-acquired sepsis than those with community- and hospital-acquired sepsis.44
The detailed reason for the polarized distribution of MDR gram-positive and gram-negative bacteria according to the onset location of sepsis is beyond the scope of our study but requires some explanations. The different sites of primary infection may play a role. Skin or soft tissue infection was more prevalent in hospital-acquired sepsis than in the nursing home- and long-term-care hospital-acquired sepsis. In our multivariate analyses, skin or soft tissue infection (adjusted OR, 2.53; 95% CI, 1.72–3.74) was a significant risk factor for the detection of MDR gram-positive bacteria. On the contrary, the rate of urinary tract infection was significantly higher in nursing home- and long-term-care hospital-acquired sepsis than that in hospital- and community-acquired sepsis. Urinary tract infection was a risk factor for the detection of both MDR gram-positive (adjusted OR, 1.45; 95% CI, 1.12–1.87) and gram-negative (adjusted OR, 2.41; 95% CI, 2.06–2.83) bacteria, but the adjusted OR was higher in gram-negative bacteria. Simple regional differences of MDR bacteria may also contribute to the polarized distribution. MDR gram-positive bacteria were more prevalent in the southern region of South Korea, of which nursing home-acquired sepsis cases were significantly fewer than in other regions, whereas MDR gram-negative bacteria were more prevalent in the central region, of which nursing home-acquired sepsis cases were more common.
Based on our study, we suggest that MDR pathogens should be considered according to each patient’s characteristics of sepsis. Patients from nursing homes and long-term-care hospitals, especially those with suspected urinary tract infections should be considered at risk for MDR gram-negative bacterial sepsis. Patients with hospital-acquired sepsis, especially those with skin or soft tissue infection, should be considered at risk for MDR gram-positive bacterial sepsis. In the surviving sepsis guideline,4 using empirical antimicrobials against MDR organisms at increased risk for such pathogens is recommended because adequate antibiotic use is the most critical issue.4546 Because no uniform recommendation can be made, regional information about the resistance patterns of sepsis pathogens is necessary to select the most effective empirical antibiotic regimen. In such context, our study findings provide real-world data about the distribution of MDR pathogens according to the onset location of sepsis. In addition, further efforts are needed to reduce the prevalence of MDR bacteria in long-term care facilities. According to the results of our study, special attention should be paid for those at risk for urinary tract infection.
Despite our meaningful findings, this study has several limitations. First, bacteremia was confirmed in only 30.8% of patients. However, blood culture has shown variable sensitivities in previous reports,4748 and negative results from blood cultures should not exclude the possibility of sepsis by an MDR pathogen. Second, certain risk factors for MDR pathogens, such as a history of recent hospitalization, administration of antibiotics or chemotherapy, and wound care, were not documented for patients with hospital-acquired sepsis. We performed a sensitivity analysis to address this issue, which was concordant with our main results. Third, our study was based on sepsis patients who visited tertiary referral or university-affiliated general hospitals and does not represent the overall population. Further studies are required to inspect the prevalence of MDR pathogens in long-term care facilities. Fourth, we could not acquire bacterial information to the species level except for S. aureus. Further studies on clinically important species such as carbapenem-resistant Enterobacteriaceae, vancomycin-resistant Enterococcus, and imipenem-resistant A. baumannii are needed.
In conclusion, the prevalence of MDR bacteria was highest in sepsis patients from long-term-care hospitals, and it was significantly higher than in patients with hospital-acquired sepsis. When administrating initial antibiotics, MDR gram-negative bacteria should be considered for sepsis patients from long-term-care hospitals or nursing homes, whereas MDR gram-positive bacteria should be considered for those with hospital-acquired sepsis. Considering the low drug-bug match of initial antibiotics in nursing home- and long-term-care hospital-acquired sepsis, antibiotics targeting MDR gram-negative pathogens can be considered in selected patients from these facilities. Efforts and further research are needed to reduce the prevalence of MDR bacteria in long-term care facilities.
 XML Download
XML Download