

 PDF
PDF Citation
Citation Print
Print



The cases of severe acute hepatitis of unknown etiology in children were reported on March 3, 2022 in central Scotland.1234 It has been also observed from the U.S. with cases since October 1, 2021.5 World Health Organization (WHO) reported probable cases according to the WHO working case definitions; acute hepatitis (non-hepatitis viruses A, B, C, D, and E) with serum transaminase greater than 500 IU/L (alanine aminotransferase or aspartate aminotransferase), and jaundice in children 16 years old and younger since October 1, 2021.3 As of May 26, 2022, WHO reported 650 cases from 33 countries; mainly 222 (34%) in the U.K. and Northern Ireland, 216 (33%) the U.S., and several countries.6 Amongst them, 38 (6%) received liver transplantation, and nine (1%) died.6 In terms of etiology, adenovirus has been detected in a significant proportion of the patients.678 The Korea Disease Control and Prevention Agency (KDCA) started nationwide surveillance for acute hepatitis of unknown etiology since May 2022.9
Respiratory adenovirus and enteric adenovirus infection data were extracted from KDCA weekly surveillance report from January 1, 2017 to July 2, 2022.10 The number of sentinel hospitals for viral surveillance was maintained as the same at 208 hospitals, and the number of reporting hospitals was similar from 2021 to 2022 (Table 1).
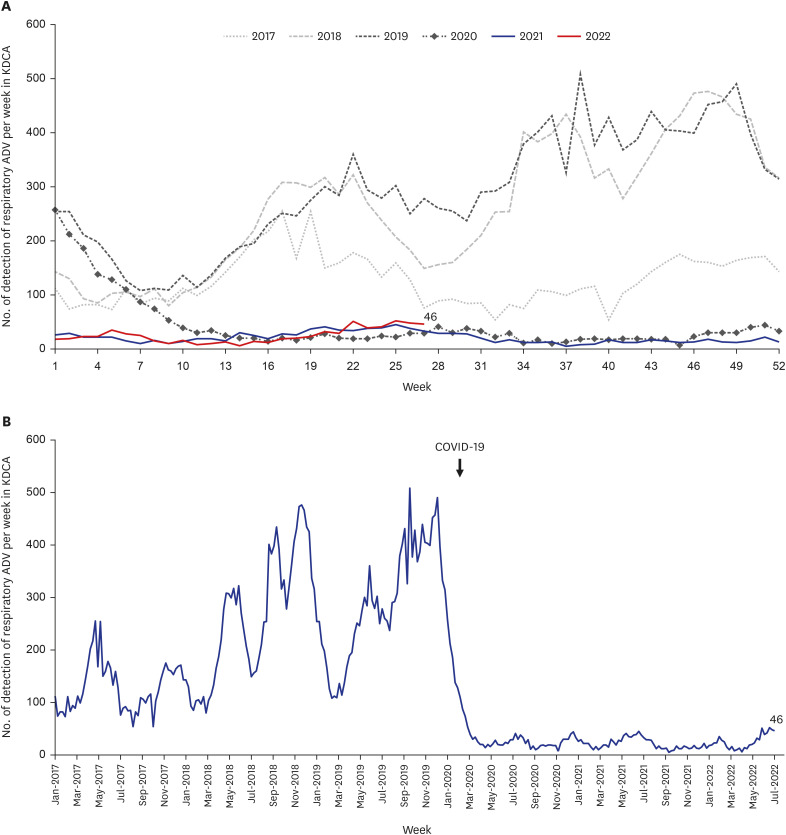
Respiratory adenovirus infection occurred throughout the year, and 100–500 cases per week were reported until 2019. When compared between 2017 and 2018–2019 period, it appeared that more cases were reported in the years 2018 and 2019 (Fig. 1A). With coronavirus disease 2019 (COVID-19) pandemic, respiratory adenovirus infection significantly decreased from its usual number in January 2020, and the reported numbers were low at around 30 cases per week. However, the respiratory adenovirus infection has been gradually increasing to around 50 cases per week since week 22 in May 2022 (Fig. 1B).
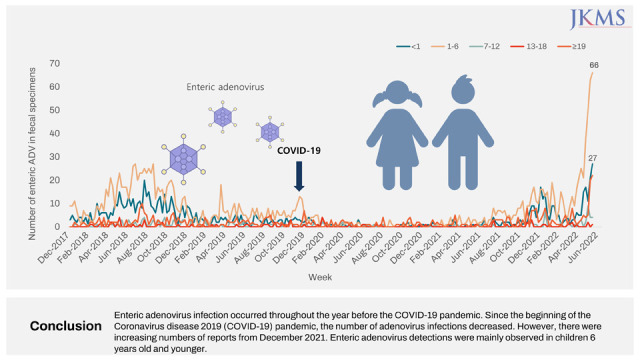
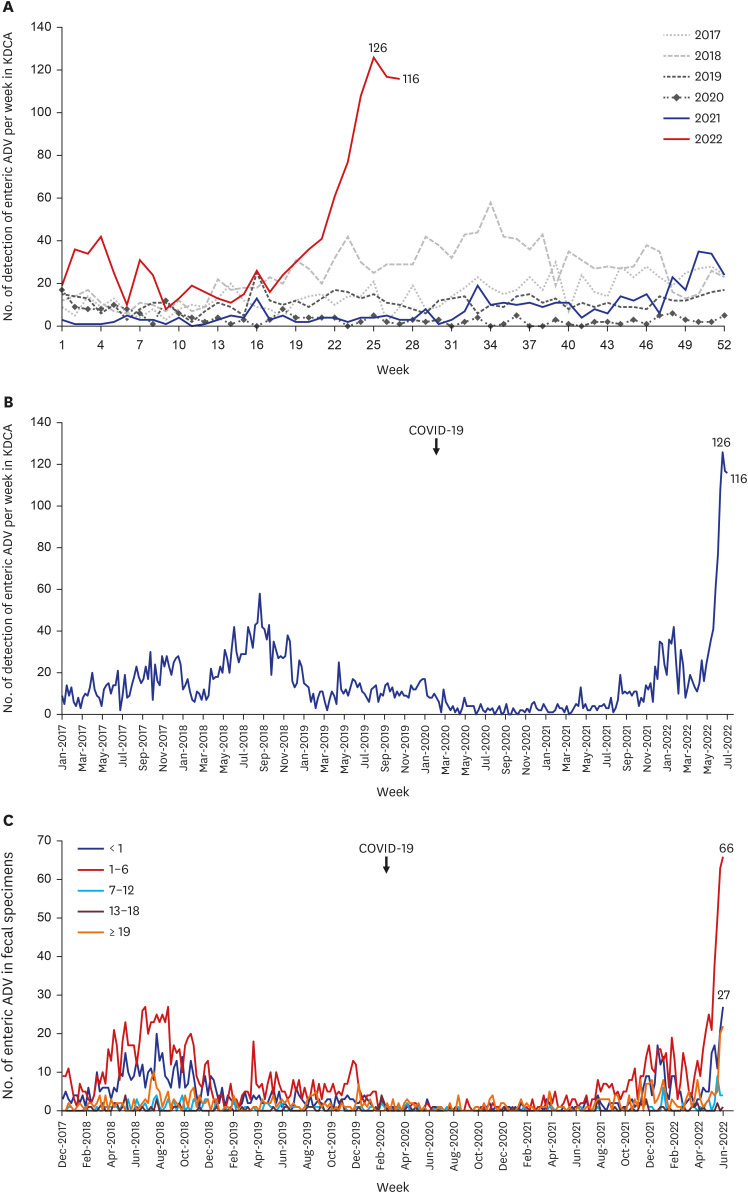
Enteric adenovirus infection, similar to respiratory adenovirus infection, occurred throughout the year before the COVID-19 pandemic (Fig. 2A). Enteric adenovirus infection was reported in around 10–20 cases per week except in 2018 when as high as 50 cases were reported during the summer months (Fig. 2A). Since the beginning of the COVID-19 pandemic, the number of enteric adenovirus infections decreased below 5 cases per week and was maintained low in 2020 and the first half of 2021. However, there was a signal of increasing numbers of reports in December 2021 and early 2022 (Fig. 2B). As of July 2, the number of enteric adenovirus infections has been continuously increasing and reached the highest number of 126 cases at week 25 in June during the study period (Fig. 2B). We additionally analyzed the reported enteric adenovirus cases by age group (under one year of age, 1–6 years of age, 7–12 years of age, 13–18 years of age, and 19 years of age) from January 1, 2018 to June 18, 2022. From December 2021–June 2022, enteric adenovirus detections were increasing mainly in children six years old and younger. The peak number was 66 cases for the 1–6-year-old age group at week 25 in 2022, followed by 27 cases for children under one year of age group (Fig. 2C). There is no information available for specific adenovirus types.
As of May 19, 2022, U.K. Health Security Agency (UKHSA) reported adenovirus-positive cases from the fecal or gastrointestinal specimens in England from January 2018 to May 15, 2022.7 In particular, significant changes were observed in 4 years of age and under. Adenovirus-positive cases were observed at 40–50 cases per week for 1–4 years of age, and around 30 cases per week for those under one year of age, before the COVID-19 pandemic.7 With the COVID-19 pandemic, April 2020–June 2021, the adenovirus detections were reported below 10 cases by all age groups.7 Adenovirus cases gradually increased from May–July 2021, rapidly increased from October 2021, and peaked at 150 cases for 1–4 years of age and 130 cases for those under one year of age, respectively.7 As of June 13, UKHSA reported 260 cases of acute hepatitis of unknown etiology in children under 16 years old; amongst them, 241 cases were tested for adenovirus, and 156 (64.7%) cases were positive for adenovirus.11 Thirty-five cases were tested for typing by partial hexon gene sequencing in blood, and in 27 (77%) patients, adenovirus 41F was detected.7
In the U.S., as of June 22, 2022, 305 cases were reported in children under ten years of age since October 1, 2021. Of the 252 cases who received adenovirus test, 113 (45%) cases were positive for adenovirus at least in one specimen, such as blood, respiratory, or stool specimens.8 In 20 cases, adenovirus typing was performed, and adenovirus 41 was the most commonly detected (n = 13) and followed by adenovirus type 1 (n = 3), type 2 (n = 1), type 5 (n = 1), type 6 (n = 1) and type 40 (n = 1).8
Adenovirus is one of the common causes of upper respiratory tract infections, and enteric adenovirus is an important pathogen of gastroenteritis in children.12 Although it is not clear whether the enteric adenovirus is the major responsible pathogen for the current increase in acute hepatitis of unknown etiology in children worldwide, careful monitoring for adenovirus infection is crucially important for the next coming months with well-maintaining surveillance. Unlike the U.S., or U.K. where increased cases alerted clinicians in the field since late 2021 or early 2022, there seems to be no significant increase in Korea and the reason is not clear. However, since the surveillance has started, further information is expected to be available later.
Taking into account the severity of the acute hepatitis of unknown origin in children and the urgent need for epidemiological situation worldwide, we report the changes in the epidemiology of adenovirus in Korea from January 2017 to early July 2022 to be used as a reference in the future.

 XML Download
XML Download