

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Antiplatelets and anticoagulants have been widely adopted into everyday clinical practice. Aspirin is an anti-inflammatory and antiplatelet agent with effects mediated through irreversible inhibition of cyclooxygenase 1 and 2 (COX1 and COX2). Adenosine diphosphate (ADP) receptor blockers inhibit platelet aggregation by preventing the binding of ADP to its specific platelet receptor. Newer agents (clopidogrel, prasugrel, and ticagrelor) are routinely prescribed as part of a dual antiplatelet therapy regimen in patients with ischemic heart disease [1]. Aspirin and clopidogrel are the most common agents in cardiovascular disease for primary and secondary prevention [2]. Warfarin was used for prophylaxis and treatment of venous thrombosis and its extension, pulmonary embolism. In addition, it could be adopted for prophylaxis and treatment of thromboembolic complications associated with atrial fibrillation and cardiac valve replacement. Recently, direct oral anticoagulants (DOACs) are used in patients with nonvalvular atrial fibrillation (AF) and for the treatment and prevention of venous thromboembolism [3]. Due to rapid onset/offset of action, few drug interactions and predictable pharmacokinetics, the use of these agents is increasing; therefore, surgeons are encountering patients who are on antiplatelets and/or anticoagulant therapy during perioperative periods [4].
Postoperative major bleeding is a rare but dangerous complication in patients who underwent laparoscopic gastric cancer surgery. Surgical site major bleeding is unexpected and causes hemodynamic instability [5]. According to the literature, the estimated rate of hemorrhagic complications following gastrectomy was 0.9% (in a series of more than 1,500 patients), with a mortality rate of 20%. As a treatment, 80% of patients initially undergo endovascular intervention with an 80% success rate [6]. If the initial treatment fails, surgeons should quickly move to secondary interventions including transfusion, endoscopic intervention, or explorative laparotomy. Therefore, for the safety of the patient who has been using antiplatelets and/or anticoagulation, it is important to investigate the postoperative major bleeding risk.
However, there are many controversies over the relationship between the use of antiplatelets and/or anticoagulants and the risk of major postoperative bleeding [78910]. In addition, there was no study in which the cohort was limited to laparoscopic gastrectomy. Therefore, we investigated the association of antiplatelet agents and anticoagulants with postoperative major bleeding risk after laparoscopic gastric cancer surgery.
Go to : 
METHODS
Design and ethical statement
This study is based on retrospective analysis. The study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-1907-552-104). We followed the STROBE (Strengthening the Reporting of Observational Studies in the Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for reporting on observational cohort studies. Informed consent was not required due to the retrospective nature of the study.
Patient selection
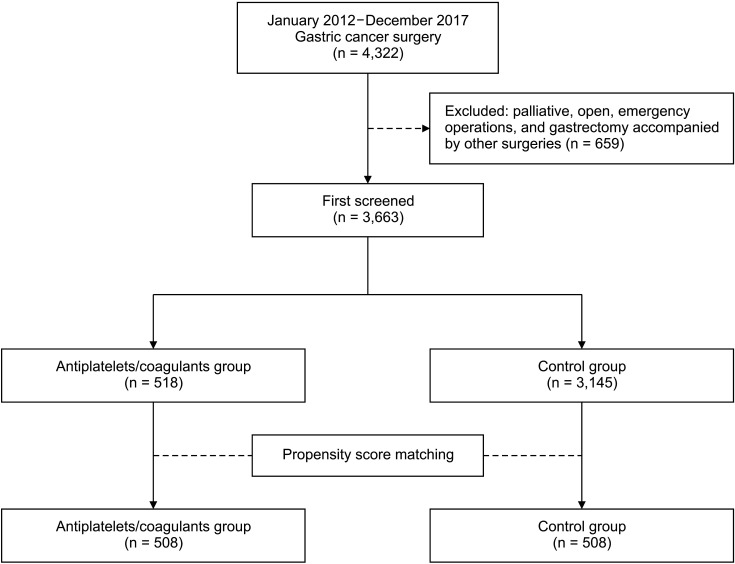
From January 2012 to December 2017, 4,322 patients underwent gastrectomy for gastric cancer in our institute. Of these, 659 cases of palliative, open, emergency operations, and gastrectomy accompanied by other surgery were excluded from the analysis. Consequently, 3,663 patients who underwent curative laparoscopic gastrectomy were enrolled in this study, among which 518 patients belong to the antiplatelets/anticoagulants group and 3,145 patients belong to the control group. After propensity score matching (PSM), a total of 1,016 patients (508 patients in each group) were included in the analysis (Fig. 1).
Data collection
We obtained data from the electronic medical records of all patients. A clinical data warehouse application was used for data retrieval and analysis. We collected the data of physical characteristics (sex, age [years], body mass index [BMI, kg/m2]), lab related to hemostasis (platelet [×103/µL], PT, international normalized ratio [INR], aPTT [sec]), American Society of Anesthesiologists (ASA) physical status (PS) classification, comorbidity, TMN stage, resection type, combined resections, lymphadenectomy, operation time, hospital day, and postoperative intensive care unit (ICU) care.
Outcome measure
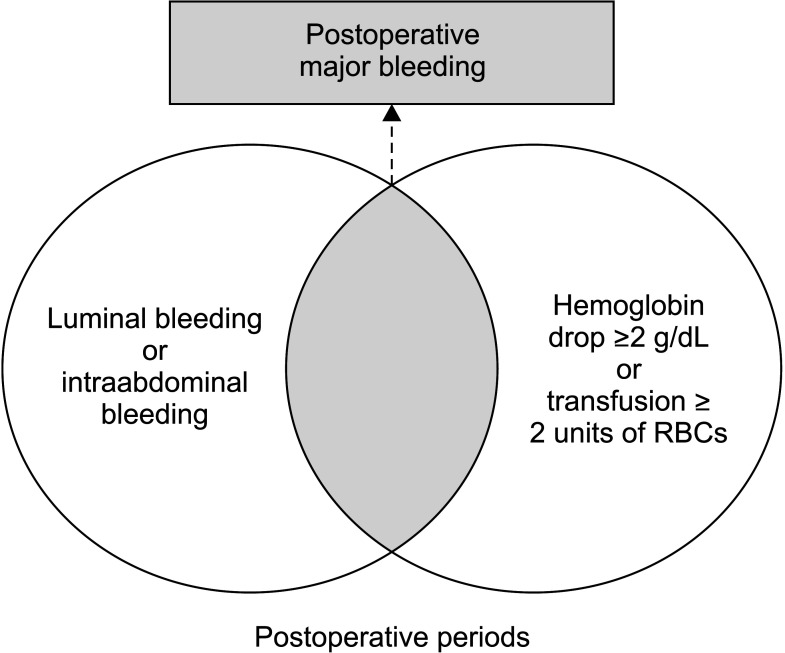
The primary outcome was postoperative major bleeding which is defined that intraluminal bleeding or intraabdominal bleeding with fall in hemoglobin level of at least 2 g/dL (1.24 mmol/L), or transfusion, indicated by the bleeding, of at least 2 units of RBCs, with temporal association within 24 hours to the bleeding (Fig. 2) [5]. Intraluminal bleeding was diagnosed by hematochezia, melena, hematemesis, or endoscopic findings. Intraabdominal bleeding was diagnosed by sanguineous drainage via Jackson-Pratt closed suction drain, hemoperitoneum, hematoma, or extravasation of contrast material on CT scan. The secondary outcomes were early complication rate and intraoperative and postoperative transfusions, which did not meet the definition of major bleeding. Administration of RBCs during surgery was defined as intraoperative transfusion. If RBCs were transfused within 2 days after surgery, we considered it as a postoperative transfusion. Early complication was defined as any deviation from the ideal postoperative course that was not inherent in the procedure and did not comprise a failure to cure [11] in postoperative 30 days. This was graded by Clavien-Dindo classifications [12].
Statistical analysis
Baseline characteristics were presented as the mean value ± standard deviation for continuous variables or number (percentage) for the categorical variables. Categorical variables were compared using the chi-square test; Student t-test was used to compare continuous data. PSM was performed using MatchIt package in the R program (R Foundation for Statistical Computing). Covariates in the model for propensity scores included sex, age, BMI, ASA PS grade, comorbidity, TMN stage, resection type, combined resection, and lymphadenectomy. Univariable logistic regression analysis was initially conducted to investigate the individual association of all covariates with postoperative major bleeding. Next, covariates with a P-value of <0.2 in the univariable model were entered into the backward stepwise regression model. All results of the logistic regression model were provided as odds ratios (ORs) with 95% confidence intervals (CIs). Goodness of fit in each multivariable model was confirmed by Hosmer-Lemeshow statistic test with a criterion of P > 0.05. There was no multicollinearity issue in each multivariable model with variance inflation factor of <2.0. All statistical analyses were performed using IBM SPSS Statistics ver. 20.0 (IBM Corp., Armonk, NY, USA) and the R program.
Go to :
RESULTS
Results from entire cohort analysis
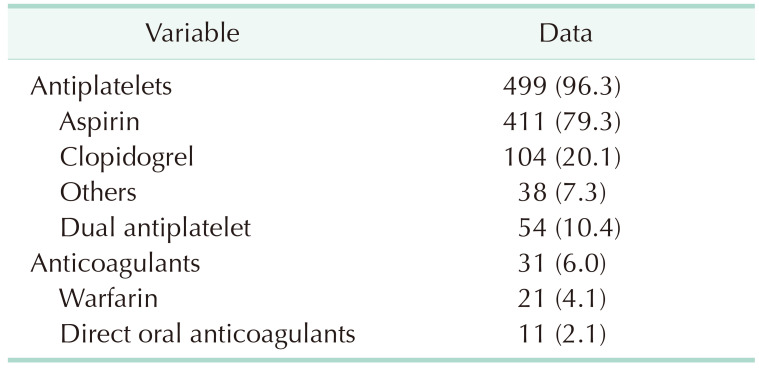
Among 3,663 patients in the entire cohort, 518 (14.1%) patients were on antiplatelet and/or anticoagulant therapy. Four hundred ninety-nine patients (96.3%) were on antiplatelets and 31 (6.0%) were on anticoagulation. Aspirin (79.3%) was the most used medication, followed by clopidogrel (20.1%) and other antiplatelet agents (7.3%) (Table 1).
In the antiplatelets/anticoagulants group, the proportion of male patients was higher (380 [73.4%] vs. 2,007 [63.8%], P < 0.001) and mean age was older (69.09 ± 8.45 years vs. 59.38 ± 12.47 years, P < 0.001). Antiplatelets/anticoagulants group showed higher BMI (24.97 ± 3.72 kg/m2
vs. 23.80 ± 3.35 kg/m2), lower platelet counts (240.52 ± 67.56 vs. 250.66 ± 65.82; unit: ×103/µL), higher PT (1.03 ± 0.108 vs. 1.01 ± 0.07), more ASA PS grades over II (500 [96.5%] vs. 1,724 [54.8%]), and more comorbidities (517 [99.8%] vs. 2,108 [67.0%]) (P < 0.001). In the antiplatelets/anticoagulants group, distal gastrectomy was performed in 73.7%, total gastrectomy in 13.9%, proximal gastrectomy in 7.5%, pylorus-preserving gastrectomy (PPG) in 2.9%, and segmental resection in 1.9% of patients. Meanwhile, for the control group patients, distal gastrectomy was performed in 72.4%, total gastrectomy in 14.7%, proximal gastrectomy in 5.5%, PPG in 5.6%, and segmental resection in 1.8 % of patients (P = 0.048). The mean days of hospital stay (7.32 ± 6.08 vs. 6.56 ± 7.75, P = 0.033) and postoperative ICU care (70 [13.5%] vs. 121 [3.8%], P < 0.001) were significantly different between the 2 groups. However, there were no significant differences in TNM stage, combined resection, lymphadenectomy, and operation time. Patients were propensity score matched to generate an analysis cohort with minimal differences in these baseline characteristics (Table 2).

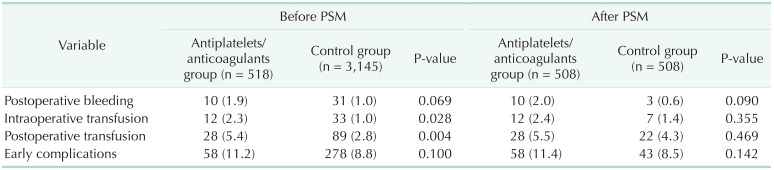
Before PSM, 10 cases of postoperative major bleeding (1.9%) were observed in the antiplatelets/anticoagulants group, an insignificant difference from the control group (31 [1.0%]) (P = 0.069). Intraoperative and postoperative transfusion rates were significantly higher in the antiplatelets/anticoagulants group than in the control group (12 [2.3%] vs. 33 [1.0%], P = 0.028; 28 [5.4%] vs. 89 [2.8%], P = 0.004). Early complications developed in 58 patients (11.2%) in the antiplatelets/anticoagulants group and 278 (8.8 %) in the control group (P = 0.100) (Table 3). The mean amounts of intraoperative and postoperative transfusions were not significantly different between the 2 groups (366.67 ± 238.68 mL vs. 484.85 ± 287.36 mL, P = 0.210; 728.57 ± 642.25 mL vs. 676.40 ± 613.12 mL, P = 0.699) (Table 4).

Results from propensity score matching cohort analysis
After PSM, 2 groups of 508 patients, homogenous for sex, age, BMI, platelet, PT, aPTT, ASA PS grade, comorbidity, TMN stage, resection type, combined resection, and lymphadenectomy were extracted. Postoperative major bleeding was not significantly higher in the antiplatelets/anticoagulants group (10 [2.0%] vs. 3 [0.6%], P = 0.090). Intraoperative transfusion and postoperative transfusions were not significantly higher in the antiplatelets/anticoagulants group than in the control group (12 [2.4%] vs. 7 [1.4%], P = 0.355; 28 [5.5%] vs. 22 [4.3%], P = 0.469). Early complications did not show significant differences between the 2 groups (58 [11.4%] vs. 43 [8.5%], P = 0.142) (Table 3). The mean amounts of intraoperative and postoperative transfusions were not significantly different between the 2 groups (366.67 ± 238.68 mL vs. 371.43 ± 138.01 mL, P = 0.962; 728.57 ± 642.25 mL vs. 508.09 ± 468.95 mL, P = 0.185) (Table 4).
Risk factors for the postoperative major bleeding risk
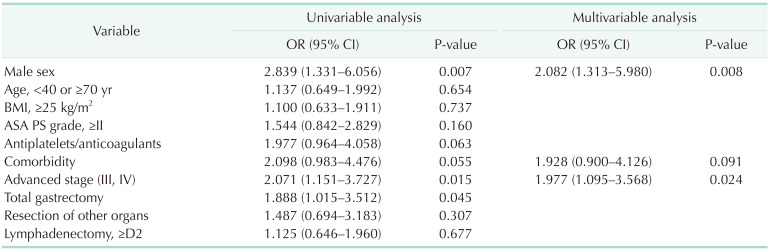
Univariable and multivariable analyses for investigating risk factors for postoperative major bleeding were conducted. In univariable analysis, male sex, advanced stage (III, IV), and total gastrectomy were associated with postoperative major bleeding. However, using multivariable analysis, male sex (OR, 2.082; 95% CI, 1.313–5.980; P = 0.008) and advanced stage (III, IV) (OR, 1.977; 95% CI, 1.095–3.568; P = 0.024) were independently significant risk factors for postoperative major bleeding (Table 5).
Go to :
DISCUSSION
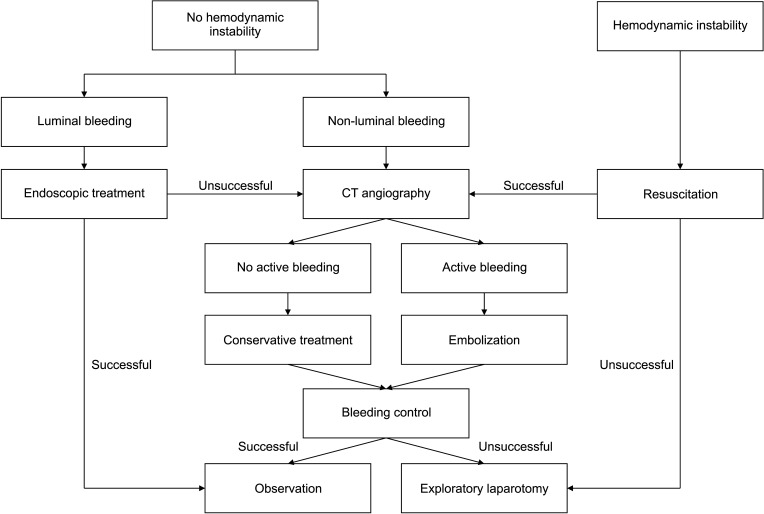
Overall, postoperative major bleeding rate was 1.1% in 3,663 patients who received laparoscopic gastric cancer surgery between January 2012 and December 2017. The causes of major bleeding were rupture from direct arterial or venous trauma, delayed rupture from a previously existing pseudoaneurysm, and anastomosis site bleeding. According to protocols of our institution, if the patients are hemodynamically stable with intraluminal bleeding, we evaluate the anastomosis site with endoscopy. In nonluminal bleeding, the patients receive CT angiography first. If active bleeding is confirmed on CT, we consider angiography following embolization or exploratory laparotomy. If patients are in hemodynamic instability, CT angiography is completed with resuscitation. However, in cases of uncontrollable hemorrhagic shock status, exploratory laparotomy is performed immediately (Fig. 3).
Our study showed that postoperative major bleeding, intraoperative and postoperative transfusions were not significantly higher in the antiplatelets/anticoagulants group. Intraoperative hemorrhage is most commonly caused by structural defects, anticoagulant excess, hyperfibrinolysis, or a generalized and severe disorder of hemostasis, such as disseminated intravascular coagulation. Early postoperative hemorrhage (within 2 days of surgery) suggests a defect in primary hemostasis, such as significant thrombocytopenia (platelet count less than 50 × 109/L) or platelet dysfunction, each of which may be inherited or acquired [13]. However, there are some studies that showed that intraoperative and early postoperative bleeding resulted from a technical defect in 75% to 90% of cases. Surgical bleeding can be distinguished by 2 different causes. A hemostatic defect is the most likely cause when bleeding occurs at multiple sites simultaneously, such as the surgical site in addition to vascular access sites and mucous membranes, skin, or nonoperative hematuria. A structural defect requiring surgical intervention is more likely to be the cause of bleeding that occurs from a single site, is of sudden onset, and/or represents a massive hemorrhage or pulsatile bleeding where a source is evident [1415]. In the present study, postoperative major bleeding occurred most often in surgical sites or particular vessels. Therefore, postoperative bleeding can be associated with surgical technique as well as medical patient considerations such as the administration of medications, which affect coagulation cascade and platelet aggregation. Our results suggest that even if patients have bleeding tendencies including persistent ooze in the operation field, bleeding can be controlled by meticulous surgical techniques by experienced surgeons with new surgical instruments.
Multivariable analysis revealed that male sex and advanced stage (III, IV) were risk factors of postoperative major bleeding risk. One study indicated that bleeding events were more frequent in males with AF during warfarin therapy [16]. As our result, Park et al. [17] analyzed male was an independent risk factor of postoperative hemorrhage following gastrectomy. In transoral surgery of the oropharynx, males were more likely than females to have a bleeding episode requiring operative intervention. The authors raised the possibility that this may not have been related to anatomy or pathologic findings but may be the result of increased postoperative exertion or activity [18]. Some literature reported that bleeding events were increased in advanced stages of gastric cancer [61920]. To achieve a curative resection, metastatic lymph nodes and other organs that tumor cells invaded should be removed. During lymph node dissections, the high temperature of the ultrasonic knife may injure blood vessel walls and adjacent tissue, facilitating vascular damage and aneurysm formation. This can result in postoperative bleeding [20]. Although D2 lymphadenectomy and resection of other organs were not revealed to be risk factors in our multivariable analysis, patients with advanced-stage cancers were usually in the high-risk group for postoperative major bleeding. Comparing major bleeding risk with antiplatelets and/or anticoagulants use in the advanced stage (III, IV) group, postoperative major bleeding risk was not significantly increased in the antiplatelets/anticoagulants group. This result strongly supports that antiplatelets and/or anticoagulants use does not increase postoperative major bleeding risk.
In our study, early complications with surgery included: atelectasis, pleural effusion, ileus, delayed gastric emptying, wound infection, pneumonia, complicated fluid collections, anastomosis leakages, anastomosis stenosis, and surgical site bleeding. One case of thromboembolism occurred in an 82-year-old male with hypertension, diabetes mellitus, and AF (CHADS2 score, 5) who was on warfarin before surgery. Preoperative bridging with low molecular weight heparin (LMWH) was initiated 10 days before laparoscopic distal gastrectomy with Billroth I. LMWH was interrupted for 3 days due to bleeding risk. On postoperative day 3, the patient showed seizure-like movements and mental status change. An ischemic stroke was detected on brain MRI. LMWH was resumed and overlapped with warfarin. Owing to early detection and treatment, the patient was discharged without sequelae. The overall incidence of clinically evident stroke after noncardiac, non-neurologic surgery is reported to be between 0.1% and 0.8% in registry and database studies [212223]. Comorbidities, hypotension, and type of surgery are the main causes of perioperative stroke [21]. Patients who are on oral anticoagulant therapy pose a common and challenging perioperative problem. Therefore, there is a need to balance the risk of thromboembolic events during the interruption of oral anticoagulant therapy against the risk of bleeding [24].
According to a literature, open surgery as compared to laparoscopic procedure leads to activation of the clotting system of a higher degree [25]. Yasui et al. [26] stated that patients treated with laparoscopic surgery tended to experience thromboprophylaxis-related bleeding more often than those treated with open surgery. To investigate the association of antithrombotic agent-related intraoperative bleeding with laparoscopic surgery, we performed subgroup analysis. We selected patients using antiplatelets and/or anticoagulants and divided them further into laparoscopic and open surgery groups. Contrary to the previous study, there was no significant difference in intraoperative transfusion rate between open and laparoscopic surgery (14.3% vs. 8.9%, P = 0.483). In addition, postoperative major bleeding risk was not significantly higher in the laparoscopy group than in the open group (0% vs. 1.9%, P > 0.999). These results suggested that laparoscopic gastrectomy can be safely completed in patients using antithrombotic agents while considering the risk of bleeding.
Patients receiving antiplatelets and/or anticoagulants undergoing gastrectomy should be urged to consult their cardiologists for management of discontinuing antiplatelet agents. Decisions about cessation and resumption of antiplatelet agents are based on the risk stratification for thrombosis and bleeding. According to the risk assessment, gastric cancer surgery has an intermediate risk. Those patients at high risk of thrombosis continue antiplatelets and/or anticoagulant medications in the perioperative periods. However, if the patients are in the intermediate- or low-risk category of perioperative thrombosis, physicians are recommended to stop these medications 5–7 days before surgery [27]. According to the INR, warfarin should be stopped 1–8 days before surgery. Furthermore, bridging heparin should be administered during the time that oral anticoagulation has been discontinued. For patients on DOACs, stopping DOACs is based on creatinine clearance. Given the short half-life of DOACs, bridging heparin is not necessary for these patients. Antiplatelets and anticoagulants may be resumed within 1–2 days without bleeding risk [28].
To our best knowledge, the present study is the first to analyze antithrombotics-related postoperative bleedings only for laparoscopic gastrectomy. Although small cases, this is the first study including patients who took DOACs in the antiplatelets and/or anticoagulants group. Of note, there was no difference in postoperative major bleedings, transfusions, and complications between antiplatelets and/or anticoagulants group and control group.
There are some limitations in this study. First, based on the retrospective design, the duration of discontinuation was not controlled exactly by the protocol of our institution. For investigating accurate correlations between antiplatelets and/or anticoagulants with postoperative major bleeding, this variable should be controlled. Second, only 11 patients (2.1%) who used DOACs during the perioperative periods were included. The use of these agents is increasing, and further studies are needed to address the association between DOACs and postoperative major bleeding.
In conclusion, preoperative antiplatelets and/or anticoagulants administration did not significantly increase the risk of postoperative major bleeding after laparoscopic gastric cancer surgery. Male sex and advanced stage (III, IV) were independent risk factors for postoperative major bleeding risk regardless of antiplatelets and/or anticoagulants.
Go to :
 XML Download
XML Download