

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer is treated with adjuvant chemotherapy to eliminate micrometastases even after curative surgery. The decision to provide adjuvant chemotherapy is based on the likelihood of disease recurrence. Although it has been proved that chemotherapy lowers recurrence and increases survival in patients with stage III colorectal cancer [12], there are controversial evidences that chemotherapy has favorable effects on patients with stage II colorectal cancer [3456]. It has been demonstrated that the pT4 has a poor prognosis in patients with node-negative disease; hence, the administration of adjuvant chemotherapy was strongly advocated [78]. Adjuvant chemotherapy is administered to patients with pT3N0 colorectal cancer based on high-risk clinicopathologic features (HRF) for prognosis, which include preoperative bowel obstruction, localized perforation, perineural invasion (PNI), lymphovascular invasion (LVI), <12 lymph nodes (LNs) retrieved, poorly differentiated/undifferentiated (PD/UD) tumors, and resection margin involvement. In T3N0 colorectal cancer with HRF, however, there is a lack of strong evidence addressing the effectiveness of adjuvant chemotherapy [91011].
The prognostic importance of individual HRF showed heterogeneous results. In addition, several HRFs, such as LVI and PNI, exhibited interobserver variability, and diagnoses were frequently modified based on the use of staining techniques or rigorous pathological evaluation. Some studies reported that patients with multiple HRF showed significantly poorer oncological outcomes than those with single HRF. However, adjuvant chemotherapy has been advised for patients with the above-mentioned risk factors, regardless of the number and kind of risk factors [1213].
The oncological importance of HRF according to type, as well as the oncological benefits of adjuvant treatment in patients with T3N0 colorectal cancer and HRF, has not been adequately examined. The effect of adjuvant chemotherapy according to the number of HRFs must also be investigated, as it would serve as a basis for the optimal and individualized administration of adjuvant chemotherapy in pT3N0 colon cancer. Therefore, we examined the effect of adjuvant treatment on oncological outcomes according to the kind and number of clinicopathologic HRF in pT3N0 colorectal cancer.
Go to : 
METHODS
Patients population
This study included 1,205 patients with pathologically proven pT3N0 colon cancer from January 2012 to December 2016 who underwent curative surgical resection. Among 8,786 patients who received elective surgical resection for primary colorectal cancer during the study period, patients with synchronous distant metastasis (n = 1,479), other concurrent malignancies (n = 208), synchronous or metachronous colorectal cancer (n = 169), patients treated with neoadjuvant treatment (n = 996), stage other than pT3N0 (n = 3,897), without standard radical resection (n = 349), patients with inaccurate staging (n = 18), rectal cancer (n = 424), and lack of record of adjuvant chemotherapy treatment status (n = 5) were excluded (Fig. 1). The study protocol was approved by the Institutional Review Board of Asan Medical Center (No. 2170-0955), and the requirement for informed consent was waived. The study has been reported according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.

Adjuvant treatment and surveillance
Adjuvant chemotherapy was recommended for patients who had more than one of the following HRF: bowel obstruction, localized perforation, <12 LNs examined, LVI, PNI, PD/UD, and resection margin involvement. The administration of adjuvant chemotherapy was finally decided after an interview between each patient and a medical oncologist to consider the risks and benefits.
The adjuvant chemotherapy regimen included fluorouracil (5-FU)/leucovorin (425 mg/m2 and 20 mg/m2 per dose, respectively, for 5 days), FOLFOX (5-FU/leucovorin/oxaliplatin; 2,800 mg/m2, 400 mg/m2, and 85 mg/m2 per dose, respectively), oral capecitabine (1,250 mg/m2 twice a day for a maximum of 14 days), and XELOX (capecitabine/oxaliplatin; 1,000 mg/m2 twice a day for a maximum of 14 days and 130 mg/m2 on day 1, respectively). When the early period of study, some patients received uracil and tegafur (UFT) plus leucovorin regimen consisting of five 28-day cycles of oral UFT 300 mg/m2/d and oral leucovorin 90 mg/day in 3 divided doses.
Postoperative surveillance consisted of physical examination, serum CEA, laboratory test, and/or chest radiographs (every 3–6 months), abdominopelvic CT (every 6 months), and chest CT (every 6–12 months). Colonoscopy was done every 2 to 3 years after surgery. In cases with preoperative bowel obstruction, colonoscopy was performed 3 to 6 months after surgery. PET and MRI were considered for patients with suspected abnormal findings in scheduled postoperative surveillance with abdominopelvic/chest CT.
Statistical analysis
The primary endpoint was overall survival (OS) and recurrence-free survival (RFS). RFS was the interval between the operation date and the diagnosis date of relapse. OS, the interval between the surgery and the date of any cause of death, was also evaluated according to adjuvant chemotherapy receipt. Descriptive statistics of clinicopathological variables were presented as mean ± standard deviation (SD) or with range. Patients were categorized into 2 groups; the adjuvant chemotherapy and the no adjuvant chemotherapy groups, according to whether adjuvant chemotherapy was applied. Continuous variables were compared using the Student t-test. Categorical variables were examined with the chi-square test, Fisher exact test, or the Mann-Whitney test. According to the number of HRFs, patients were also compared in terms of OS and RFS among groups with no HRF, one HRF, or more than 2 HRF.
The Kaplan-Meier method was used for OS and RFS analysis, and data were compared using the log-rank test between the adjuvant and no adjuvant groups, as well as according to the existence of HRF. Cox regression analysis was performed to assess the prognostic impact of the risk factors on RFS and OS. The results were considered statistically significant if the P-value was less than 0.05. Data analysis was done with IBM SPSS Statistics ver. 27.0 (IBM Corp.).
Go to :
RESULTS
Clinicopathologic characteristics and treatment of patients
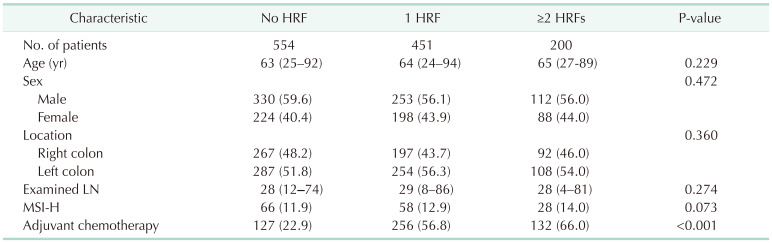
A total of 1,205 patients were included. The mean age with SD was 63 ± 12 years (24–94 years); 699 patients (58.0%) were males. The mean number of harvested LNs was 28 (4–86). In 13 cases (1.1%), <12 LNs were harvested. LVI and PNI were observed in 286 (23.7%) and 191 patients (15.9%), respectively. For tumor differentiation, poorly differentiated tumors were found in 43 cases. Among the 366 patients (30.4%) with preoperative obstruction, 292 (79.8%) had an endoscopy, and 74 (20.2%) presented complete symptomatic obstruction. A total of 11 patients (0.9%) had resection margin involvement.
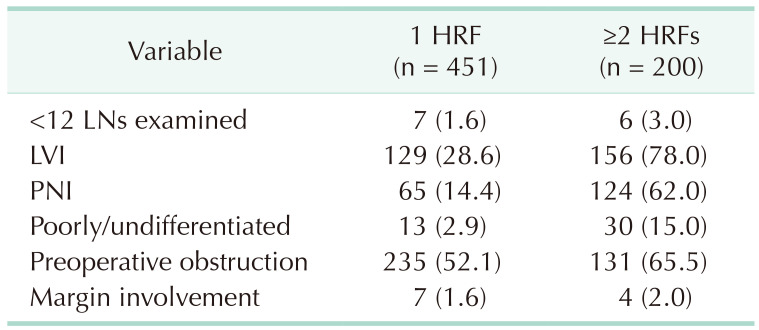
Among the patients, 751 (62.3%) had at least 1 risk factor, and 515 (42.7%) received adjuvant chemotherapy (Table 1). HRFs were significantly more common in the adjuvant chemotherapy group. Adjuvant chemotherapy was given in 66% of patients with more than 2 HRFs and 56.7% of those with one HRF, while 40.3% of patients with HRF did not receive adjuvant chemotherapy. Adjuvant chemotherapy was administered in 22.9% of patients without HRF. The chemotherapy regimens varied; 145 patients received 5-FU/leucovorin, 169 received FOLFOX, 128 received capecitabine, 42 received UFT-E/leucovorin, and type of regimens was not known in 31 patients. In the chemotherapy group, 256 patients had a single risk factor. Bowel obstruction is the most common single HRF (113, 44.1%) in patients treated with adjuvant chemotherapy, followed by LVI (98, 38.3%) and PNI (35, 13.7%). LVI was the most common HRF type in patients with multiple risk factors followed by clinical obstruction, and PNI (Table 2). The mean follow-up duration of the cohort was 49 ± 22 months.
The 5-year recurrence-free survival and overall survival according to individual high-risk feature
The 5-year RFS and the OS rates in the cohort were 92% and 91.4%, respectively. Patients who received adjuvant chemotherapy showed similar RFS to those who did not receive adjuvant chemotherapy. Patients treated with adjuvant chemotherapy, however, had higher OS rate in survival analysis than those without adjuvant chemotherapy (Fig. 2). The 5-year RFS and OS were compared according to the existence of individual HRF (Fig. 3). PNI and bowel obstruction were significantly associated with RFS and OS. Margin involvement of tumor and LVI reduced RFS, but neither was associated with OS. Less than 12 LNs examined, and poorly/undifferentiated tumors were not associated with either RFS or OS. In the cases with LVI, PNI, or bowel obstruction, the adjuvant chemotherapy group had improved OS. However, RFS was not increased with adjuvant chemotherapy in patients with any kind of HRF.
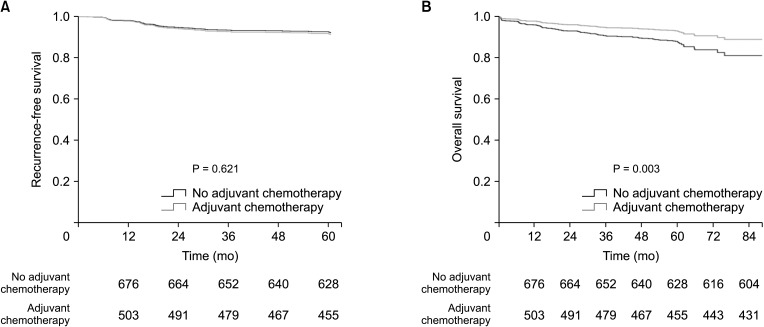 | Fig. 2Recurrence-free survival (A) and overall survival (B) according to adjuvant chemotherapy in T3N0 colon cancer.
|
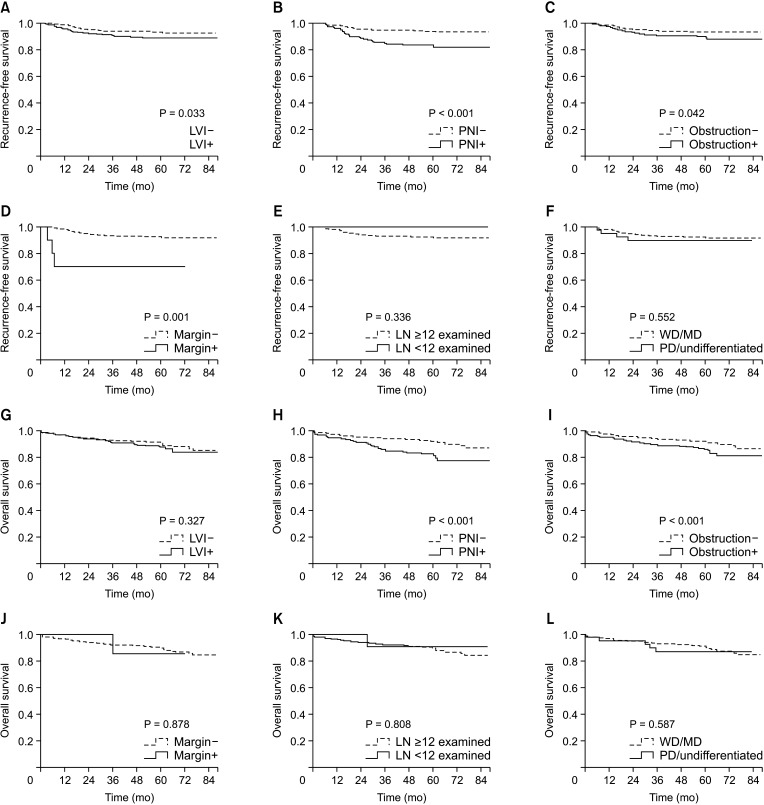 | Fig. 3Recurrence-free survival (A–F) and overall survival (G–L) according to each type of high-risk features. PNI and obstruction showed significant association with recurrence-free survival and overall survival. LVI, lymphovascular invasion; PNI, perineural invasion; Margin, margin involvement by tumor; LN, lymph node; WD, well differentiated; MD, moderately differentiated; PD, poorly differentiated.
|
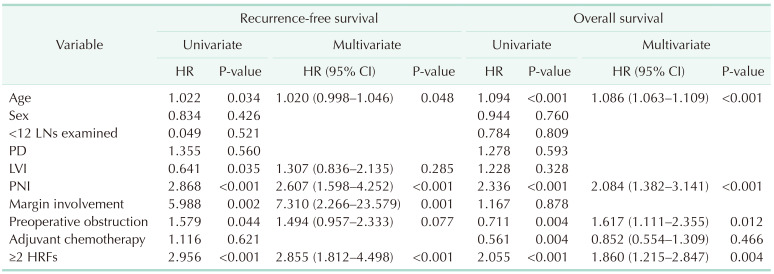
Considering individual type of HRF, PNI, margin involvement of tumor, and age were confirmed as independent risk factors of reduced RFS in multivariate analysis. Age, PNI, and obstruction were risk factors for reduced OS (Table 3). Considering the number of HRFs, multiple HRFs was confirmed as a significant factor for both RFS and OS. Adjuvant chemotherapy was not associated with both RFS and OS when type and number of HRFs were considered as covariates (Table 3).
Oncologic outcomes and impact of the number of high-risk features according to adjuvant chemotherapy treatment
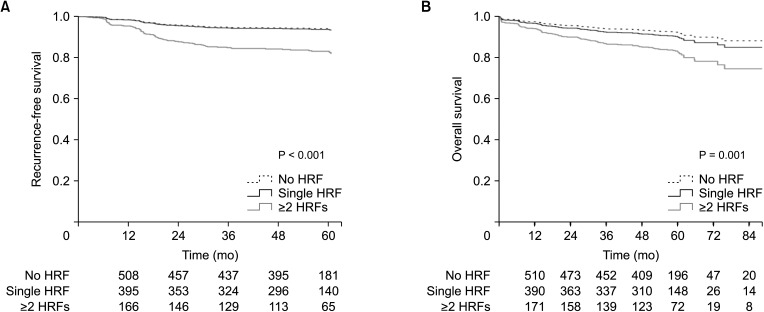
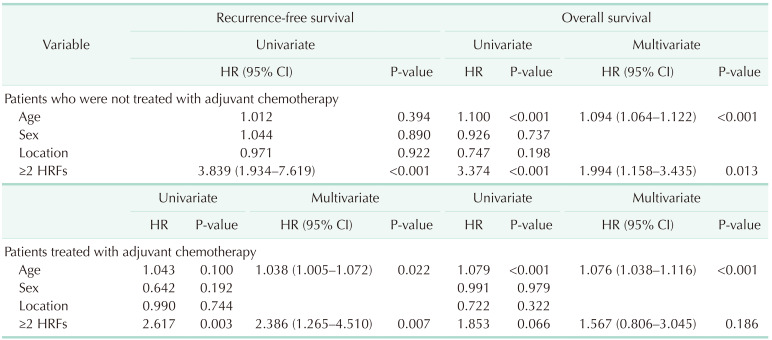
The 5-year RFS and OS were significantly different according to the number of HRFs. The 5-year RFS was 93.9% in patients with 0–1 HRF and 83.4% in those with ≥2 HRFs. The 5-year OS rates were 91.8% and 81.7% for patients with 0–1 HRF and ≥2 HRFs, respectively. The patients with 0 or 1 HRF showed similar results, but patients with ≥2 HRFs showed significantly lower 5-year RFS and OS (Fig. 4) in overall cohort. The impact of the number of HRFs on RFS and OS according to adjuvant chemotherapy receipt was evaluated. Multiple HRF was confirmed as an associated factor with both RFS and OS in patients who did not receive adjuvant chemotherapy (Table 4) and it was the single associated factor with RFS. In patient treated with adjuvant chemotherapy, multiple HRFs was associated with RFS, but it was not associated with OS in multivariate analysis (Table 4).
Go to :
DISCUSSION
Adjuvant chemotherapy improved the OS rate but was not related to better RFS in the patients with T3N0 colon cancer included in this study. More than 2 HRFs, which is a criterion that guides the decision of adjuvant chemotherapy, was a significant risk factor for worse RFS and OS. The impact of adjuvant chemotherapy on OS was sustained regardless of the number of HRFs, based on the results of the present study.
We only included patients with T3N0 colon cancer because the prognostic impact of T4 disease in patients without LN metastasis has been well demonstrated, and the benefit of adjuvant chemotherapy for these patients has been defined. Our focus was to determine adequate guidance for adjuvant chemotherapy in T3N0 colon cancer patients with relatively favorable prognoses.
The prognostic benefit of adjuvant chemotherapy in stage II cancer has been controversial in many previous reports. Some reported that a clear OS benefit of adjuvant chemotherapy had not been shown for stage II colon cancer [114151617], and some studies reported higher survival outcomes of stage II colorectal cancer with adjuvant chemotherapy in subgroups of patients [171819]. Studies reporting prognostic improvement with adjuvant chemotherapy indicate that this benefit was mainly seen in the subgroup of patients with T4 disease [42021]. However, it is difficult to evaluate the role of adjuvant chemotherapy in T3N0 colon cancer. Recently, a study including only stage IIA colon cancer from 2010 to 2015 from the national cancer database reported an estimated 5-year OS benefit of 11.3% with adjuvant chemotherapy in patients with high-risk pathological features. However, the influence on recurrence-related outcomes was not evaluated. The 5-year disease-free survival was reported as about 68% to 83% in stage II disease after surgical resection alone [22], and these favorable oncological outcomes have restricted the opportunity for adjuvant chemotherapy to play a role. The OS has been reported to be higher than 70% in recent studies [172324]. In the present study, the 5-year RFS and OS, which are higher than 90%, are even better. However, oncologic outcomes showed difference according to the number of HRFs although overall oncologic outcomes in stage II is quite favorable. We showed that 5-year RFS and OS are significantly lower in patients with more than 2 HRFs. Therefore, we can assume that decision-making regarding adjuvant chemotherapy for stage IIA colon cancer needs to consider the number of HRFs. A study with the SEER (Surveillance, Epidemiology, and End Results) database showed that OS decreased according to the number of HRFs; 78.4% for patients with no HRF, 71.99% for those with one HRF, and 59.24% for those with more than 2 HRFs, which is worse than the OS of stage III disease, which is reported to be 64.68% [23]. The detrimental effect of multiple HRFs on OS was also demonstrated in another study using data from the SEER database from a different period [14]. The International Duration Evaluation of Adjuvant Chemotherapy Collaboration data also reported that the 5-year disease-free survival was 74.8% for stage II patients with 2 or more HRFs, compared with 87.3% for patients with one HRF [25]. However, adjuvant chemotherapy improved OS and did not improve RFS regardless of the number of HRFs in the present study.
This confusing result may be caused by a combination of various factors. Low compliance with the adjuvant chemotherapy administration guidelines in stage II disease may be a contributing factor. In many reports, adjuvant chemotherapy was given to less than 40% of patients with stage II disease, and even patients without HRF received adjuvant chemotherapy in around 10% of cases [1417232627]. In the current study, adjuvant chemotherapy was given at a greater proportion than in previous reports. Even so, 40.3% of patients with HRF did not receive adjuvant chemotherapy, and 22.9% of those without HRF received adjuvant chemotherapy. Therefore, the effect of adjuvant chemotherapy based on prognostic risk features would not be clearly presented. This overall low obedience to the guidelines may be caused by the uncertainty of the benefits of adjuvant chemotherapy. The decision to give chemotherapy depends on risk-to-benefit consideration, and a lack of evidence revealing the benefit of adjuvant chemotherapy makes physicians and patients reluctant to proceed with adjuvant chemotherapy, with the toxicity of the adjuvant chemotherapy and age being the commonly considered criteria [28].
Another factor is that HRF included in various studies differed. Some studies did not include the recommended HRF [1423], while some included other clinicopathologic features such as location, age, microsatellite instability status, and tumor deposit [1729].
The weight of the prognostic importance of individual HRF is also often considered the same, although evidence suggests that the influence of each HRF as a prognostic factor varies. Studies regarding the prognostic importance of HRF in cases other than with T4 disease showed high heterogeneity and low levels of evidence [430]. Histological differentiation, inadequate LN evaluation, and margin involvement were not sufficiently studied, or the results were contradictory. The small proportion of patients with these HRFs may contribute toward inconsistent reporting. The proportion of patients with <12 LNs was reported to be approximately 10% [1417]. The proportion with margin involvement and poor differentiation was also very low [141723]. A study assessing the survival benefit of adjuvant chemotherapy in patients with colon cancer with <12 LNs harvested reported that 23.3% of patients had inadequate LNs harvest [16]. The small number of events limited the usefulness of <12 LNs harvested as an HRF. In the present study, the proportions of <12 LNs harvested, poor differentiation, and margin involvement were reported as 1.1%, 3.5%, and 0.9%, respectively.
Although LVI and PNI are generally accepted pathologic HRFs [2627], there have also been controversial data regarding the benefit of adjuvant chemotherapy for patients with LVI or PNI. The variability of diagnostic accuracy caused interobserver variance. Different diagnostic methods for LVI and PNI may also result in prognostic inconsistency. In this study, PNI was the strongest prognostic HRF for both OS and RFS. It has been widely reported that the presence of PNI would indicate more aggressive clinicopathologic features, resulting in poor prognosis in colorectal cancer, and some previous studies found that PNI could be an indicator recommending chemotherapy in colon cancer [2627]. In the present study, patients with LVI or PNI showed improved OS with the addition of adjuvant chemotherapy. This suggests that LVI and PNI can be potential predictors of adjuvant chemotherapy outcomes in T3N0 colon cancer.
Although HRF showed mixed results in terms of adjuvant chemotherapy benefits, a consistent positive effect of adjuvant chemotherapy was found for RFS and OS for bowel obstruction [429]. In this study, bowel obstruction was a significant negative risk factor for OS, and adjuvant chemotherapy benefited OS in these patients (97.5% vs. 73.9%, P = 0.002). Although not statistically significant, bowel obstruction was associated with decreased RFS. The oncological benefit of adjuvant chemotherapy was confined to improvement of the OS and did not appear to impact RFS. As mentioned above, we must consider the general performance status to determine adjuvant chemotherapy. Patients treated given adjuvant chemotherapy may have had better general conditions, which could be associated with better OS. Therefore, we have adapted the results of previous studies carefully because improvement in OS may not be entirely due to adjuvant chemotherapy.
This study has some limitations. Because it is a retrospective study, it may include selection bias. We cannot ascertain exactly why patients who had HRF did not receive adjuvant chemotherapy. In addition, completion of chemotherapy and adjuvant chemotherapeutic regimen was not included in the analysis because of missing data. We did not conduct a central review of pathological HRF in which interobserver variation was involved in the diagnosis. However, this study included a relatively large real-world cohort with long-term follow-up and access to HRF with institutional standards. The study results should be helpful for practitioners to understand the current status and benefit of adjuvant chemotherapy for T3N0 colorectal cancer. In conclusion, considering the results, we can identify that individual HRF possess different prognostic importance, and current guidelines, where all HRFs are treated as having the same level of importance, need to be reevaluated. We have to stratify each risk factor in terms of the prognostic impact and stratify patients with T3N0 according to the risk of poor oncological outcomes. This tailored stratification would result in the effective use of adjuvant chemotherapy, which can induce oncological improvement. It will also be helpful to optimize and differentiate chemotherapeutic regimens according to the prognosis.
Go to :
 XML Download
XML Download