

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Calcific coronary artery disease is an increasingly prevalent entity in the catheterization laboratory which has implications for stenting and expected outcomes. With new interventional techniques and equipment, strategies to favorably modify coronary calcium prior to stenting continue to evolve. This paper sought to review the latest advances in the management of severe coronary artery calcification in the catheterization laboratory and discuss contemporary percutaneous interventional approaches.
EPIDEMIOLOGY AND OUTCOMES
Calcific coronary lesion is an increasingly common finding in the catheterization laboratory. In angiographic studies, significant coronary calcification was detected in approximately 20–30% of patients undergoing percutaneous coronary intervention (PCI) but this is likely to be an under-estimate as fluoroscopy is poorly sensitive for its detection.1)2) In a single center retrospective intracoronary imaging study, among 889 patients with de novo culprit lesions that underwent pre-PCI optical coherence tomography (OCT) imaging, 317 (35.7%) of lesions had moderate to severe calcification with a mean calcium arc of 51°.3) Male gender, white race, metabolic syndrome, uremia and diabetes mellitus all increase risk of coronary calcification.4)5)6)7)
Presence of significant coronary calcification is a well-established predictor of future cardiovascular events.8)9) The amount of coronary calcification reflects plaque burden and has been incorporated into prediction models to assess patients’ future cardiovascular risk.10) Patients with higher coronary calcium score on computed tomography are at significantly higher risk for cardiac events as well as progression.11)12)
Coronary calcification has been associated with poor outcomes post-intervention and is likely to relate to suboptimal stent-expansion. In an analysis which included data from 6,855 patients from 2 large-scale randomized controlled trials (RCTs), ACUITY and HORIZONS-AMI, moderate-to-severe coronary calcification was strongly associated with stent thrombosis and ischemic target lesion revascularization at 1 year.1) In another pooled analysis of 7 drug-eluting stents clinical trials which included a total of 6,296 patients, severe coronary calcification was an independent predictor of poor clinical outcomes after PCI, including all-cause mortality.2) The more recent MACE-trial was a prospective, multicenter, observational study that enrolled 350 patients across 33 sites from 2013 to 2015 and showed that severe coronary calcification was associated with lower lesion and procedural success rates and higher overall adverse events at 1 year.13)
According to a National Cardiovascular Data Registry CathPCI Registry analysis, the use of coronary atherectomy for treatment of calcification has increased from 1.1% in 2009 to 3.0% in 2016.14) This temporal increase in work volumes was associated with a lower rate of mortality and PCI failure but interestingly associated with a small increase in coronary perforation risk.
EVALUATION OF CORONARY CALCIUM
An accurate and comprehensive assessment of the location and severity of calcification is crucial to the optimal management of calcified coronary lesions. In the catheterization laboratory, coronary calcification is evaluated with the use of either angiography and intra-coronary imaging such as intravascular ultrasound (IVUS) or OCT. Comparison of different imaging modalities for coronary calcium in the catheterization laboratory is illustrated in Table 1.
Table 1
Comparison of imaging techniques for coronary calcification in the Catheterization laboratory
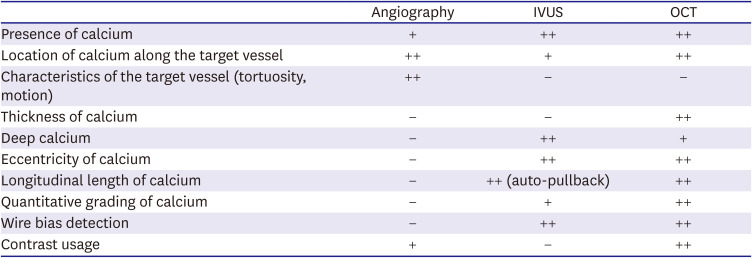
Coronary angiography is routinely performed before any intervention. Prior to contrast injection, calcification may be visualized along the silhouette of a coronary artery as radio-opaque shadows synchronous with cardiac motion. Core lab defined none/mild, moderate (only during the cardiac cycle before contrast), and severe (radiopacities without cardiac motion before contrast affecting both arterial walls).15) Thus, angiography has limited sensitivity in the detection of mild to moderate coronary calcification particularly 1–2 quadrants and short segments.16) It is also unable to provide information regarding the distribution, eccentricity and depth of calcium within the vessel wall. Use of summation angiography (such as StentBoost or ClearStent) can allow an estimation of calcium distribution but is proprietary and vendor dependent, and not quantitative.
Despite its limitation, preliminary assessment with angiography is important in the management of coronary calcium such as locating calcium within the coronary system and evaluating characteristics of the target vessel. For aorto-ostial lesions, some operators prefer orbital atherectomy with the benefit of ablating calcium during backward motion and risk of wire fracture using rotational atherectomy. If the target vessel shows significant tortuosity and high mobility during cardiac contraction, atherectomy might be associated with significant perforation risk and rotational atherectomy with a smaller burr size would be preferred over a larger one. It is also not uncommon to encounter myocardial bridging distal to a calcific lesion in the left anterior descending (LAD) and, and calcium modification with atherectomy or lithoplasty should be avoided in this setting.
Intracoronary imaging is much more sensitive in the evaluation of coronary calcification. On IVUS, coronary calcification appears as hyper-echogenic arc. Pathological and clinical data have confirmed the superiority of IVUS over angiography in the detection of this calcification.17)18) IVUS gives an accurate assessment on the calcific arc circumference inside the coronary artery, which can predict the efficiency of stent expansion.19) The introduction of auto-pullback allows the measurement of longitudinal calcium length. Near complete reflection of ultrasound by calcium with resultant acoustic shadowing severely limits IVUS ability to measure thickness. On OCT, these plaques appear as well-delineated areas of specific signal attenuation with a “hard edge.”20) Utilizing transmissible light waves, OCT can distinguish calcific thickness as well as length and allows for a more accurate reflection of volume (calcium volume index) which can adversely affect stent expansion.21)22)
Intravascular imaging can also provide important information to predict outcome following calcium modification, such as eccentricity of calcium and location of wire bias. Such information is not available with angiography alone. With highly eccentric or even nodular calcific lesions, currently available calcium modification techniques are often unable to provide satisfactory expansion and rotational atherectomy with larger burr might be the only effective option with risk of perforation. Wire bias across the lesion on intravascular imaging may assist in predicting the atherectomy result but accuracy and consistency are limited.
An OCT-based scoring system has been adopted into clinical practice which allows for a simple evaluation of calcific plaque volume and possible risk of stent under-expansion and negative outcomes.23) Maximum calcium arc angle >180° (scores 2), maximum calcium thickness >0.5 mm (scores 1) and calcium length >5 mm (scores 1) and calcium modification recommended prior to stenting if score >2/4 (since all have been shown to independently predict stent under-expansion). More recently an IVUS-based scoring system has been introduced.24) Morphological characteristics associated with stent under-expansion from a retrospective cohort include superficial calcium angle >270° longer than 5 mm, 360° arc superficial calcium, calcific nodule and vessel diameter <3.5 mm adjacent to calcium. The presence of any one of these characteristics should prompt the operator to consider modification (e.g., atherectomy).
OPTIONS OF CALCIUM MODIFICATION
Rotational atherectomy
Rotational atherectomy, introduced by David Auth in 1981 and first performed in human coronary arteries by Fourrier et al.25) in 1988, currently remains the most commonly used atherectomy device for calcified lesions worldwide. The device has a microscopic diamond-coated burr (front half only) which can rotate at high speed (140,000–200,000 rpm). The burr is advanced over a dedicated guidewire (0.009”×325 cm) and connected to the console in which a motor converts compressed gas to rotational energy. Continuous intracoronary infusion of a lubricant solution (usually heparinized saline ± vasodilators) is required throughout the procedure. On forward advancement, the burr preferentially ablates fibrocalcific plaque and pulverizes tissue into 5–10 μm debris. The device doesn’t ablate when burr is being retracted. Potential serious complications include burr entrapment/separation, coronary dissection or perforation, and slow or no flow phenomenon. The risk of such complications could be minimized by meticulous technique and avoiding extremely angulated or tortuous vessels, allowing adequate time intervals between runs, and avoiding burr deceleration of >5,000 rpm.
The ROTAXUS trial is the first RCT to evaluate routine rotational atherectomy before paclitaxel-eluting stent implantation in calcified coronary artery disease. The study randomly assigned 240 patients with complex calcified coronary lesions to stenting either with or without prior rotational atherectomy. At 9 months, the study failed to show any significant superiority of rotational atherectomy over no atherectomy in terms of in-stent restenosis, target lesion revascularization, stent thrombosis and major adverse cardiac events.26) At an extended follow-up of 2 years, there were no differences in mortality, myocardial infarction and target lesion revascularization between patients treated with or without rotational atherectomy.27) It should be noted that 12.5% crossed over from balloon strategy to rotational atherectomy (RA) indicating rate of absolute need in a case (such as undilatable or uncrossable lesions). Recent advances in equipment in RotaPro™ system means the advancer encompassing all controls and a new digital speedometer removing the need for foot pedals. Importantly, a more maneuverable RotaWire Drive™ allows for the ability to primary wire lesions and obtain enough purchase to perform RA without struggling to pass microcatheters to exchange.
The PREPARE-CALC trial is a more recent RCT comparing rotational atherectomy with modified balloons in lesion preparation before implantation of third generation sirolimus-eluting stent.28) The study randomized assigned 200 patients with severely calcified native coronary artery disease from 2 centers in Germany to either modified balloons or rotational atherectomy followed by stenting. Strategy success was significantly more common in the group treated with rotational atherectomy, primarily driven by higher success rate in non-LAD disease and more complex lesions.29) At 9 months, there was no significant difference between the 2 groups in terms of in-stent late lumen loss, target lesion revascularization, stent thrombosis or target vessel failure. Subgroup analysis demonstrated higher side branch patency rate in patients treated with rotational atherectomy, as compared with modified balloons.30)
Burr entrapment and coronary perforation are serious complications following rotational atherectomy, especially in long and angulated calcified lesions. Halfway rotational atherectomy is a novel technique in which the operator does not advance the burr all the way to the end of a long angulated calcified lesion in the coronary artery.31) In practice, this may be where there is burr has advanced but unable to fully lesion-cross or repeated runs still see the burr “maximally advanced.” The burr is retrieved once it reaches this point or where an unfavorable lesion angle is, conventional balloon angioplasty is then performed in the remaining segment of the lesion and if successful then stenting is done. This technique was compared with conventional rotational atherectomy in a retrospective single-center study which included 307 consecutive calcified lesions treated with rotational atherectomy.32) Although no burr entrapment or coronary perforation was reported in the halfway rotational atherectomy group, there was no statistically significant difference demonstrated between the 2 groups in the incidence of various complications.
Orbital atherectomy
Orbital atherectomy, first introduced in 2007 for peripheral intervention, gained Food and Drug Administration approval for coronary intervention in 2013. The 1.25 mm crown of the device is eccentrically mounted with diamond coated on both front and back. The crown is attached to a controller, itself connected to a pneumatic console which powers the entire system. The crown is advanced through a specialized 0.014” guidewire with continuous intracoronary infusion of lubricant solution during the procedure. Orbital atherectomy works through rapid continual elliptical rotation of the crown with increase in orbital diameter. The resultant centrifugal force pushes and compresses crown against calcific plaque with a differential sanding action, creating debris of 2–4 μm in size during the process. The device allows the operator to use different rotational speeds (low speed: 80,000 rpm, high speed: 120,000 rpm) to increase orbital diameter for larger vessels. Bi-directional removal of calcium was possible during pull and push. During pulling back, the crown might be able to remove more calcium on inner curve in curved lesion. Compared with RA, orbital atherectomy is a more “side cutting” than “front cutting” and maintains flow throughout runs. It could debulk significantly with a 6F system and can be used for multiple lesions in a case. Potential complications include coronary dissection, perforation, slow or no flow phenomenon. Orbital atherectomy is not recommended for in-stent restenosis but this is being studied and vessels with gross dissection may be a contraindication due to stalled crown risk.
The ORBIT I trial was a prospective non-randomized study evaluating the safety and feasibility of orbital atherectomy in 50 patients at 2 Indian sites with calcified native coronary artery disease.33) Procedural success rate was 94%, while major adverse cardiac event rate was 12.1% at 6 months and 21.2% at 5 years.34) The ORBIT II trial further evaluated the safety and efficacy of orbital atherectomy in a larger sample size.35) It prospectively enrolled 443 consecutive patients with severely calcified coronary lesions across 49 sites in the United States. The study achieved both primary safety and efficacy endpoints and <50% stenosis was achieved in 98.6% of subjects with successful stent delivery in 97.7%. Rates of in-hospital myocardial infarction, cardiac death or target vessel revascularization were 0.7%, 0.2% and 0.7% respectively. There was no significant different in MACE rate between protected left main and non-left main groups at 2 years.36) At 3 years, the cumulative MACE was 23.5% including cardiac death (6.7%), myocardial infarction (11.2%) and target vessel revascularization (10.2%).37) There was no significant difference between subtotal occlusions (≥95% stenosis) and other lesions in all outcomes except higher target vessel revascularization rate in the ≥95% stenosis group (19.1% vs. 7.5%, p=0.004).38) Patients with long (25–40 mm) target lesions had similar outcomes at 3 years except higher rates of myocardial infarction which predominantly occurred during index admission (17.0% vs. 9.0%, p=0.024).39)
The ECLIPSE trial is an ongoing study comparing orbital atherectomy with conventional balloon angioplasty before drug-eluting stent implantation in patients with severe calcified coronary artery disease.40) The trial aims to enroll approximately 2,000 participants. The primary outcome measures include acute minimum stent area by OCT at the end of the procedure and target vessel failure at 1 year, defined as the composite of cardiac death, target vessel related myocardial infarction, or ischemia-driven target vessel revascularization. Enrollment is expected to complete in 2022 with planned follow-up for 2 years.
Excimer laser coronary atherectomy
Excimer laser coronary atherectomy (ELCA), first successfully performed in human in 1988, was initially employed as an alternative to balloon angioplasty in complex coronary lesions.41)42) Its action on atherosclerotic plaque was based on 3 mechanisms, namely photo-chemical, photo-thermal, and photo-mechanical ablations. The impact of pressure pulses generated by ELCA is dependent on the choice of medium—contrast media is associated with the strongest impact, followed by blood and lastly saline.43) While ELCA has limited calcium modifying capacity, its role in calcified coronary lesions lies mainly in tight uncrossable lesions.44)45) Unlike rotational atherectomy and orbital atherectomy, the ELCA device can be advanced over any coronary guidewire and therefore wire exchange using microcatheter is not necessary. Therefore, in lesions already wire crossed but angioplasty balloons nor microcatheter cannot, ELCA passage can increase the luminal area and allow further calcium modification by other devices.
ELCA has mainly been used in treating in-stent restenosis. In the ELLEMENT registry, 28 patients with under-expanded stent despite high-pressure balloon angioplasty underwent ELCA ablation with contrast injection.46) Twenty-five of these patients (89.3%) had calcification in the lesion. ELCA ablation was successful in 27 patients (96.4%) with improvement in luminal area. The use of ELCA in modifying peri-stent calcium related stent under-expansion was further evaluated in a retrospective observational study which included 81 patients who underwent OCT imaging both before and after PCI.47) ELCA use was associated with larger final lumen and stent dimensions.
Intravascular lithotripsy
Intravascular lithotripsy, or lithoplasty, was based on the principle of lithotripsy which has been applied in the management of renal and ureteric calculi for over 3 decades. The use of this technology in coronary intervention was first introduced in 2015. The lithoplasty balloons contain multiple emitters which generate pulsatile sonic pressure waves. During the procedure, these balloons are generally inflated at low pressures ≤4 atm while pulses of sonic pressure waves are delivered to the calcific plaque at a rate of 1 pulse per second. The sonic pressure waves cause vibration which cracks both superficial and deep calcium in the coronary artery. Each balloon can deliver a maximum of 80 pulses. In comparison to atherectomy devices, lithoplasty balloon is more user friendly especially to less experienced operators, with better safety profile due to its low-pressure inflation. Another advantage of lithoplasty is that side branch can be safely protected by guidewire during its action which is not recommended during rotational or orbital atherectomy.
The feasibility of lithoplasty for modification of calcified plaque before stenting was first evaluated in Disrupt CAD I.48) In this prospective single-arm study, 60 patients with severely calcified atherosclerotic plaques were treated with lithoplasty prior to stenting. Stent delivery was successful in all patients, while 95% achieved residual diameter stenosis <50% without in-hospital major adverse cardiac events. At 6 months, rate of major adverse cardiac events was 8.3%. The safety and effectiveness of lithoplasty were further investigated in Disrupt CAD II, a prospective multicenter single-arm post-approval study.49) The trial enrolled 120 patients with severe calcified coronary artery disease from 15 sites across 9 countries. Among 47 patients with post-intervention OCT, calcium fracture was identified in 78.7% of lesions. Non-Q wave myocardial infarctions occurred in 5.8% of patients, with no reported cardiac death, Q wave myocardial infarction or target vessel revascularization. There were also no perforations, abrupt closure, slow flow or no reflow reported. Disrupt CAD III was another prospective single-arm study designed for regulatory approval of lithoplasty use.50) It included 431 patients from 47 sites across 4 countries. Procedural success rate was 92.4%, while 92.2% of patients were free from major adverse cardiovascular events at 30 days. In the OCT substudy which enrolled 100 patients, multiplane and longitudinal calcium fractures were detected in 67.4% of lesions after intravascular lithotripsy.
In a retrospective analysis, 53 patients who received lithoplasty for heavily calcified coronary lesions were compared with 271 patients who underwent rotational atherectomy. While patients who received lithoplasty were more likely to have had acute coronary syndrome, multivessel disease and emergency procedures, there were no statistically significant differences in both in-patient and 30-day outcomes.51)
While clinical trials have demonstrated low rate of major intra-procedural complications such as coronary perforation, major dissection or no-reflow phenomenon, the use of lithoplasty might be limited by the large crossing profile of the balloon catheter as well as cost. In severely stenotic or highly tortuous vessels, prior treatment with conventional balloon angioplasty or event atherectomy might be necessary before lithoplasty.
This novel calcium modifying technique is still being studied despite wide clinical adoption even before any trial data. Some controversial areas in its use include whether more pulses are required (multiple lithotripsy balloons) on difficult calcific lesions, kissing with lithotripsy balloon, use of lithotripsy immediately post-suboptimal drug-eluting stent stenting (anecdotally successful but no well-designed studies have been done to evaluate clinical outcomes), forward effectiveness (use in fracturing proximal chronic total occlusion caps) remain unknown. The authors have experienced both success and failures in using multiple lithoplasty on the same calcified lesion. In the USA, anecdotal reports of utilizing peripheral intravascular lithotripsy balloons in coronary lesions with ability to deliver up to 300 pulses. There are no known predictors of success to help guide practitioners. Lithoplasty in newly deployed drug-eluting stent as bailout has also been performed in our centers with excellent results and no adverse clinical events on long-term follow up. These indications should be further explored and formally investigated in future research.
Specialized (scoring and high pressure) angioplasty balloons
Before the emergence of atherectomy devices, specialized angioplasty balloons have conventionally been the mainstay of pre-stenting treatment for calcified coronary lesions. Cutting balloon (Flextome™ or Wolverine™ has 3 to 4 microsurgical blades [also known as atherotomes]) mounted longitudinally on a non-compliant balloon. During inflation, a cutting balloon can create longitudinal incision through atherosclerotic plaques which permits more effective luminal gain with subsequent conventional non-compliant balloon angioplasty. Other scoring balloons comes in many forms (LaCrosse NSE™, Angiosculpt™ and Scoreflex™): one consists of a semi-compliant balloon encased with 1 or more nitinol scoring wires. When a scoring balloon is inflated, radial force is transmitted through these scoring wires to create incision on atherosclerotic plaques along the coronary artery. Compared with cutting balloon, scoring balloons has better deliverability with a lower crossing profile, and theoretically lower risk of coronary perforation due to its rectangular edges. The scoring wires also reduce balloon slipping (“melon seeding”) during inflation with better anchoring at highly calcified focal lesions. Super high-pressure balloon is a non-compliant balloon with a twin-layered structure which ensures uniform linear expansion and permits inflation pressure of over 35 atm without balloon rupturing. While it has been used for preparation of lesions prior to stenting, although most evidence regarding its use focused on post-stenting optimization. Concerns relate to risk of vessel rupture as compliance/tolerance cannot be measured in vessels during PCI.
The Cutting Balloon Global Randomized Trial evaluated the procedural outcome in 1,238 patients following cutting balloon angioplasty as compared with conventional balloon angioplasty.52) While severely calcified lesions were excluded in this study, it failed to demonstrate any reduction in restenosis rate and difference in acute procedural success. While freedom from target vessel revascularization was slightly higher among patients treated with cutting balloon angioplasty (88.5% vs. 84.6%, log-rank p=0.04), this group also had more coronary perforations (0.8% vs. 0%, p=0.03). More recent retrospective data have also failed to show any significant difference in outcome between cutting balloon angioplasty and other calcium modifying strategies such as rotational atherectomy and conventional balloon angioplasty.53)54) These have shown improved results with combination of rotational atherectomy and scoring balloons.
Data supporting the use of scoring balloon angioplasty in severely calcified lesions came mostly from case series or in vitro studies.55)56)57)58) In an observational study which included 299 consecutive de novo lesions treated with a drug-eluting stent under IVUS guidance, lesion preparation using a scoring balloon was associated with better stent expansion, as compared with direct stenting and conventional balloon angioplasty before stenting. Of note, only 16% of the lesions were calcified.
Case series have reported angiographic success with super high-pressure balloon angioplasty when conventional non-compliant balloons failed to dilate rigid calcific lesions.59)60) The ISAR-CALC study is a randomized open-label trial comparing stent expansion following super high-pressure balloon or scoring balloon angioplasty in severely calcified lesions which were unsuccessfully opened with conventional non-compliant balloons.61) The study enrolled 74 patients, with OCT imaging available in 70 of them. Super high-pressure balloon angioplasty achieved greater minimum lumen diameter (2.83 mm vs. 2.65 mm, p=0.03) with less diameter stenosis (11.6% vs. 14.4%, p=0.02), compared with scoring balloons. However, the 2 strategies were associated with comparable stent expansion and procedural success rates. Both groups reported one coronary perforation and zero in-hospital cardiac death.
SPECIFIC STRATEGIES IN CALCIUM MODIFICATION
Rotational vs. orbital atherectomy
Since the introduction of orbital atherectomy, there have been ongoing discussions on the optimal choice of atherectomy device in severely calcified coronary lesions. A meta-analysis including 8 observational trials and a total of 4,332 patients demonstrated no significant difference in overall all-cause death, major adverse cardiac events, myocardial infarction and target vessel revascularization between rotational and orbital atherectomy.62) The analysis did, however, report a higher rate of coronary dissections (odds ratio [OR], 2.61, p=0.003) and perforations (OR, 2.79, p=0.03) among patients treated with orbital atherectomy. It is unclear if these risks are device or operator technique related.
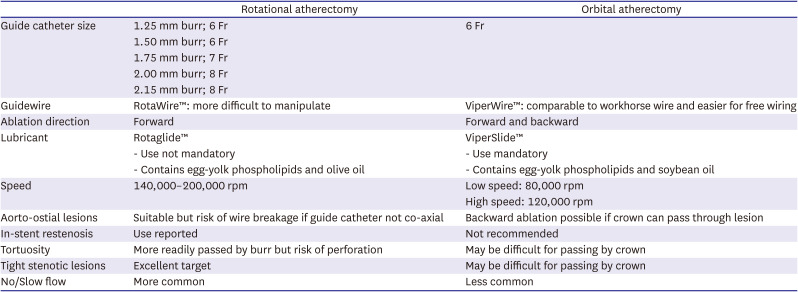
To date, there is no large-scale randomized data comparing the use of rotational and orbital atherectomy in severely calcified lesions. This is in part due to the heterogenicity of calcified lesions in terms of calcium thickness, depth, distribution and eccentricity, lesion length and location within the coronary arteries. All these factors would affect the behavior of calcified plaque during the procedure and the outcome of calcium modification. Each atherectomy device also has its specific advantages and disadvantages. Therefore, it appears logical that there is unlikely a universally superior device for all calcified lesions. Instead, the optimal choice of atherectomy device should be based on characteristics of individual lesion and device. Table 2 illustrates and compares the different features of rotational and orbital atherectomy.
Table 2
Comparison of rotational atherectomy versus orbital atherectomy
Atherectomy and lithoplasty
With the emergence of intravascular lithotripsy, the landscape of coronary calcium modification has changed dramatically. While lithoplasty is effective against deep calcium, it might be challenging to deliver lithoplasty balloons in highly stenotic lesions without prior preparation given the large crossing profile. The upfront use of atherectomy to debulk thick calcium ring followed by lithoplasty to fracture the calcium has been described in case report and small series.63)64)65)66) After initial lesion preparation with either rotational or orbital atherectomy, delivery of lithoplasty balloon is enhanced and calcium fracture can be achieved at low inflation pressure with intravascular lithotripsy. Both Rota-Shock (rotational atherectomy followed by lithoplasty) and Orbital-Tripsy (orbital atherectomy followed by lithoplasty) appear to be feasible and safe with the limited current evidence, and more high-quality data from large-scale clinical trials is warranted.
CONCLUSION
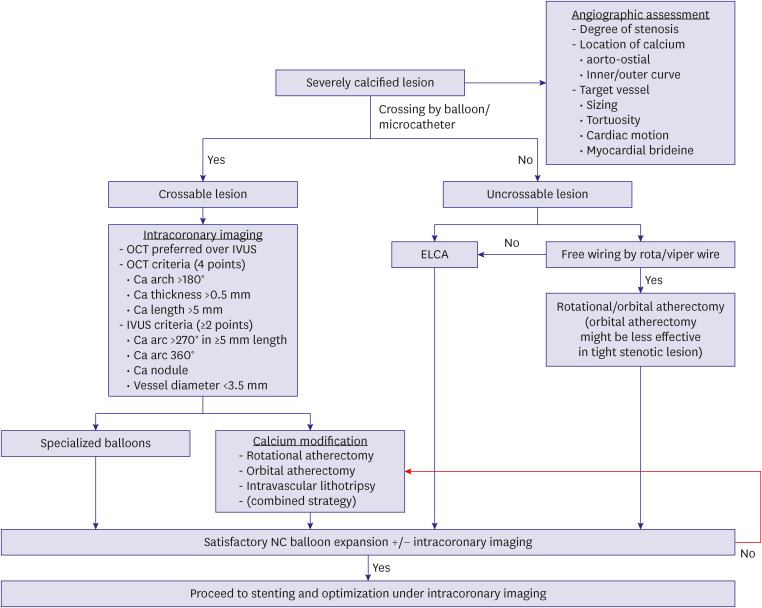
Management of calcific coronary artery disease has been one of the greatest challenges in coronary intervention. The advancement of intravascular imaging and emergence of new calcium modifying techniques have changed the landscape of coronary calcium management. A stepwise algorithm on the management of severely calcific coronary lesions is illustrated in Figure 1. While the optimal choice of calcium modifying techniques remains controversial, operators should base their decision on the characteristics of individual lesion according to imaging findings. In tight stenotic lesions not crossable by microcatheter or small semi-compliant balloons, ELCA can be considered if available. Free wiring with RotaWire or ViperWire might sometimes be possible, although orbital atherectomy could be less effective in highly stenotic lesions. While intracoronary imaging could evaluate the result of calcium modification following atherectomy and angioplasty, it does not replace non-compliant balloon angioplasty which provide direct evidence on expandability of lesion.
Figure 1
Management algorithm for severely calcified lesion.
ELCA = excimer laser coronary atherectomy; IVUS = intravascular ultrasound; NC = non-compliant; OCT = optical coherence tomography.
Overall, high-quality randomized data on individual calcium modifying technique and different proposed management algorithms remains limited. Future trials should provide insight on a comprehensive evidence-based approach to the optimal management of calcific coronary artery disease.
 XML Download
XML Download