

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Left main coronary artery disease (LMCAD) represents the highest-risk anatomical subset of atherosclerotic obstructive coronary artery disease (CAD), carrying important prognostic impact owing to the large area of myocardial at risk.1) LMCAD is not uncommon in daily clinical practice, and its clinical relevance and anatomical complexities are gradually increasing over the past decades.2) On the basis of early reports from a half century ago, LMCAD treated with medical therapy alone had a very poor prognosis, with a 5-year survival of less than 50%.3)4)5) Meanwhile, in the recent report from the International Study of Comparative Health Effectiveness With Medical and Invasive Approaches (ISCHEMIA) trial, invasive revascularization in patients with intermediate (25–49%) left main coronary artery (LMCA) stenosis resulted in a greater risk reduction of nonprocedural myocardial infarction (MI) with no significant difference for the hard composite endpoint when compared with conservative management.6) Current clinical practice guidelines usually recommend myocardial revascularization in patients with ≥50% LMCA stenosis,7) and the optimal revascularization strategy is essential in the treatment of significant LMCAD.
Historically, coronary artery bypass grafting (CABG) was developed and technically matured earlier than percutaneous coronary intervention (PCI).8) For a long time, CABG has been regarded as the “gold standard” for treating LMCAD owing to its proven mortality benefit over medical therapy. In earlier period of interventional cardiology practice, PCI for unprotected LMCAD was reserved only for selected patients with high surgical risk or hemodynamic instability.9) However, with notable advances in the field of PCI including stent technology, complex PCI techniques, supportive devices or adjunctive antithrombotic drugs, PCI has become a viable option for a sizable majority of patients with LMCAD who are equally suitable for CABG or PCI.1) Until recently, several randomized controlled trials (RCTs) have evaluated the clinical outcomes of PCI with stenting in comparison with standard CABG for LMCAD.10) In current clinical practice, the optimal revascularization strategy of patients with LMCAD is guided by several clinical and anatomical factors; therefore, the role of the Heart Team in decision-making is emphasized more than ever. In this review article, we sought to provide an up-to-date knowledge of revascularization strategies for the treatment of LMCAD, specifically on the comparison of contemporary PCI with CABG. We also discussed contemporary evidence gaps, unmet needs, and future perspectives on the left main revascularization.
Go to : 
HISTORY OF THE EVOLUTION OF CORONARY ARTERY BYPASS GRAFTING AND PERCUTANEOUS CORONARY INTERVENTION FOR LEFT MAIN CORONARY ARTERY DISEASE
The timelines of the important milestones of PCI and CABG and landmark trials comparing PCI versus CABG for LMCAD revascularization are shown in Figure 1. Although it continues to evolve, CABG surgery, as it is known today—using the left internal mammary artery (LIMA) conduit to the left anterior descending artery (LAD)—was first performed in the late 1960s. CABG was implemented to treat CAD in the 1970s.11) Superior late outcomes associated with the use of LIMA grafts were already reported in the early 1980s.3)12) CABG has been the gold standard treatment since RCTs conducted 30–40 years ago have demonstrated the 5- to 10-year survival benefit of CABG over medical treatment in patients with LMCAD.13)14)15)16)
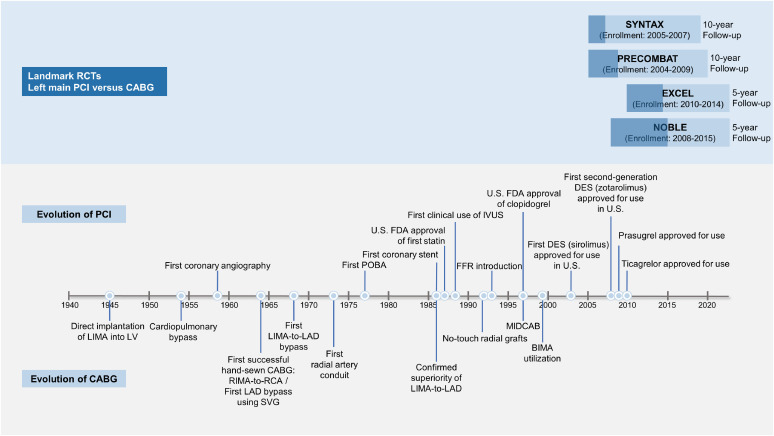 | Figure 1Timelines of important milestones of PCI and CABG and landmark trials comparing PCI versus CABG for left main revascularization.BIMA = bilateral internal mammary artery; CABG = coronary artery bypass grafting; DES = drug-eluting stents; EXCEL = Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; FDA = Food and Drug Administration; FFR = fractional flow reserve; IVUS = intravascular ultrasound; LAD = left anterior descending artery; LIMA = left internal mammary artery; LV = left ventricular; MIDCAB = minimally invasive direct coronary artery bypass; NOBLE = Nordic-Baltic-British left main revascularization; PCI = percutaneous coronary intervention; POBA = plain old balloon angioplasty; PRECOMBAT = Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease; RCA = right coronary artery; RCT = randomized clinical trial; RIMA = right internal mammary artery; SVG = saphenous vein graft; SYNTAX = Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery.
|
In 1977, Dr. Andreas Gruentzig performed the first PCI using balloon angioplasty.17) Unfortunately, in the first case series, the plain balloon angioplasty had poor long-term outcomes with high risks of death and restenosis in patients with unprotected LMCAD.18) Thereafter, given CABG has been the first choice for left main revascularization for almost more than two decades, PCI using balloon angioplasty has been performed on a highly limited basis, such as for salvage if surgically ineligible. In the mid-1990s, PCI overcame the shortcomings of balloon angioplasty with the introduction of coronary stents and dual antiplatelet therapy (DAPT), making it a revisited treatment option for LMCAD on a limited basis. PCI using bare-metal stents (BMS) was performed in highly selected low-risk patients with LMCAD; clinical studies showed acceptable short- and midterm clinical outcomes.19)20) In the early 2000s, drug-eluting stents (DES) were widely adopted in the clinical practice, which significantly reduced restenosis and repeat revascularization. Several observational studies have shown that PCI for LMCAD with early-generation DES has more favorable outcomes than with BMS.21)22) The introduction of second-generation DES in the late 2000s further reduced the risk of restenosis and stent thrombosis.23)24) In the contemporary PCI era, PCI for LMCAD has been increasingly performed for a diverse clinical or anatomical spectrum of patients. Not surprisingly, at each milestone of advances in PCI, PCI has been tested against the “gold standard” CABG (Figure 1).
Go to :
CLINICAL EVIDENCE ON PERCUTANEOUS CORONARY INTERVENTION VERSUS CORONARY ARTERY BYPASS GRAFTING FOR LEFT MAIN CORONARY ARTERY DISEASE
Randomized clinical trials
Table 1 provides an overview of the key features and primary results of RCTs comparing PCI using DES vs. CABG for patients with unprotected LMCAD.25)26)27)28)29)30)31)32)33)34)35)36)37) The Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery (SYNTAX) trial was the first RCT with adequate statistical power to compare PCI with CABG in the modern era. The SYNTAX trial included 705 patients with LMCAD and a range of complex diseases, and PCI had comparable composite endpoints with CABG in this subgroup with LMCAD.28)29) However, in a stratified analysis according to the baseline SYNTAX score, the risks of major adverse cardiac and cerebrovascular events (MACCEs) and cardiac mortality at 5 years were higher with PCI in those with LMCAD and high anatomical complexity, defined as a SYNTAX score of ≥33.29) This results became the foundation for the design of future trials specifically targeting on patients with LMCAD. Subsequently, in the Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease (PRECOMBAT) trial (n=600), the risk of MACCEs was comparable between PCI and CABG; however, it had wide noninferiority margin and a relatively limited number of patients and clinical events.32) In recent reports of 10-year extended follow-up of SYNTAX and PRECOMBAT, PCI and CABG showed comparable clinical outcomes in terms of all-cause mortality or hard clinical endpoints.30)33)
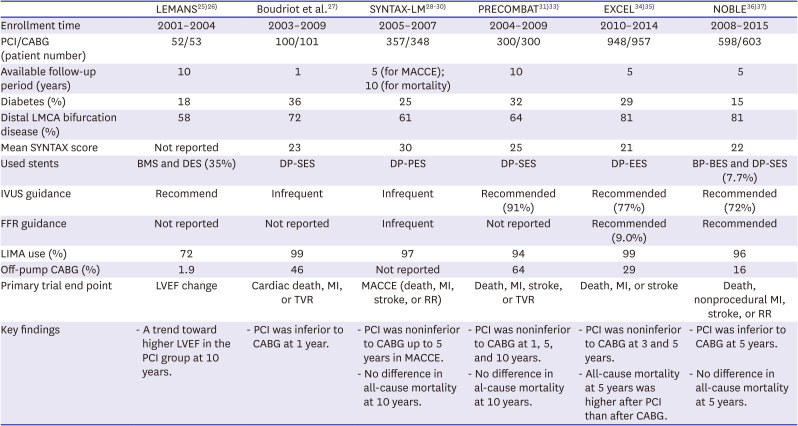
Table 1
Key randomized clinical trials comparing PCI versus CABG for LMCAD
| LEMANS25)26) | Boudriot et al.27) | SYNTAX-LM28)29)30) | PRECOMBAT31)33) | EXCEL34)35) | NOBLE36)37) | |
|---|---|---|---|---|---|---|
| Enrollment time | 2001–2004 | 2003–2009 | 2005–2007 | 2004–2009 | 2010–2014 | 2008–2015 |
| PCI/CABG (patient number) | 52/53 | 100/101 | 357/348 | 300/300 | 948/957 | 598/603 |
| Available follow-up period (years) | 10 | 1 | 5 (for MACCE); 10 (for mortality) | 10 | 5 | 5 |
| Diabetes (%) | 18 | 36 | 25 | 32 | 29 | 15 |
| Distal LMCA bifurcation disease (%) | 58 | 72 | 61 | 64 | 81 | 81 |
| Mean SYNTAX score | Not reported | 23 | 30 | 25 | 21 | 22 |
| Used stents | BMS and DES (35%) | DP-SES | DP-PES | DP-SES | DP-EES | BP-BES and DP-SES (7.7%) |
| IVUS guidance | Recommend | Infrequent | Infrequent | Recommended (91%) | Recommended (77%) | Recommended (72%) |
| FFR guidance | Not reported | Not reported | Infrequent | Not reported | Recommended (9.0%) | Recommended |
| LIMA use (%) | 72 | 99 | 97 | 94 | 99 | 96 |
| Off-pump CABG (%) | 1.9 | 46 | Not reported | 64 | 29 | 16 |
| Primary trial end point | LVEF change | Cardiac death, MI, or TVR | MACCE (death, MI, stroke, or RR) | Death, MI, stroke, or TVR | Death, MI, or stroke | Death, nonprocedural MI, stroke, or RR |
| Key findings | - A trend toward higher LVEF in the PCI group at 10 years. | - PCI was inferior to CABG at 1 year. | - PCI was noninferior to CABG up to 5 years in MACCE. | - PCI was noninferior to CABG at 1, 5, and 10 years. | - PCI was noninferior to CABG at 3 and 5 years. | - PCI was inferior to CABG at 5 years. |
| - No difference in all-cause mortality at 10 years. | - No difference in al-cause mortality at 10 years. | - All-cause mortality at 5 years was higher after PCI than after CABG. | - No difference in all-cause mortality at 5 years. |
BMS = bare-metal stent; BP-BES = biodegradable-polymer biolimus-eluting-stent; CABG = coronary artery bypass grafting; DES = drug-eluting stent; DP-EES = durable-polymer everolimus-eluting-stent; DP-PES = durable-polymer paclitaxel-eluting-stent; DP-SES = durable-polymer sirolimus-eluting-stent; EXCEL = Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; FFR = fractional flow reserve; LEMANS = Left Main Stenting; LIMA = left internal mammary artery; LVEF = left ventricular ejection fraction; MACCE = major adverse cardiac or cerebrovascular event; MI = myocardial infraction; NOBLE = Nordic-Baltic-British left main revascularization; PCI = percutaneous coronary intervention; PRECOMBAT = Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease; RR = repeat revascularization; SYNTAX = Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery; TVR = target vessel revascularization.
![]()
To date, only 2 RCTs, the Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL) and the Nordic-Baltic-British left main revascularization (NOBLE), have evaluated the clinical outcomes of state-of-the-art PCI with contemporary DES versus contemporary CABG for LMCAD.34)35)36)37) Recently, the 5-year results of EXCEL and NOBLE trials were reported. However, conflicting results from these 2 RCTs have ignited huge debate in the cardiovascular community: EXCEL reported that PCI is noninferior to CABG in terms of all-cause death, MI, or stroke,34)35) whereas NOBLE failed to show noninferiority of PCI to CABG in terms of their primary composite endpoint of all-cause death, nonprocedural MI, stroke, or repeat revascularization.36)37) The detailed results and related controversies of EXCEL and NOBLE trials are summarized in Table 2. In addition, longer-term follow-up of EXCEL and NOBLE has alarmed late catch-up or diverging event rates favoring CABG over PCI during late periods of follow-up. Considering that the advantages of CABG over PCI tend to become more pronounced over a longer follow-up,38) longer-term follow-up (10 years) results from these RCTs are necessary to draw definitive conclusions on the relative long-term durability of PCI and CABG for LMCAD.
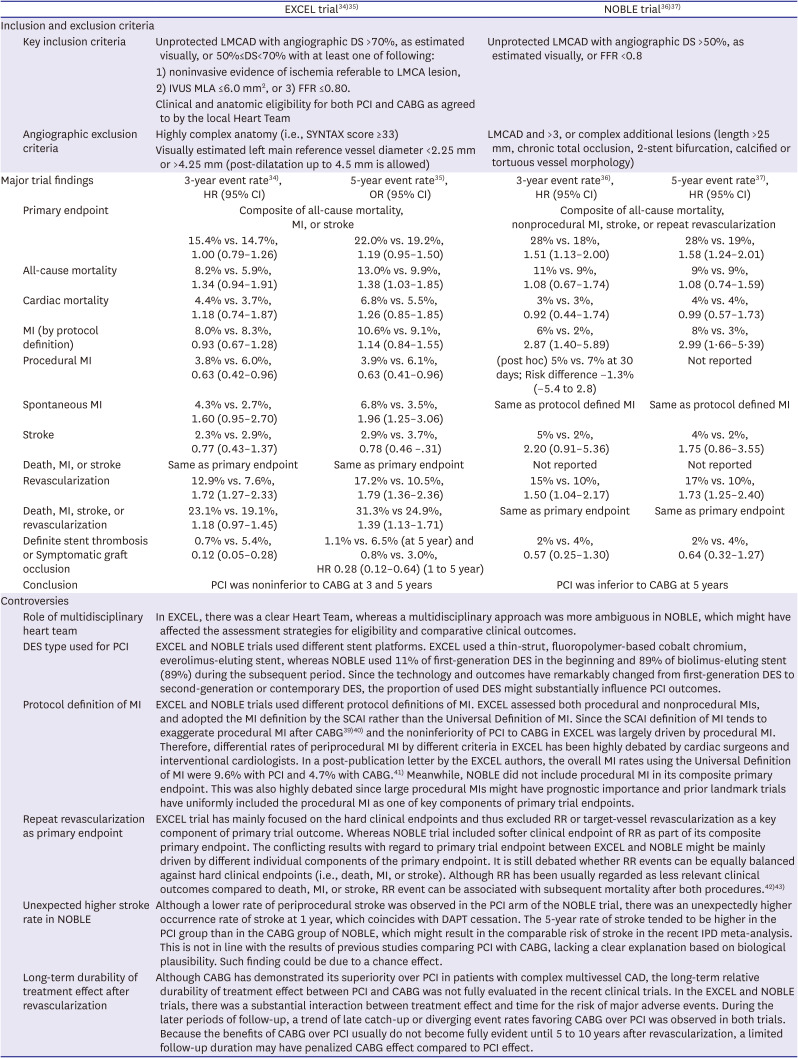
Table 2
Major features and controversies of EXCEL and NOBLE trials
| EXCEL trial34)35) | NOBLE trial36)37) | ||||
|---|---|---|---|---|---|
| Inclusion and exclusion criteria | |||||
| Key inclusion criteria | Unprotected LMCAD with angiographic DS >70%, as estimated visually, or 50%≤DS<70% with at least one of following: 1) noninvasive evidence of ischemia referable to LMCA lesion, 2) IVUS MLA ≤6.0 mm2, or 3) FFR ≤0.80. | Unprotected LMCAD with angiographic DS >50%, as estimated visually, or FFR <0.8 | |||
| Clinical and anatomic eligibility for both PCI and CABG as agreed to by the local Heart Team | |||||
| Angiographic exclusion criteria | Highly complex anatomy (i.e., SYNTAX score ≥33) | LMCAD and >3, or complex additional lesions (length >25 mm, chronic total occlusion, 2-stent bifurcation, calcified or tortuous vessel morphology) | |||
| Visually estimated left main reference vessel diameter <2.25 mm or >4.25 mm (post-dilatation up to 4.5 mm is allowed) | |||||
| Major trial findings | 3-year event rate34), HR (95% CI) | 5-year event rate35), OR (95% CI) | 3-year event rate36), HR (95% CI) | 5-year event rate37), HR (95% CI) | |
| Primary endpoint | Composite of all-cause mortality, MI, or stroke | Composite of all-cause mortality, nonprocedural MI, stroke, or repeat revascularization | |||
| 15.4% vs. 14.7%, 1.00 (0.79–1.26) | 22.0% vs. 19.2%, 1.19 (0.95–1.50) | 28% vs. 18%, 1.51 (1.13–2.00) | 28% vs. 19%, 1.58 (1.24–2.01) | ||
| All-cause mortality | 8.2% vs. 5.9%, 1.34 (0.94–1.91) | 13.0% vs. 9.9%, 1.38 (1.03–1.85) | 11% vs. 9%, 1.08 (0.67–1.74) | 9% vs. 9%, 1.08 (0.74–1.59) | |
| Cardiac mortality | 4.4% vs. 3.7%, 1.18 (0.74–1.87) | 6.8% vs. 5.5%, 1.26 (0.85–1.85) | 3% vs. 3%, 0.92 (0.44–1.74) | 4% vs. 4%, 0.99 (0.57–1.73) | |
| MI (by protocol definition) | 8.0% vs. 8.3%, 0.93 (0.67–1.28) | 10.6% vs. 9.1%, 1.14 (0.84–1.55) | 6% vs. 2%, 2.87 (1.40–5.89) | 8% vs. 3%, 2.99 (1·66–5·39) | |
| Procedural MI | 3.8% vs. 6.0%, 0.63 (0.42–0.96) | 3.9% vs. 6.1%, 0.63 (0.41–0.96) | (post hoc) 5% vs. 7% at 30 days; Risk difference −1.3% (−5.4 to 2.8) | Not reported | |
| Spontaneous MI | 4.3% vs. 2.7%, 1.60 (0.95–2.70) | 6.8% vs. 3.5%, 1.96 (1.25–3.06) | Same as protocol defined MI | Same as protocol defined MI | |
| Stroke | 2.3% vs. 2.9%, 0.77 (0.43–1.37) | 2.9% vs. 3.7%, 0.78 (0.46 –.31) | 5% vs. 2%, 2.20 (0.91–5.36) | 4% vs. 2%, 1.75 (0.86–3.55) | |
| Death, MI, or stroke | Same as primary endpoint | Same as primary endpoint | Not reported | Not reported | |
| Revascularization | 12.9% vs. 7.6%, 1.72 (1.27–2.33) | 17.2% vs. 10.5%, 1.79 (1.36–2.36) | 15% vs. 10%, 1.50 (1.04–2.17) | 17% vs. 10%, 1.73 (1.25–2.40) | |
| Death, MI, stroke, or revascularization | 23.1% vs. 19.1%, 1.18 (0.97–1.45) | 31.3% vs 24.9%, 1.39 (1.13–1.71) | Same as primary endpoint | Same as primary endpoint | |
| Definite stent thrombosis or Symptomatic graft occlusion | 0.7% vs. 5.4%, 0.12 (0.05–0.28) | 1.1% vs. 6.5% (at 5 year) and 0.8% vs. 3.0%, HR 0.28 (0.12–0.64) (1 to 5 year) | 2% vs. 4%, 0.57 (0.25–1.30) | 2% vs. 4%, 0.64 (0.32–1.27) | |
| Conclusion | PCI was noninferior to CABG at 3 and 5 years | PCI was inferior to CABG at 5 years | |||
| Controversies | |||||
| Role of multidisciplinary heart team | In EXCEL, there was a clear Heart Team, whereas a multidisciplinary approach was more ambiguous in NOBLE, which might have affected the assessment strategies for eligibility and comparative clinical outcomes. | ||||
| DES type used for PCI | EXCEL and NOBLE trials used different stent platforms. EXCEL used a thin-strut, fluoropolymer-based cobalt chromium, everolimus-eluting stent, whereas NOBLE used 11% of first-generation DES in the beginning and 89% of biolimus-eluting stent (89%) during the subsequent period. Since the technology and outcomes have remarkably changed from first-generation DES to second-generation or contemporary DES, the proportion of used DES might substantially influence PCI outcomes. | ||||
| Protocol definition of MI | EXCEL and NOBLE trials used different protocol definitions of MI. EXCEL assessed both procedural and nonprocedural MIs, and adopted the MI definition by the SCAI rather than the Universal Definition of MI. Since the SCAI definition of MI tends to exaggerate procedural MI after CABG39)40) and the noninferiority of PCI to CABG in EXCEL was largely driven by procedural MI. Therefore, differential rates of periprocedural MI by different criteria in EXCEL has been highly debated by cardiac surgeons and interventional cardiologists. In a post-publication letter by the EXCEL authors, the overall MI rates using the Universal Definition of MI were 9.6% with PCI and 4.7% with CABG.41) Meanwhile, NOBLE did not include procedural MI in its composite primary endpoint. This was also highly debated since large procedural MIs might have prognostic importance and prior landmark trials have uniformly included the procedural MI as one of key components of primary trial endpoints. | ||||
| Repeat revascularization as primary endpoint | EXCEL trial has mainly focused on the hard clinical endpoints and thus excluded RR or target-vessel revascularization as a key component of primary trial outcome. Whereas NOBLE trial included softer clinical endpoint of RR as part of its composite primary endpoint. The conflicting results with regard to primary trial endpoint between EXCEL and NOBLE might be mainly driven by different individual components of the primary endpoint. It is still debated whether RR events can be equally balanced against hard clinical endpoints (i.e., death, MI, or stroke). Although RR has been usually regarded as less relevant clinical outcomes compared to death, MI, or stroke, RR event can be associated with subsequent mortality after both procedures.42)43) | ||||
| Unexpected higher stroke rate in NOBLE | Although a lower rate of periprocedural stroke was observed in the PCI arm of the NOBLE trial, there was an unexpectedly higher occurrence rate of stroke at 1 year, which coincides with DAPT cessation. The 5-year rate of stroke tended to be higher in the PCI group than in the CABG group of NOBLE, which might result in the comparable risk of stroke in the recent IPD meta-analysis. This is not in line with the results of previous studies comparing PCI with CABG, lacking a clear explanation based on biological plausibility. Such finding could be due to a chance effect. | ||||
| Long-term durability of treatment effect after revascularization | Although CABG has demonstrated its superiority over PCI in patients with complex multivessel CAD, the long-term relative durability of treatment effect between PCI and CABG was not fully evaluated in the recent clinical trials. In the EXCEL and NOBLE trials, there was a substantial interaction between treatment effect and time for the risk of major adverse events. During the later periods of follow-up, a trend of late catch-up or diverging event rates favoring CABG over PCI was observed in both trials. Because the benefits of CABG over PCI usually do not become fully evident until 5 to 10 years after revascularization, a limited follow-up duration may have penalized CABG effect compared to PCI effect. | ||||
CABG = coronary artery bypass grafting; CAD = coronary artery disease; DES = drug-eluting stent; DAPT = dual antiplatelet therapy; DS = diameter stenosis; EXCEL = Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization; FFR = fractional flow reserve; HR = hazard ratio; IPD = individual patient data; IVUS = intravascular ultrasound; LMCAD = left main coronary artery disease; MI = myocardial infarction; MLA = minimal lumen area; NOBLE = Nordic-Baltic-British left main revascularization; OR = odd ratio; PCI = percutaneous coronary intervention; RR = repeat revascularization; SCAI = Society for Cardiovascular Angiography and Interventions.
![]()
Updated meta-analyses of percutaneous coronary intervention following the EXCEL and NOBLE trials
Not surprisingly, several trial-level or individual patient-level meta-analyses incorporating different combinations of trials of LMCAD have been published (Table 3).44)45)46)47)48)49)50) These analyses generally reported comparable hard clinical outcomes, such as long-term mortality and a composite endpoint of death, MI, or stroke. Recently, the Thrombolysis in Myocardial Infarction (TIMI) group performed an independent individual patient data (IPD) pooled meta-analysis of the long-term follow-up results of 4 key RCTs (i.e., SYNTAX, PRECOMBAT, EXCEL, and NOBLE) comparing PCI with DES with CABG for LMCAD (4,394 randomized patients).50) In this analysis, no significant difference was found in all-cause mortality between PCI and CABG up to 5–10 years of follow-up. All-cause mortality difference was likely less than 0.2%/year by Bayesian analysis. A closer look at each outcome of this meta-analysis could be helpful to guide the decision-making for whom both PCI and CABG are equipoised (both PCI and CABG are reasonable options). The risk of spontaneous MI was reduced after CABG, whereas the risk of procedural MI was lower after PCI with prespecified protocol definitions from each trial. Compared with CABG, PCI was associated with a small reduction in procedural stroke, but the difference was no longer significant by 5 years. The risk of repeat revascularization was higher after PCI than after CABG.
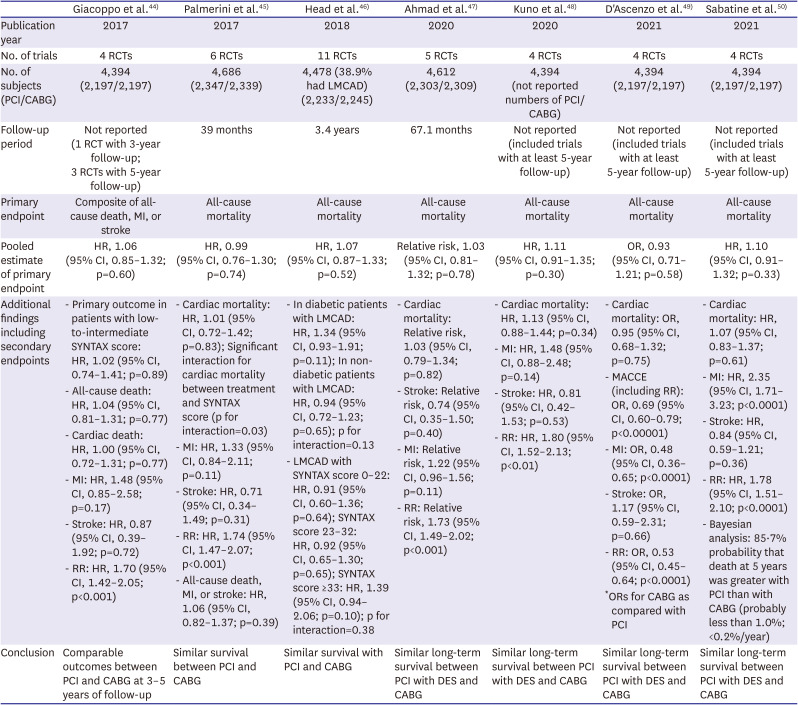
Table 3
| Giacoppo et al.44) | Palmerini et al.45) | Head et al.46) | Ahmad et al.47) | Kuno et al.48) | D'Ascenzo et al.49) | Sabatine et al.50) | |
|---|---|---|---|---|---|---|---|
| Publication year | 2017 | 2017 | 2018 | 2020 | 2020 | 2021 | 2021 |
| No. of trials | 4 RCTs | 6 RCTs | 11 RCTs | 5 RCTs | 4 RCTs | 4 RCTs | 4 RCTs |
| No. of subjects (PCI/CABG) | 4,394 (2,197/2,197) | 4,686 (2,347/2,339) | 4,478 (38.9% had LMCAD) (2,233/2,245) | 4,612 (2,303/2,309) | 4,394 (not reported numbers of PCI/CABG) | 4,394 (2,197/2,197) | 4,394 (2,197/2,197) |
| Follow-up period | Not reported (1 RCT with 3-year follow-up; 3 RCTs with 5-year follow-up) | 39 months | 3.4 years | 67.1 months | Not reported (included trials with at least 5-year follow-up) | Not reported (included trials with at least 5-year follow-up) | Not reported (included trials with at least 5-year follow-up) |
| Primary endpoint | Composite of all-cause death, MI, or stroke | All-cause mortality | All-cause mortality | All-cause mortality | All-cause mortality | All-cause mortality | All-cause mortality |
| Pooled estimate of primary endpoint | HR, 1.06 (95% CI, 0.85–1.32; p=0.60) | HR, 0.99 (95% CI, 0.76–1.30; p=0.74) | HR, 1.07 (95% CI, 0.87–1.33; p=0.52) | Relative risk, 1.03 (95% CI, 0.81–1.32; p=0.78) | HR, 1.11 (95% CI, 0.91–1.35; p=0.30) | OR, 0.93 (95% CI, 0.71–1.21; p=0.58) | HR, 1.10 (95% CI, 0.91–1.32; p=0.33) |
| Additional findings including secondary endpoints | - Primary outcome in patients with low-to-intermediate SYNTAX score: HR, 1.02 (95% CI, 0.74–1.41; p=0.89) | - Cardiac mortality: HR, 1.01 (95% CI, 0.72–1.42; p=0.83); Significant interaction for cardiac mortality between treatment and SYNTAX score (p for interaction=0.03) | - In diabetic patients with LMCAD: HR, 1.34 (95% CI, 0.93–1.91; p=0.11); In non-diabetic patients with LMCAD: HR, 0.94 (95% CI, 0.72–1.23; p=0.65); p for interaction=0.13 | - Cardiac mortality: Relative risk, 1.03 (95% CI, 0.79–1.34; p=0.82) | - Cardiac mortality: HR, 1.13 (95% CI, 0.88–1.44; p=0.34) | - Cardiac mortality: OR, 0.95 (95% CI, 0.68–1.32; p=0.75) | - Cardiac mortality: HR, 1.07 (95% CI, 0.83–1.37; p=0.61) |
| - All-cause death: HR, 1.04 (95% CI, 0.81–1.31; p=0.77) | - MI: HR, 1.33 (95% CI, 0.84–2.11; p=0.11) | - LMCAD with SYNTAX score 0–22: HR, 0.91 (95% CI, 0.60–1.36; p=0.64); SYNTAX score 23–32: HR, 0.92 (95% CI, 0.65–1.30; p=0.65); SYNTAX score ≥33: HR, 1.39 (95% CI, 0.94–2.06; p=0.10); p for interaction=0.38 | - Stroke: Relative risk, 0.74 (95% CI, 0.35–1.50; p=0.40) | - MI: HR, 1.48 (95% CI, 0.88–2.48; p=0.14) | - MACCE (including RR): OR, 0.69 (95% CI, 0.60–0.79; p<0.00001) | - MI: HR, 2.35 (95% CI, 1.71–3.23; p<0.0001) | |
| - Cardiac death: HR, 1.00 (95% CI, 0.72–1.31; p=0.77) | - Stroke: HR, 0.71 (95% CI, 0.34–1.49; p=0.31) | - MI: Relative risk, 1.22 (95% CI, 0.96–1.56; p=0.11) | - Stroke: HR, 0.81 (95% CI, 0.42–1.53; p=0.53) | - MI: OR, 0.48 (95% CI, 0.36–0.65; p<0.0001) | - Stroke: HR, 0.84 (95% CI, 0.59–1.21; p=0.36) | ||
| - MI: HR, 1.48 (95% CI, 0.85–2.58; p=0.17) | - RR: HR, 1.74 (95% CI, 1.47–2.07; p<0.001) | - RR: Relative risk, 1.73 (95% CI, 1.49–2.02; p<0.001) | - RR: HR, 1.80 (95% CI, 1.52–2.13; p<0.01) | - Stroke: OR, 1.17 (95% CI, 0.59–2.31; p=0.66) | - RR: HR, 1.78 (95% CI, 1.51–2.10; p<0.0001) | ||
| - Stroke: HR, 0.87 (95% CI, 0.39–1.92; p=0.72) | - All-cause death, MI, or stroke: HR, 1.06 (95% CI, 0.82–1.37; p=0.39) | - RR: OR, 0.53 (95% CI, 0.45–0.64; p<0.0001) | - Bayesian analysis: 85·7% probability that death at 5 years was greater with PCI than with CABG (probably less than 1.0%; <0.2%/year) | ||||
| - RR: HR, 1.70 (95% CI, 1.42–2.05; p<0.001) | *ORs for CABG as compared with PCI | ||||||
| Conclusion | Comparable outcomes between PCI and CABG at 3–5 years of follow-up | Similar survival between PCI and CABG | Similar survival with PCI and CABG | Similar long-term survival between PCI with DES and CABG | Similar long-term survival between PCI with DES and CABG | Similar long-term survival between PCI with DES and CABG | Similar long-term survival between PCI with DES and CABG |
CABG = coronary artery bypass grafting; CI = confidence interval; DES = drug-eluting stent; HR = hazard ratio; MI = myocardial infraction; PCI = percutaneous coronary intervention; LMCAD = left main coronary artery disease; MI = myocardial infarction; OR = odd ratio; RCT = randomized clinical trial; RR = repeat revascularization.
![]()
In summary, CABG and PCI with DES for the treatment of LMCAD have comparable risks for overall mortality up to 5–10 years of follow-up based on the totality of currently available evidence. The early benefit of PCI over CABG in terms of lower procedural MI and stroke risks is eventually offset by higher risks of spontaneous MI and repeat revascularization during long-term follow-up.
Current guidelines on the left main revascularization
Over the last decades, CABG has been a gold standard for left main revascularization, reflected in class I A indication in all patients with LMCAD irrespective of anatomical complexity by European and US guidelines. In recent years, PCI has become a reasonable alternative in selected patients with less complex LMCAD, with remarkable progress and evidence accumulation in the field of PCI. Table 4 summarizes the major changes on European or US guideline recommendations on LMCAD over last decade. In the most recent 2018 European guidelines after the publication of EXCEL and NOBLE trials, PCI still has class I, IIa, or III indications for treatment of LMCAD according to the SYNTAX score tertiles, although corresponding levels of evidence have been upgraded from B to A.51)52) Contrary to the European guidelines, the US guidelines have given stricter recommendations for PCI for LMCAD. In the 2014 US guidelines, PCI was recommended as a class IIa B indication for patients with low anatomical risk (e.g., a low SYNTAX score of ≤22, ostial/shaft LMCAD), a class IIb B indication for those with intermediate anatomical risk (e.g., low-to-intermediate SYNTAX score of <33, bifurcation LMCAD), and a class III B indication for those with unfavorable anatomy (e.g., SYNTAX score ≥33).53) The most updated 2021 American College of Cardiology (ACC)/American Heart Association (AHA)/Society for Cardiovascular Angiography & Interventions (SCAI) guidelines for coronary revascularization gave a more unified class IIa B recommendation to PCI for LMCAD in selected patients for whom PCI can provide equivalent revascularization to that possible with CABG, without mention of anatomical complexity stratification.54) We expect further changes in European guidelines soon.
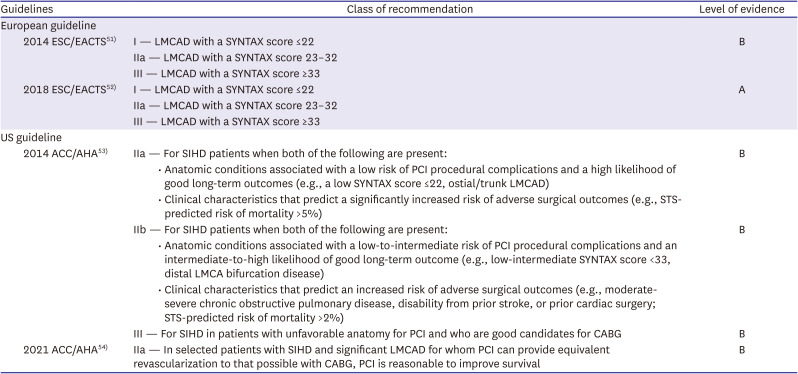
Table 4
Recent clinical guideline changes for left main revascularization
| Guidelines | Class of recommendation | Level of evidence | ||
|---|---|---|---|---|
| European guideline | ||||
| 2014 ESC/EACTS51) | I — LMCAD with a SYNTAX score ≤22 | B | ||
| IIa — LMCAD with a SYNTAX score 23–32 | ||||
| III — LMCAD with a SYNTAX score ≥33 | ||||
| 2018 ESC/EACTS52) | I — LMCAD with a SYNTAX score ≤22 | A | ||
| IIa — LMCAD with a SYNTAX score 23–32 | ||||
| III — LMCAD with a SYNTAX score ≥33 | ||||
| US guideline | ||||
| 2014 ACC/AHA53) | IIa — For SIHD patients when both of the following are present: | B | ||
| • Anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of good long-term outcomes (e.g., a low SYNTAX score ≤22, ostial/trunk LMCAD) | ||||
| • Clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (e.g., STS-predicted risk of mortality >5%) | ||||
| IIb — For SIHD patients when both of the following are present: | B | |||
| • Anatomic conditions associated with a low-to-intermediate risk of PCI procedural complications and an intermediate-to-high likelihood of good long-term outcome (e.g., low-intermediate SYNTAX score <33, distal LMCA bifurcation disease) | ||||
| • Clinical characteristics that predict an increased risk of adverse surgical outcomes (e.g., moderate-severe chronic obstructive pulmonary disease, disability from prior stroke, or prior cardiac surgery; STS-predicted risk of mortality >2%) | ||||
| III — For SIHD in patients with unfavorable anatomy for PCI and who are good candidates for CABG | B | |||
| 2021 ACC/AHA54) | IIa — In selected patients with SIHD and significant LMCAD for whom PCI can provide equivalent revascularization to that possible with CABG, PCI is reasonable to improve survival | B | ||
ACC = American College of Cardiology; AHA = American Heart Association; CABG = coronary artery bypass grafting; EACTS = European Association for Cardio-Thoracic Surgery; ESC = European Society of Cardiology; LMCAD = left main coronary artery disease; PCI = percutaneous coronary intervention; SIHD = stable ischemic heart disease; STS = Society of Thoracic Surgeons; SYNTAX = Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery.
![]()
Heart team approach for optimal left main revascularization
Current guidelines recommend multidisciplinary Heart Team decision-making in the management of complex CAD, including LMCAD.52)53) In real-world clinical practice, patients and physicians are increasingly choosing PCI over CABG for LMCAD owing to convenient benefit of less invasiveness and early recovery.2)55) Consequently, increasing clinical and anatomical complexities in patients undergoing left main PCI have been widely reported worldwide.3)56) Therefore, the role of heart team to guide the decision-making on the optimal revascularization strategy in LMCAD is emphasized more than ever.
In the heart team discussion, whether there is true equipoise or any conditions that strongly favor one treatment over the other should be discussed based on collective clinical, anatomical, and procedural factors (Figure 2). With the goal of achieving complete revascularization, the complexity and extent of CAD should be taken into account during the Heart Team discussion.57) To facilitate Heart Team discussion and shared decision-making, anatomical scoring system such as the SYNTAX score and surgical risk scores (e.g., EuroSCORE, STS score, and ACEF score) could be used.1)58) Other aspects, not usually reflected in surgical risk scores (e.g., life expectancy, frailty, anticipated quality of life [QoL] improvement, patient preference, patient-stated life goals, expected DAPT nonadherence, operator skills, and local expertise), should be also considered in the comprehensive, integrated discussion.
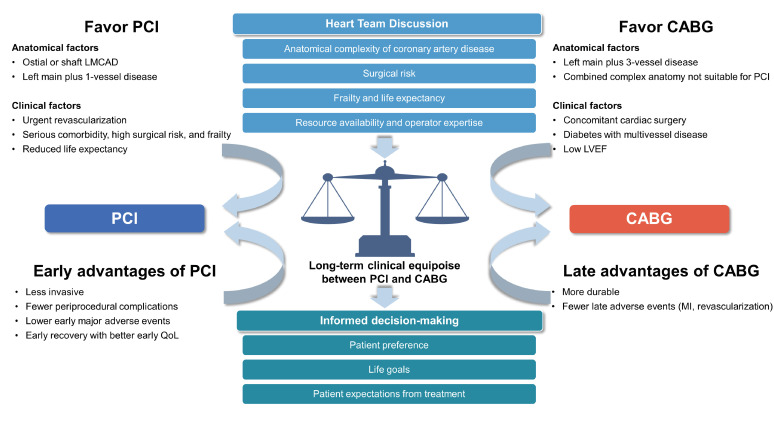
In cases where the Heart Team made the decision of equipoise risk (both PCI and CABG are reasonable), the patient preference should come first. The insignificant difference in long-term mortality and tradeoffs between early and late risk-benefit of the treatment (safety profile, early recovery, and QoL improvement after PCI versus long-term durability after CABG) should inform patients’ own decision-making under the principle of autonomy. In patients who would benefit more from one approach for clinical, anatomical, or other reasons, the Heart Team should discuss the likely differences in future risks and benefits from each treatment with patients to make shared decision-making for the optimal revascularization strategy.
Go to :
SPECIAL ANATOMICAL OR CLINICAL CONSIDERATIONS
Lesion location: ostial/shaft versus distal bifurcation lesions
The lesion location of LMCAD is considered a key factor in determining the optimal revascularization strategy, which was also reflected in previous practice guidelines.52)53) PCI for distal LMCA bifurcation disease is technically demanding and associated with worse outcomes than PCI for ostial/shaft lesions.59) By contrast, PCI showed comparable long-term outcomes with CABG for isolated ostial/shaft LMCAD.60)61) In the 10-year results of the Revascularization for Unprotected Left Main Coronary Artery Stenosis: Comparison of Percutaneous Coronary Angioplasty Versus Surgical Revascularization (MAIN-COMPARE) registry, PCI using DES demonstrated increased mortality and worse serious composite outcomes beyond 5 years compared to CABG in patients with distal LMCA bifurcation disease, particularly when treated with 2-stent techniques.61) In the EXCEL trial, patients with LMCA bifurcation disease but not those with isolated ostial/shaft disease showed a trend toward late crossover in terms of hard endpoints over 3 years.62) Meanwhile, the higher risk of repeat revascularization with PCI than with CABG in distal LMCA bifurcation disease was uniformly reported among several studies. In a recent meta-analysis, the superiority of CABG over PCI was noted in distal LMCAD, but not in ostial/shaft LMCAD.63) Nevertheless, no significant interaction was observed between the relative treatment effect and mortality according to presence or absence of distal LMCA bifurcation involvement in the most recent IPD meta-analysis.50)
Patients with diabetes mellitus
Diabetes is one of the major risk factors for CAD.64) Patients with diabetes are at a higher risk of having a complex CAD such as multivessel or LMCAD.65) Traditionally, CABG has been the preferred treatment in patients with diabetes and multivessel or complex CAD.52)66) However, currently, there is no dedicated RCT comparing the clinical outcomes of PCI with that of CABG for patients with concurrent diabetes and LMCAD. In the 10-year result of the MAIN-COMPARE registry, the risks of mortality and serious composite outcome were comparable following PCI and CABG in patients with diabetes, showing that the benefit of CABG over PCI in patients with diabetes in the BMS era was reduced in the DES era.67) Similarly, the subgroup analysis of the EXCEL trial revealed comparable outcomes between CABG and PCI irrespective of diabetic status.68) In a IPD meta-analysis of 11 RCTs, the diabetic status modified the relative impact of PCI versus CABG on the 5-year mortality in patients with multivessel CAD (p for interaction=0.045) but not in patients with LMCAD (p for interaction=0.13).46) In the latest meta-analysis involving four large RCTs (including EXCEL and NOBLE trials) with at least 5 years of follow-up, diabetic status did not interact with the treatment effect on the 5-year mortality (p for interaction=0.87).50) Therefore, the role of diabetes in guiding the decision-making of left main revascularization strategy is limited in the modern DES era. PCI can be a reasonable option in diabetic patients with LMCAD and relatively low anatomical complexity, whereas CABG should be taken into consideration in diabetic patients with more complex LMCAD.
Patients with heart failure with reduced ejection fraction
CAD is the most common cause of heart failure.69) The long-term manifestation of significant LMCAD could lead to decompensated heart failure due to substantial myocardium at risk.5) Since patients with reduced left ventricular ejection fraction (LVEF) secondary to ischemic CAD have a very poor prognosis with medical therapy alone, an appropriate revascularization strategy could be important to improve their long-term survival. However, no dedicated RCTs have been performed to guide the optimal revascularization strategy for patients with LMCAD and reduced LVEF.
In a 10-year follow-up report of the Surgical Treatment for Ischemic Heart Failure (STICH) trial, CABG showed superior clinical outcomes to medical therapy in patients with ischemic cardiomyopathy.70) However, in the most recent Revascularization for Ischemic Ventricular Dysfunction (REVIVED) trial, PCI in addition to optimal medical therapy did not result in a lower incidence of all-cause death or hospitalization for heart failure.71) This result was consistent in the subgroup of patients with LMCAD (n=95, 13.6% of the study population). In a meta-analysis involving 16,191 patients with CAD and LVEF ≤40% (21 studies, mostly observational studies), CABG was associated with significantly lower mortality than PCI (hazard ratio [HR], 0.82; 95% confidence interval [CI], 0.75–0.90; p<0.001), which was consistent among patients with LMCAD or proximal LAD disease.72) In a recent study from the Interventional Research Incorporation Society-Left MAIN Revascularization (IRIS-MAIN) registry, CABG had a lower risk of the composite outcome of death, MI, or stroke than PCI in patients with LMCAD and moderately or severely reduced LVEF.73) The noteworthy finding of this study was that the differences in clinical outcomes following PCI and CABG were diminished when complete revascularization was attained by PCI in patients with low LVEF.
In the practical viewpoint, the severity of left ventricular dysfunction should be considered along with the potential to achieve complete revascularization in the decision-making on the optimal revascularization strategy in patients with LMCAD and reduced LVEF. If the surgical risk is acceptable, CABG would be more advantageous for patients with moderately or severely reduced LVEF, particularly when complete revascularization cannot be accomplished with PCI.
Elderly patients
Global life expectancy is rising, and the age threshold considered to define the elderly is changing.74) In 2017, South Korea officially became an aged society with >14% of its population aged 65 years and older, and the life expectancy at birth in Korea is expected to be the longest among 35 developed countries in 2030.75)76) Compared to younger patients, older patients usually have more complex CAD and are frequently frailer.77) Thus, treating physicians usually consider age or frailty along with anatomical considerations when determining a treatment strategy in older patients with complex CAD, including LMCAD. However, there is currently no clear guidance for the optimal revascularization strategy in older patients with complex CAD based on available evidence or practical guidelines.
In the analyses of the IRIS-MAIN registry, significant interactions between age and revascularization strategy of PCI and CABG were not found for all-cause mortality, repeat revascularization, and MACCEs.78) A recent subgroup analysis of the SYNTAX Extended study reported that older patients (>70 years) with three-vessel and/or LMCAD had similar 10-year all-cause death, 5-year MACCEs, and 5-year QoL irrespective of revascularization strategy.79) Moreover, no significant difference was found in the treatment effects for clinical outcomes according to age groups in the EXCEL and NOBLE trials and subsequent recent IPD meta-analysis.35)37)50)
Based on currently available evidence, opting for a more invasive surgical revascularization in older patients with LMCAD might be less attractive. Given that long-term survival and QoL are comparable between CABG and PCI, a less invasive approach with PCI may be preferred over CABG in older patients. However, the final decision should be made through shared decision-making in the heart team discussion, considering comorbidities, frailty, and expected QoL, rather than chronological age.
Go to :
STATE-OF-THE-ART LEFT MAIN PERCUTANEOUS CORONARY INTERVENTION
Intracoronary physiology and imaging concept is a key component of the contemporary “State-of-the-Art PCI,” which is uniformly applied in LMCA PCI.
Intracoronary physiology
In the recent analysis of the ISCHEMIA trial, moderate or severe ischemia documented on noninvasive functional testing modalities was weakly predictive of the presence of LMCAD (≥50% stenosis of the LMCA) on coronary computed tomography angiography.80) Although anatomical imaging is important to rule out LMCAD, anatomical assessment of the LMCA lesion is often hampered by the absence of a reference segment, eccentricity, angulation, foreshortening, and overlapping branches, resulting in the interobserver variation and visual–functional mismatch.81)82)83)84) Thus, the functional significance of these lesions should be properly evaluated in patients with intermediate LMCA stenosis and no clinically relevant symptoms or findings suggestive of ischemia. With the physiological assessment of the fractional flow reserve (FFR), revascularization of LMCA lesions can be safely deferred with FFR values of >0.75 or 0.80.82)85)86)87)
Meanwhile, FFR measurement in the jailed left circumflex artery (LCX) during the left main provisional stenting procedure can help guide the adequate treatment strategy. According to previous studies, angiography alone tends to overestimate the functional significance of side branches after bifurcation crossover stenting.88)89) In a recent observational study from Korea, the long-term impact of the FFR value in jailed LCX after simple crossover stenting for LMCAD was evaluated.90) In this report, the patients with FFR ≥0.80 in jailed LCX had a lower 5-year target lesion failure rate than those with FFR <0.80, while no difference in such outcomes was found based on angiographic diameter stenosis. According to this study, unnecessary complex procedures can be avoided by FFR measurement in the jailed LCX.
In addition, the use of physiology-guided PCI in patients with LMCAD and concomitant multivessel disease could result in lower MACCE risk associated with non-left main PCI. The FAME trial showed that FFR-guided PCI for multivessel CAD significantly reduced the risk of the composite of death or MI compared with angiography-guided PCI.91)
The instantaneous wave-free ratio (iFR), a resting index, was introduced recently and showed noninferiority to FFR in guiding revascularization.92)93)94) Despite compelling clinical evidence suggesting that deferring the revascularization of non-LMCA CAD with an iFR >0.89 is safe, supporting data on its use for LMCAD has been limited. In 2020, the results of the DEFINE-Left Main Registry reported that deferral of revascularization for LMCAD with iFR cutoff >0.89 appears to be safe, with similar long-term outcomes over a median follow-up of 30 months.95) Based on a recent study, FFR and iFR showed moderate agreement in patients with intermediate LMCAD, and deferred left main revascularization based on the iFR appeared safe.96) If more evidence can be accumulated, iFR may become a valuable tool as an adenosine-free alternative to the FFR in the evaluation of LMCAD.
Intravascular ultrasound
Intravascular ultrasound (IVUS) is the most well-established intravascular imaging method in the evaluation of LMCAD. IVUS use in LMCAD provides information on the vessel size, minimal lumen area (MLA), and extent and distribution of the plaque within the LMCA and its branches of the LAD and LCX.97)
IVUS can be useful for determining the functional significance of intermediate LMCAD. The IVUS-derived MLA can reflect the ischemic burden of the LMCA lesion, serving as an independent predictor of future cardiac events.98) A previous US study first proposed an MLA cutoff value of 5.9 mm2 for an FFR value of <0.75 (sensitivity 93%, specificity 94%).99) Later, an MLA of ≥6 mm2 on IVUS was validated as a safe cutoff value for deferring revascularization for intermediate LMCAD in a multicenter prospective study.100) However, a study involving Korean individuals reported that IVUS-derived MLA of ≤4.5 mm2 is related to functionally significant LMCA stenosis (FFR <0.80).101) One of the plausible explanations for these discrepancies might be ethnic differences in the diameters of coronary arteries.1) Despite some controversies, currently, an MLA of ≥6 mm2 is a widely acknowledged cutoff value for safely deferring revascularization of LMCAD.
IVUS can help in planning the PCI strategy, especially in distal LMCA bifurcation disease, by characterizing the bifurcation anatomy and longitudinal distribution of the plaque. As a part of planning, the risk of side branch compromise, stent length and diameter, and reference size and length (to plan proximal optimization technique) measurements can be evaluated during IVUS. To obtain comprehensive information on left main bifurcation anatomy and prevent overestimating the ostial LCX MLA due to the noncoaxial position of the IVUS catheter, IVUS imaging should be performed from both the LAD and LCX with at least one pullback to the aorta. Another important role of IVUS in the left main PCI is to ensure stent optimization. Based on an early study, stent underexpansion, as represented by the minimum stent area (MSA) on IVUS measurement, was a key predictor of restenosis following PCI.102) Even in a more recent analysis from the EXCEL trial, IVUS-derived MSA was strongly associated with the occurrence of adverse events during a 3-year follow-up after PCI with contemporary DES.103) The use of IVUS during left main PCI has a prognostic impact, especially in patients with distal left main bifurcation disease treated with two-stent technique, because the IVUS guidance could facilitate stent optimization strategy to achieve optimal stent expansion following complex stenting.104)105) While RCTs are limited, the use of IVUS guidance during left main PCI impressively reduced the risk of all-cause mortality by 40% and cardiac death by 53% compared to angiography-guided PCI in a meta-analysis (based mostly on nonrandomized studies).106) Several RCTs (i.e., OPTIMAL [NCT04111770], INFINITE [NCT04072003], and DKCRUSH VIII [NCT03770650]) to evaluate the true prognostic impact of IVUS-guided PCI are currently ongoing. The currently best-known MSA criteria for predicting restenosis are 5.0 mm2 for the LCX ostium, 6.3 mm2 for the LAD ostium, 7.2 mm2 for the polygon of confluence, and 8.2 mm2 for the proximal LMCA above the polygon of confluence (“5-6-7-8” rule).107) However, stricter IVUS-derived criteria to define optimal bifurcation stenting (MSA >10 mm2 for LMCA, >7 mm2 for LAD, and >6 mm2 for LCX) are advocated by some clinicians, as in the ongoing DKCRUSH VIII trial.108) In summary, IVUS is an important component of contemporary left main PCI and useful at each step of left main PCI, leading to a better prognosis in patients with LMCAD.
Go to :
FUTURE PERSPECTIVES
For optimal management and decision-making for LMCA revascularization, several unmet issues should be further addressed in the future studies. Since CABG provides clinical benefits at longer follow-up after overcoming the intrinsic early risk with surgery, sufficient longer follow-up is important when comparing PCI with CABG. The relative treatment effects of PCI using contemporary DES in comparison with CABG beyond 5 years—including late catch-up or divergence in the clinical event rate noted in 5-year follow-up results of EXCEL and NOBLE trials—should be further clarified by longer follow-up results from these trials.
A closer look at the controversies surrounding EXCEL and NOBLE trials could help in understanding the perspectives of interventionists and surgeons on contemporary PCI and CABG and designing future revascularization trials. Owing to the conflicting primary results and subsequent uncertainties that mainly resulted from differences in definitions, one of the key issues in future studies comparing PCI with CABG would be the validation and acceptance of a harmonized definition of clinical outcomes, including procedural MI.
Regarding the technical aspect of the left main PCI, the provisional approach as the default strategy for complex distal bifurcation PCI was recently challenged by double-kissing crush technique, which showed better clinical outcomes than provisional stenting.109)110) Although the technical and procedural refinements of the PCI technique are still in progress, further solid evidence (including the definition of complex LMCA bifurcation lesion requiring the upfront two-stenting and optimal two-stent strategy for best clinical outcomes) is needed to appropriately guide LMCA bifurcation PCI strategies. Meanwhile, the optimal antithrombotic strategy following left main bifurcation PCI with the 2-stent technique is still not clear. Left main bifurcation PCI is conventionally one of the most complex procedures; however, sophisticated stent technology, refinement in the bifurcation PCI technique, and widespread adoption of IVUS have dramatically helped mitigate restenosis and thrombosis following PCI. In addition, traditional DAPT strategies are now being challenged by shortened DAPT strategies or more tailored antithrombotic strategies.111) Finally, the results of highly selected clinical trials may not be fully applicable to a variety of real-world patients with increasing clinical and anatomical complexities.
The role of the unbiased heart team is fundamental in the selection of the optimal revascularization strategy. Appropriate selection of revascularization strategy for each patient is more important than the binary comparison of PCI with CABG in RCTs to maximize clinical outcomes. Although the patient is the center of the Heart Team and the health goals for most patients are “Live Longer. Live Better.”, the latter is often not taken into account in decision-making. Consideration of the qualitative aspects (e.g., QoL, life goals, and patient preferences) may become more important because no significant differences were found in the long-term major clinical outcomes after PCI and CABG based on the most up-to-date evidence.
Go to :
CONCLUSIONS
For myocardial revascularization in patients with complex CAD including LMCAD, PCI and CABG are very different procedures with varying early and late risks and benefits. The landscape of LMCAD revascularization is constantly changing along with the evolving CABG and PCI practices. Over last decades, tremendous advancements in the PCI field have resulted in improved clinical outcomes after left main PCI; thus, PCI is now considered a reasonable treatment option for a substantial proportion of patients with LMCAD. In contemporary clinical practice, we encounter the diverse spectrum of patients with LMCAD with various clinical and anatomical complexities. Owing to the gap between clinical practice and the available supporting evidence, no unified algorithm can be applied to various clinical scenarios in left main revascularization. Decision-making should be on a case-by-case basis; therefore, the Heart Team approach is being emphasized more than ever to deliver the best care to patients with LMCAD.
Go to :
 XML Download
XML Download