

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ventricular septal defect (VSD) is the most common form of congenital heart disease.1) There are various types of VSD based on the location of the defect within the ventricular septum. The most common type is perimembranous VSD, with various extensions to the outlet septum or to the muscular septum. The perimembranous defect in patients with this type of VSD is usually located close to the aortic and tricuspid valves. In contrast, subpulmonary or subarterial defects are located just below the pulmonary and aortic valves. The subarterial type of VSD is rare worldwide but encountered more frequently in Asian countries than in Western countries. The defect can also be located entirely within the muscular portion of the interventricular septum (muscular type) or located just below the tricuspid valve and in the right ventricle septal leaflet (inlet type).
Since the first surgical repair of VSD in 1954 by Lillehei et al.,2) surgery has been the gold-standard method for VSD repair. Although the surgical outcomes have been improved consistently, surgery is associated with morbidity and mortality, including atrioventricular block, residual leak, and neurologic complications.3)4)5)6)7)8) To reduce the morbidity, mortality, and psychological stress, percutaneous transcatheter VSD closure has emerged, with the first report published by Lock et al. in 1988.9) Following the first success, several cases describing successful closure with various devices, such as the Rashkind device, vascular coils, button device, and Starflex device, were published.10)11)12)13)14) Meanwhile, the Amplatzer family of cardiac occlusion devices (Abbott, Chicago, IL, USA) has made actual progress in this field.15) Recently, a meta-analysis on percutaneous closure of all types of VSD using different types of devices reported a success rate of 96.6% with rare mortality and mentioned significant complications, including residual shunt, valvar problems, and cardiac arrhythmias.16) The recent development of lower-profile delivery systems and softer devices has improved success rates and lowered incidence rates of heart block and arrhythmias. However, there remains a substantial degree of uncertainty associated with device closure. Nonetheless, I am looking forward to device closure becoming a standard treatment for VSD as if percutaneous pulmonary valve insertion and device closure of foramen ovale have been established as a standard therapy in the field of catheter intervention for congenital heart disease.17)18)
In this review, the technical and material aspects of percutaneous VSD closure are described and complications associated with device closure are explained. The patient’s informed consent has been waived by Institutional Review Board approval (2022-11-118).
Go to : 
INDICATIONS FOR VSD CLOSURE
In general, the defect should be closed whenever the patient is symptomatic due to hemodynamic consequences. As a rule, VSDs resulting in a Qp/Qs of >1.5 and volume overload in the left ventricle have been accepted as needing to be closed. However, irreversible pulmonary hypertension due to longstanding VSD is a typical contraindication of closure. There are several complications that occur in patients with even small VSDs and are indications for surgical closure; they include left or right ventricular outflow tract stenosis and aortic valve cusp prolapse. A history of infective endocarditis is another indication, too. Transcatheter VSD closure is reserved for membranous or muscular defects, although there are reports of successful transcatheter closure of subarterial VSDs.19)20)21) For safe VSD closure using devices, adequate distance (≥2 mm) from the aortic valves ought to be secured.22) Patients with other anatomic lesions that need correction together with the VSD should undergo surgery instead of transcatheter closure. When it comes to small, restrictive VSDs, significantly improved surgical outcomes of VSD closure might allow us to expand the indications for VSD closure.23) Neumayer et al. argued in their paper that surgical closure of small perimembranous VSD in childhood would be recommendable due to various complications that occur in adult life.24) Therefore, using various kinds of devices and improving technology might help close small VSDs percutaneously.25) Transcatheter VSD closure is not usually safe in small children weighing <10 kg, but some authors have reported successful transcatheter VSD closure in these small children.26)27)28)29)30) However, we should remember that young age and low weight may be risk factors for procedure failure and complications.31)32)
Go to :
PROCEDURES
The procedures of VSD closure have been well described. The choice of procedure depends on the patient’s size, the defect’s size and location, and the device being used. An antegrade approach has been accepted as a standard method so far, which relies on an arteriovenous wire loop and involves device delivery from a venous approach, i.e., a femoral or internal jugular vein. The internal jugular vein approach might be helpful for treating muscular VSDs located more toward the apex area. The retrograde approach from the femoral artery can be conveniently used to treat small VSDs without using a wire loop by the introduction of symmetric devices with low profiles (Figure 1).33)34) Otherwise, a perventricular approach can be used in small patients.

Before the procedure, 100 IU/kg of heparin as a bolus intravenous injection and continuous infusion are mandatory. The VSD can be crossed from the left ventricle usually using a right coronary diagnostic catheter and hydrophilic J-tipped guidewire. An arteriovenous wire loop should be created after snaring the wire in the pulmonary artery or superior/inferior vena cava using an antegrade approach. The most important task in creating an arteriovenous wire loop is to avoid entanglement with the tricuspid valve chordae (Figure 2). However, when the operator snares the wire in superior or inferior vena cava, they do not need to worry about entangling the chordae. At this point, the delivery sheath can be advanced over the wire from the vein into the ascending aorta; then, the device is often deployed partially in the ascending aorta. Lastly, the device can be deployed completely and released under echocardiographic guidance. When using the retrograde approach, the delivery catheter is advanced to the right ventricle from the femoral artery over the wire, not creating an arteriovenous wire loop. The device is then deployed partially in right ventricle before complete deployment across the VSD. Use of the perventricular hybrid approach is saved for small children with large muscular VSDs. A right ventricle free wall puncture after full or partial sternotomy is performed directly under transesophageal or epicardial echocardiographic guidance and a wire can then be advanced into the left ventricle across the VSD. Following an exchange of a sheath of appropriate size for the device, successful device implantation can be achieved under echocardiographic guidance. Lastly, the puncture site and sternotomy should be closed by the surgeon (Figures 3 and 4). After the procedure, an intravenous heparin infusion should be maintained for 24 hours; then, aspirin should be taken orally for 6 months.

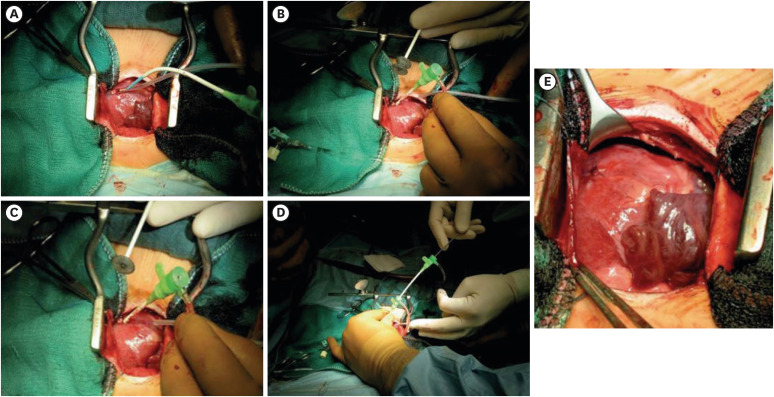 | Figure 3Perventricular closure of muscular VSD. A direct puncture of the right ventricle free wall (A) and sheath insertion over the defect (B) are followed by device preparation (C) and implantation (D). After the implantation, the puncture site should be sutured (E).VSD = ventricular septal defect.
|
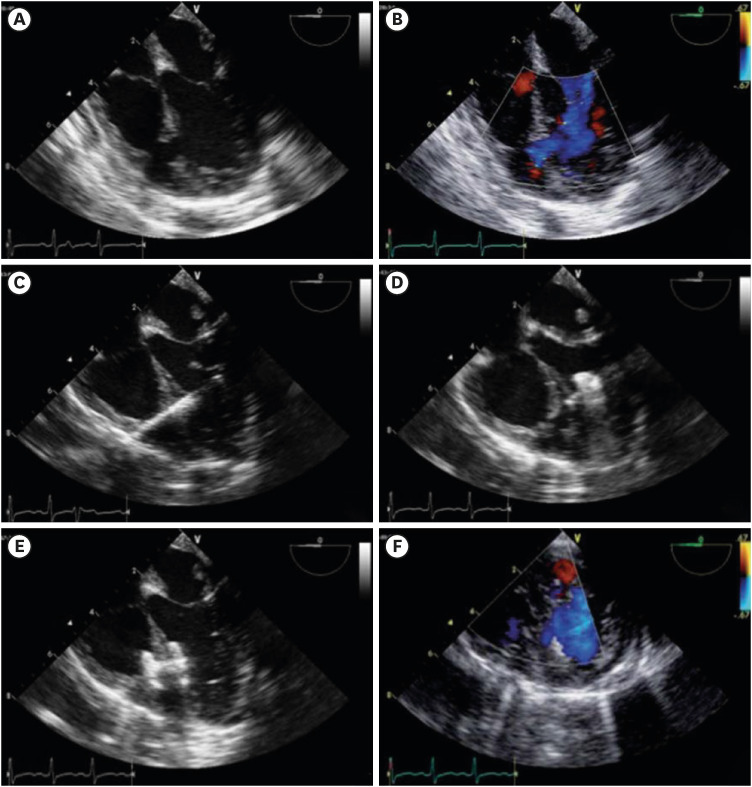 | Figure 4Trans-esophageal echocardiography guidance for perventricular closure of muscular VSD. Conformation of the defect and puncture site (A, B) leads to the puncture needle passing through the defect (C) and device deployment partially inside the left ventricle (D). Echocardiography confirms a secure position of the device (E) and complete defect closure (F).VSD = ventricular septal defect.
|
Go to :
MUSCULAR VSD CLOSURE
Surgical closure of muscular VSD remains challenging and is associated with increased complication and mortality rates compared to other types of VSD.35)36)37) Following the introduction of the Amplatzer device, a number of reports of successful device closures of muscular VSD have been published so far,32)38)39)40)41)42)43)44) with an overall procedural success rate of 87–100%. However, various complications associated with the procedure were also reported, such as device embolization, cardiac perforation, stroke, and death. The most frequent complication might be the presence of a residual shunt through the existing defect or a new defect.44)45) However, the existence of a residual shunt immediately after closure might also occur after the surgical procedure. Fortunately, it is known that most of the residual shunt will close within 1 year after the procedure either spontaneously or as triggered by devices.44) Some authors have reported series of small patients, including neonates and infants, with good success rates, but they also documented high complication rates.42)43)44) In the small infant, especially those weighing <5–6 kg, using the perventricular approach only under transesophageal echocardiography guidance was suggested by Amin et al.46) in 1998. Further studies have reported its safety and efficacy with much-reduced complication rates.28)47)48)49)50) In particular, Kang et al.30) confirmed the long-term safety of this technique for small infants. The Amplatzer muscular VSD device or other similar devices used son-label have been employed as the major devices for muscular VSD, but other good experiences with the Amplatzer duct occluder (ADO) and the KONAR-Multifunctional™ ventricular septal defect occluder (Lifetech, Shenzhen, China) have also been reported.29)51)
In most cases, the antegrade approach has been used, but the retrograde approach could be effective for treating high muscular VSD. A device size that is 2–3 mm larger than the largest end-diastolic diameter should be selected because most defects are oval in shape. In most cases, the first retention disc of the device can be completed in the left ventricle (antegrade approach) or right ventricle (retrograde approach), with operators remaining cautious about entanglement of the chordae inside each ventricle. Especially, when taking the perventricular approach in small infants, special attention must be paid to ensure entanglement with the mitral valve apparatus is avoided. To prevent left ventricular posterior wall trauma, proper space inside the left ventricle should be secured. When closing apical muscular VSDs, it is difficult to gain enough space inside the right ventricle for deployment of the right-side disc. The puncture site should be selected after taking both the right and left discs into account. For this reason, the ADO might be a good choice.
Surgical closure of multiple muscular VSDs has been known to be challenging, especially when they are located at the apex muscular area. Historically, Kirklin et al.52) reported a hospital mortality rate of 14% and a need for reoperation to close residual defects in 28% of patients. As a result, various techniques were developed by various surgeons. Still, surgical repair of multiple muscular VSDs is challenging, and transcatheter closure might be an additional good option. Multiple defects can be closed with multiple devices using standard techniques. Zartner et al. reported their experience employing multiple devices in a single procedure but noted ≥1 procedure may be required.43)
Go to :
PERIMEMBRANOUS VSD CLOSURE
Percutaneous closure of perimembranous VSDs is more challenging and controversial still. The Amplatzer membranous VSD occluder was developed and began trials in the United States (Figure 5). In a U.S. phase 1 trial and subsequent similar trials, the device attained high procedural success rates but led to rare cases of complete heart block.53)54)55) Moreover, additional studies following the initial reports demonstrated higher rates of complete heart block (2–22%).56)57)58)59) Ultimately, the Amplatzer membranous VSD occluder was not approved for clinical use. To date, there have been several trials using different types of Amplatzer occluders with satisfactory results and only very rare cases of complete heart block (Figure 6).34)60)61)62)63)64)65) Meanwhile, a new Amplatzer device replacing the Amplatzer membranous VSD occluder was developed and tested experimentally in some cases (Figure 7).66)67) In a prospective study, it led to a good success rate of 95% and no complete atrioventricular block (CAVB) or significant aortic valve regurgitation.68)
 | Figure 5The asymmetric shape of the Amplatzer membranous VSD occluder (A), which is designed to sit across the defect without distorting the aortic valve. A left ventricular angiogram demonstrates complete closure of the defect (B), and a lack of aortic valve impingement is confirmed by an aortic angiogram (C). A radiopaque marker on the left ventricular disk helped to confirm appropriate device positioning (courtesy of Abbott, Inc., Chicago, IL, USA).Figure is adapted from Bass et al.55) with permission.
VSD = ventricular septal defect.
|
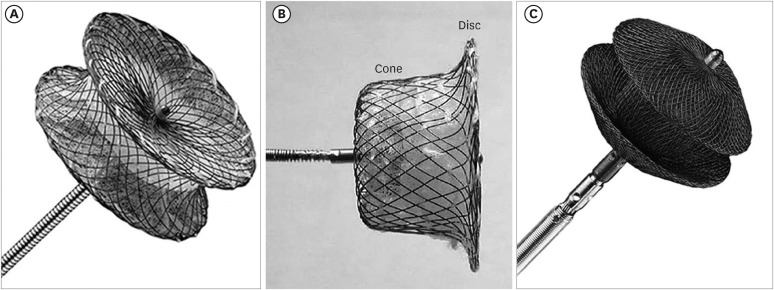 | Figure 6Amplatzer devices for VSD closure. The Amplatzer muscular VSD occluder (A), ADO type I (B), and ADO type II (C).ADO = Amplatzer duct occluder; VSD = ventricular septal defect.
|
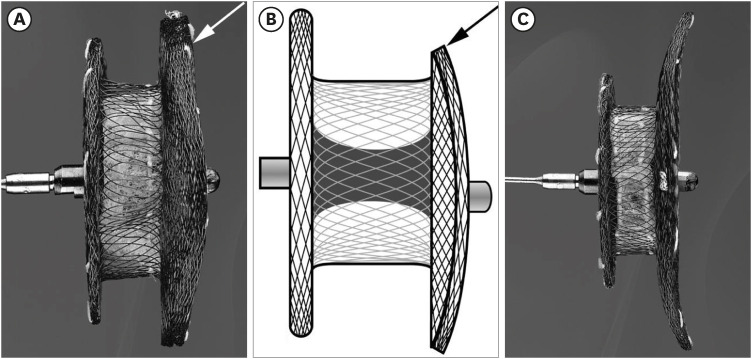 | Figure 7New Amplatzer perimembranous VSD occluders include a symmetrical type (A) and an asymmetrical type (B). The white arrow (A) indicates the 3-mm superior rim of the symmetrical device. The black arrow (B) indicates the 1-mm superior rim of the asymmetrical device. The curvature of the left side wing can match the left ventricle outflow tract.VSD = ventricular septal defect.
|
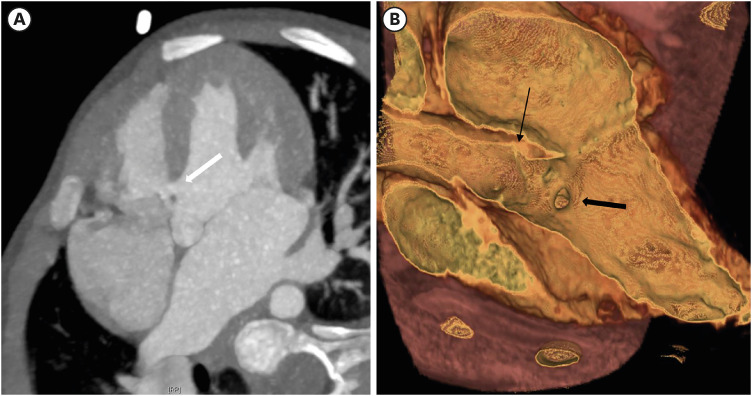
The size and morphology of VSDs vary, so it is not easy to determine the VSD size precisely. Most VSDs have an oval shape, and the longest diameter at the time of the largest size should be measured. Collecting en-face images using electrocardiogram gated cardiac computed tomography might be very helpful (Figure 8), but could be difficult when the defect is associated with aneurysm formation. The morphologies of aneurysm are not uniform and >1 exit holes on the right side may exist.69) Defining an exit hole on the right side can be hard. Sometimes, other holes appear after device closure. Anyhow, whether to close either one or multiple exit holes on the right side or one exit hole on the left side must be determined because most perimembranous VSD patients with aneurysms only have a single hole on the left side. The closure of a right-sided exit hole might be safer in terms of CAVB and aortic valve damage associated with device placement due to the existence of the left disc left inside the aneurysm (Figure 9). However, multiple exit holes on the right side may be closed using multiple devices. The most complex aneurysm morphology is a cauliflower appearance, with multiple fenestrations, and closure of the single exit hole on the left side might be preferred in this context. Therefore, there are no solid guidelines for the closure of perimembranous VSD in patients with aneurysm formation.

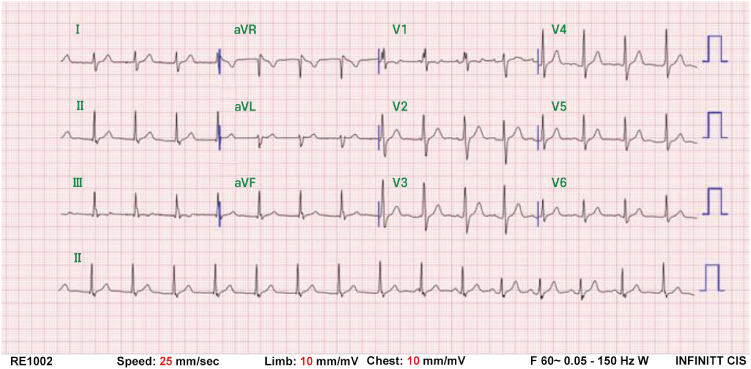
Closure is usually completed using an antegrade approach with transesophageal or transthoracic echocardiographic guidance. Due to conduction pathway proximity, transient arrhythmias during the procedure are common, and cautious manipulation of the wire and catheter is necessary. The most important complications are arrhythmias and CAVB, which require pacemaker insertion. With the newly developed soft devices for perimembranous VSD closure, an incidence of 0.2% was reported, which is decreased significantly from historical figures and more similar to that recorded after surgery.70)71) The exact mechanisms for CAVB have not been discovered yet, but the exertion of radial and clamp forces from the device causing injury or inflammation in the surrounding conduction tissue was proposed. In the case of postprocedural arrhythmias, steroid use has been reported to be effective even in patients with CAVB.72)73)74)75) Not only just after the procedure but also months to years following implantation, CAVB may occur.56)76)77) The risk factors for CAVB are uncertain, but smaller patient sizes and oversized devices have been suggested.56) Another study suggested a farther distance from the aortic valve and closer distance to the tricuspid valve as risk factors.76) For various reasons, oversized devices should not be used, and only those 1–2 mm larger than the defect diameter have been recommended. In order to reduce radial and clamp forces, dual-disc devices with long distances between the retention discs and softer devices have been preferred over the Amplatzer membranous VSD occluder. Several such devices made in China have emerged, and their effective and safe outcomes in human trials have been reported.78)79)80)81) Recently, another type of device, The KONAR-Multifunctional™ occluder, was developed, and its outcomes were reported.82)83)84) The study investigators reported no complete heart block among mid-term outcomes, but Leong et al. observed CAVB after KONAR-Multifunctional™ occluder implantation.77) Among the different kinds of devices used in perimembranous VSD closure, in the ADO type II and the Amplatzer vascular plug type II lack data on CAVB cases. However, considering the potential occurrence of CAVB even in the late postoperative period, transcatheter closure of perimembranous VSD is not absolutely without a risk for CAVB. Other than CAVB, we experienced several patients with accelerated idio-junctional rhythms appearing 1–9 days after their procedure (Figure 10). Zhao et al.85) reported that such idio-junctional rhythms are transient and benign, and there were no patients with long-term problems in our series.
The presence of a residual shunt after device closure of perimembranous VSD could be defined by the width of the color Doppler jet around the device. Shunts of more than a moderate size (>2 mm) with an audible murmur should be revised using larger devices or surgical referral. In general, complete closure rates have been known to reach >90% during follow-up, and the need for surgical correction due to the presence of a residual shunt has been rare.33)56)57)63)86) Hemolysis after the procedure is associated with the existence of a residual shunt, even in cases of only small residual shunts. From a recent report, the incidence of post-procedural hemolysis was 1.6%, with no significant hemolysis necessitating device retrieval; in all cases, complete resolution with hydration and alkalization was reported.87)
Device impingement of the aortic valve cusp should be avoided because it can cause aortic regurgitation, resulting in the need for device removal. Careful evaluation of the distance between the defect and aortic valve is crucial, but it is not easy to complete on echocardiographic images, especially in the case of perimembranous VSD. In general, a distance of >2 mm is acceptable but depends on the device type and expected device position. For example, device placement inside an aneurysm can be very safe regardless of the distance from the aortic valve, but ADO II requires a greater distance. With improved designs of current devices for perimembranous VSD and careful monitoring before and after the procedure, very low rates of significant aortic regurgitation following device closure (<0.5%) were reported.70)71) Other than the aortic valve, the tricuspid valve should also be monitored during and after the procedure. The right disc of the device can interfere with septal leaflet motion, which results in tricuspid regurgitation. As such, a softer device with greater space between the right and left discs is preferred over a device with less space and a rigid right disc, such as the Amplatzer membranous device. In spite of those concerns, Saurav et al.88) found that percutaneous closure of perimembranous VSD led to a similar success rate as that of surgical closure without an increased risk of serious complications. Actually, various articles on percutaneous closure of perimembranous VSD have reported very good success rates and rare complications that did not require intervention or operation. When we investigated 64 cases recently treated using Cocoon occluders (Vascular Innovations Co., Nonthaburi, Thailand) and ADO II over 6 years, one case was referred to surgery due to having too large a defect, but no death or CAVB case was documented. Newly developed minimal aortic regurgitation in one case and small residual leaks in 2 cases were noticed, but no further intervention was needed, similarly to in other reports (Table 1).

Table 1
Outcomes of percutaneous closure of perimembranous VSD using various kinds of devices
| Study | Devices | No of patients | Success rate (%) | Age range (years) | Defect range (mm) | Death (%) | AR* (%) | CAVB (%) | Residual shunt* (%) |
|---|---|---|---|---|---|---|---|---|---|
| Zhao et al.60) | ADO II | 51 | 98.0 | 1.5–25.0 | 1.8–5.1 | 0 | 7.8 | 0 | 0 |
| Hua et al.89) | AVP II | 16 | 100 | 0.5–27.3 | 5.9–14.4 | 0 | 12.5 | 0 | 17.0 |
| Jiang et al.65) | ADO II | 103 | 99.0 | 2.0–3.9 | 0 | 1.0 | 0 | 10.8 | |
| Lin et al.90) | ADO | 105 | 95.2 | 6.3–28.5 | 3.2–5.1 | 0 | 1.0 | 0 | 4.5 |
| Lee et al.62) | ADO I | 21 | 100 | 3.0–42.0 | 2.5–5.6 | 0 | 0 | 0 | 9.5 |
| Haddad et al.82) | MFO | 20 | 100 | 0.7–43.4 | 7.0–16.5 | 0 | 5.3 | 0 | 17.8 |
| Current study | Cocoon VSD occluder + ADO II | 64 | 98.4 | 2.3–57.0 | 0 | 1.6 | 0 | 3.1 |
ADO = Amplatzer duct occluder; AR = aortic regurgitation; CAVB = complete atrioventricular block; MFO = multifunctional occluder; VSD = ventricular septal defect.
*Complications happened, but no interventions were needed.
![]()
Go to :
POSTOPERATIVE RESIDUAL VSD CLOSURE
The main reason for postoperative residual VSD is dehiscence of the patch,7) although iatrogenic fenestration might be another cause. Redo surgery for residual VSDs is risky, carrying increased mortality or morbidity rates, so transcatheter closure could be another good option. A few reports documenting complete closure and no complications have been published.91)92)93) Their authors demonstrated that the procedures were straightforward and the postprocedural courses were very smooth. Therefore, transcatheter device closure of postoperative VSD is safe and effective and can be performed using various types of devices.
Go to :
DEVICES OTHER THAN AMPLATZER DEVICES
Some of those devices are shown on Figure 11. The Nit-Occlud® Lê VSD coil (Produkte für die Medizin AG, Cologne, Germany) (Figure 11B) has been used for perimembranous and membranous VSD closure with good results.94) VSD closure using the Occlutech duct occluder (Occlutech GmbH, Helsingborg, Sweden) was also reported.95) There are several kinds of Chinese VSD closure products, and a prospective study from Brazil using CERA® devices (Lifetech, Shenzhen, China) in perimembranous VSD closure reported a complete closure rate of 91%.81) This author documented experiences of VSD closure using Cocoon occluders (Figure 11A).96) Recently, the KONAR-Multifunctional™ occlude (Figure 11C) has been receiving attention in East Asia. Unfortunately, ideal devices for all kinds of VSD have not yet been developed.

Go to :
CONCLUSION
Although surgical VSD closure is a golden standard, transcatheter VSD closure has emerged as an alternative option. Because surgical outcomes after muscular VSD closure are unsatisfactory, device closure has been introduced and has shown good results. Surgical morbidity led to the introduction of device closure for perimembranous VSD. Even though CAVB was the challenging problem in the beginning, the development of low-profile systems and softer devices could reduce its rate to one lower than that seen after surgery. However, serious conduction problems and proximity to the aortic valve remain to be addressed, and performing the procedure in small patients is challenging. Overall, transcatheter VSD closure is a promising treatment modality and an alternative emerging novel option to surgery.
Go to :
 XML Download
XML Download