

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epidermoid cysts are uncommon tumors, accounting for less than 2% of intracranial tumors [1]. These tumors originate from the remaining ectodermal tissues when the neural tube is closed at the third to fifth gestational weeks [2]. According to their location, epidermoid cysts are classified as extradural and intradural [1]. As one of the extradural types, intradiploic epidermoid cysts occur in any part of the skull and are even rarer tumors [3]. They usually present as a painless local swelling under the scalp. Rarely, they show dural invasion and compress the brain parenchyma [14]. Here, we present a rare case of a giant intradiploic epidermoid cyst of the skull presenting with progressive headache.
Go to : 
CASE REPORT
A 57-year-old woman presented with a 1-year history of localized headache in the occipital area. The symptoms were aggravated 2 weeks prior to arrival at our institution. Physical and neurological examination revealed no specific findings. CT and MRI showed an extradural mass measuring 50×70 mm in the occipital bone (Fig. 1). CT scanning showed a large extracerebellar, hypodense lesion representing destruction in the right occipital bone. MRI revealed compression in the right occipital lobe and cerebellar hemisphere. T2-weighted MRI showed hyperintensity with a low intratumoral signal, and T1-weighted MRI showed hypointensity with a high intratumoral signal. Diffusion-weighted imaging (DWI) MRI showed restricted diffusion with characteristic hyperintensity. T1-weighed gadolinium-enhanced MR image showed no enhancement of the mass. Based on the radiological findings including the extradural location, bony erosion, diffusion restriction and lack of contrast enhancement, an extradural intradiploic epidermoid cyst was considered.
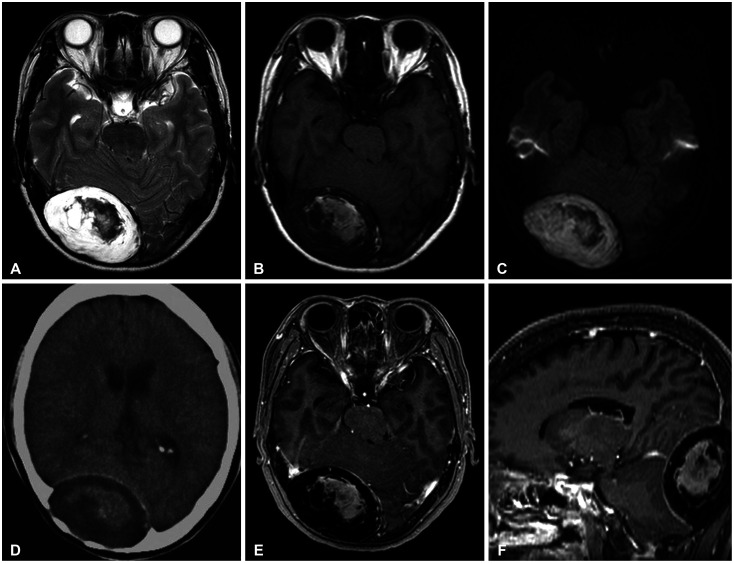 | Fig. 1CT and MRI shows an extradural mass measuring 50×70 mm in the occipital bone. MRI also reveals compression in the right occipital lobe and cerebellar hemisphere. A: T2-weighted MRI shows hyperintensity with a low intratumoral signal. B: T1-weighted MRI shows hypointensity with a high intratumoral signal. C: Diffusion-weighted imaging shows restricted diffusion with characteristic hyperintensity. D: CT scanning shows a large hypodense mass with sharply demarcated bony defects in the right occipital bone. E and F: T1-weighted contrast MRI shows no enhancement of the mass. There is no abnormal signal change in the brain.
|
A paramedian suboccipital approach was planned. The tumor and its capsule were completely removed in an en bloc removal pattern (Fig. 2A). There was no dura defect and no extension to the intradural space. After gross total tumor removal, cranioplasty was performed using bone cement. The pathology report confirmed that the tumor was an epidermoid cyst. The cyst was unilocular and consisted of a grayish brown, sticky material. The wall of the cyst was gray-white and smooth (Fig. 2A, B). The mass was lined by mature squamous epithelium and filled with laminated keratin material (arrow and arrowhead, respectively, Fig. 2C).
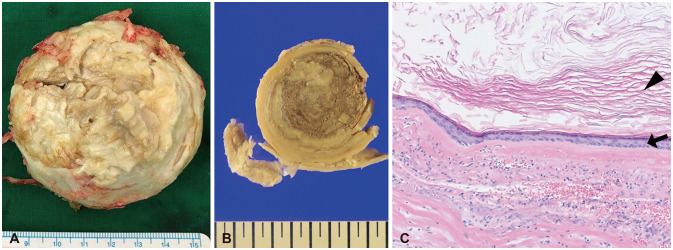 | Fig. 2The cyst is unilocular and consisted of a grayish brown, sticky material. A and B: The cyst wall is gray-white and smooth. C: Histologic examination shows that the cyst is lined by mature squamous epithelium (arrow) and filled with anucleate laminated keratin material (arrowhead) (hematoxylin-eosin stain, ×100).
|
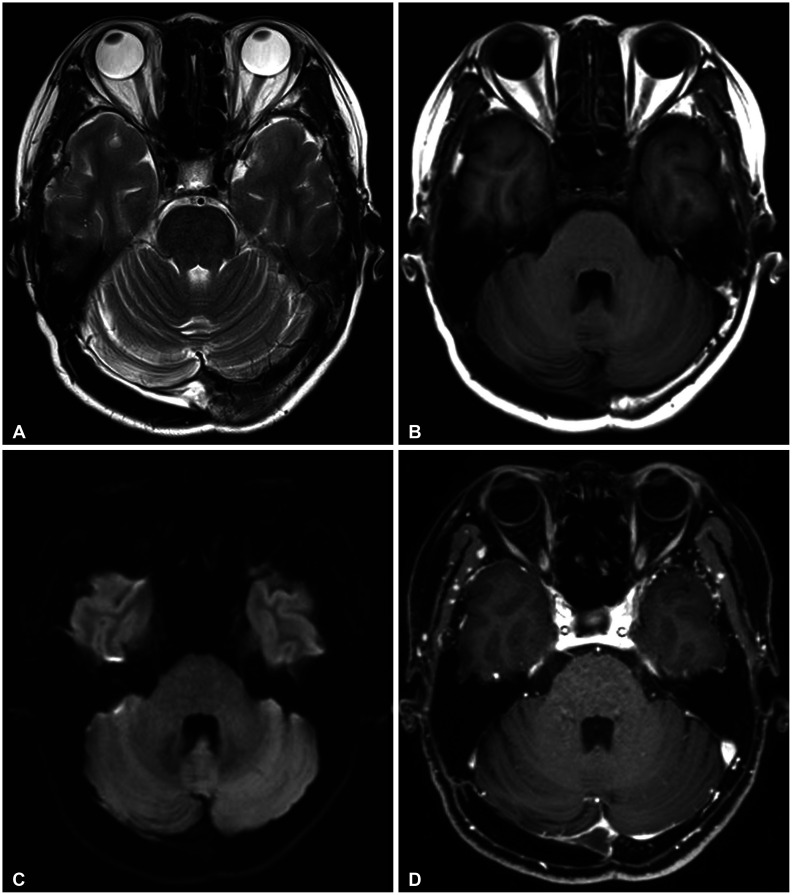
Follow-up MRI 24 months after the operation showed no recurrence (Fig. 3). At the last clinical follow-up 24 months after the operation, the headache was well controlled without any medications.
This study was approved by our Institutional Review Board and followed the Declaration of Helsinki (IRB No. 2020-03-033-001). Identifying details (names, dates of birth and other information) were not included in this study. Informed consents were received from the patient.
Go to :
DISCUSSION
Epidermoid cysts are slow-growing benign congenital lesions. They originate from ectodermal remnants as a result of incomplete cleavage of neural ectoderm from the cutaneous ectoderm in the neural groove during the neural tube closure phase [23]. Epidermoid cysts can arise from any part of the craniospinal neural axis, with 90% of epidermoid cysts in the intradural space and 10% of epidermoid cysts in the extradural space [5]. In epidermoid cysts, rupture, hemorrhage, or aseptic meningitis can occur as complications [16]. Malignant transformation of epidermoid cysts has rarely been reported [7].
Intradiploic epidermoid tumors usually occur as a result of entrapped ectodermal remnants within the skull bones or, rarely, secondary to trauma [28]. In this case report, the patient had no history of head injury prior to the diagnosis of this disease. Therefore, the mass in this case was considered a primary inlesion, not a secondary lesion due to head injury. Epidermoid cysts account for approximately 0.2–1.8% of all intracranial tumors, and of these epidermoid cysts, only 25% are intradiploic [291011]. Although epidermoid cysts are slow growing, they often reach a large size without any neurological symptoms [12]. In general, epidermoid cysts measuring more than 5 cm are known as giant epidermoid cysts. Giant intradiploic epidermoid cysts are rare and only a small case series describing them have been published in the literature, so their true incidence is unknown [910111213141516]. Intradiploic epidermoid cysts may usually present with headache or as a painless local swelling [117]. In our case, the patient presented with only headache, without any local swelling. This finding recommends careful assessment of a patient with persistent localized headache, even without any palpable scalp mass.
The diagnosis of an intracranial epidermoid cyst is suggested by various imaging studies, including X-ray, CT, and MRI, and confirmed by histopathology. Skull X-rays shows expansile lytic areas with sharply defined sclerotic borders, expansion of the inner and outer tables of the skull and bony erosion, which are observed in both the inner and outer tables in 46% of cases and only in the outer table in 36% of cases [1819]. CT scans usually show well-defined lobulated hypodense masses, and they occasionally display calcification in the cyst wall [152021]. The higher attenuation may be explained by a high protein content [22]. In our case, the CT scan showed a large, hypodense mass with an internal higher signal density and bony erosion. On MRI, epidermoid cysts usually show isointensity to cerebrospinal fluid (CSF) signal on T1-weighted and T2-weighted MRI and hyperintense intensity relative to CSF signal on fluid-attenuated inversion recovery images [2123]. On the other hand, the T1-weighted MRI signal intensity may change according to the components in epidermoid cysts [22]. T1-weighted gadolinium-enhanced MRI usually shows no contrast enhancement of these lesions [22]. Differential diagnoses should include dermoid cysts, hemangiomas, arachnoid cysts, cholesterol granulomas, and/or osseous tumors such as aneurysmal bone cysts, fibrous dysplasia, and eosinophilic granulomas [71924]. Dermoid cysts are more frequently diagnosed in childhood and are usually located along the midline [24]. Hemangiomas have a typical appearance, including a honeycomb or radiating sunburst pattern [24]. Arachnoid cysts, which are very rarely located in the skull, similar to intradiploic cysts, can be distinguished from epidermoid cysts on DWI, where the latter usually present with high signal intensity while the former demonstrate low signal intensity [252627]. Eosinophilic granulomas usually occur in children and young adults and show contrast enhancement on MRI [24]. In our case, although the mass was difficult to differentiate from other osteolytic skull lesions, our radiological diagnosis was intradiploic epidermoid cyst based on the patient's age and radiological findings, including the paramedian location of osteolytic skull lesion, the lack of dural invasion and contrast enhancement, and diffusion restriction on MRI.
Surgical indications for epidermoid cysts include increased size, progression of neurological deficit, and/or malignant transformation [4]. In intradiploic epidermoid cysts, complete surgical excision followed by appropriate cranioplasty is the treatment of choice. Total removal of these lesions, including the cyst wall, is associated with a good prognosis [31528]. Arko et al. [17] analyzed the outcome of a total of 169 intradiploic epidermoid cysts that were previously described. The authors reported that the recurrence rate was only 5.8%, and of these recurrent cases, malignant transformation to squamous cell carcinoma occurred in 44% (4 of 9 cases) [17]. Most of these cases might be related to incomplete resection of primary intradiploic epidermoid cysts [17]. We completely removed the epidermoid cyst with its capsule from our patient (Fig. 2). The patient was free of recurrence at the 24-month follow-up.
In this article, a rare case of intradiploic epidermoid cyst located in the occipital bone is presented with clinical and radiologic features, and surgical treatment. It is important to consider this diagnosis in a patient who presents with persistent regional headache and/or a slowly growing scalp mass. Correct radiologic evaluation and complete surgical resection are important for favorable long-term outcomes.
Go to :
 XML Download
XML Download