

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
‘Diffuse midline glioma (DMG), H3K27M-mutant’ is a newly established disease entity according to the 2016 revised version of the World Health Organization (WHO) classification of brain tumors [1]. H3K27M-mutant DMGs are high-grade gliomas (WHO grade IV) associated with local infiltration and a poor prognosis of an average survival time of less than one year [2]. The pons is the most common location of H3K27M-mutant DMG, however, they can also occur in the thalamus, spinal cord, and other midline locations in patients of all DMGs [3]. Importantly, H3K27M-mutant DMG is a pathologic diagnosis and is not synonymous with the clinical and radiologic entity of diffuse intrinsic pontine glioma (DIPG). DMG is a part of disease that was previously classified as ‘DIPG’ or ‘brain stem glioma’. Approximately 80% of biopsied DIPGs harbor mutations at position K27 in one of several histone-encoding genes [456].
Despite the dismal prognosis of DMG, there are few randomized controlled clinical trials to establish the evidence-based standard treatment protocol. In general, surgery, radiotherapy, and chemotherapy can be considered as treatment options for DMG. If it is feasible, maximal safe resection can be considered as an initial treatment of choice. However, no superior treatment modalities including radiotherapy, chemotherapy, and/ or surgery, have been recommended alone or in combination to others. There are no unified (inter)national guidelines of radio- and chemotherapy for DMG, which resulted in a heterogeneous application of treatments.
A practical guideline for the management of patients with central nervous system (CNS) tumors in Korea has been limited. Therefore, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society for CNS tumors, began to prepare guidelines for various types of brain tumors from February 2018. In 2019, a new Guideline Working Group chapter began to develop the practical guidelines for the management of DMG in Korea. The main purpose of KSNO guidelines for DMG is to 1) provide an opportunity to share relevant medical knowledge and experiences among experts through the development of treatment guidelines, 2) provide practical standard treatment information to medical staffs, 3) help determining the optimal treatment strategies for DMG through multidisciplinary approaches, and 4) prolong patient's life, improve quality of life, and ultimately contribute to the improvement of national health.
Go to : 
KSNO GUIDELINE WORKING GROUP
A new chapter of Working Group was appointed by the KSNO in 2019 to develop a clinical guideline for management of patients with brain tumor. These guidelines should be optimized considering the unique medical circumstance in Korea. The KSNO Guideline Working Group was composed of 27 medical experts in Korea, including 15 neurosurgeons, 6 radiation oncologists, 1 medical oncologist, 2 neuroradiologists, 2 pathologists, and 1 neurologist.
References were identified by searching PubMed, MEDLINE, EMBASE, and Cochrane CENTRAL databases using specific and sensitive keywords as well as combinations of keywords. After ‘diffuse midline glioma, H3K27M-mutant’ was proposed as a new diagnostic entity in 2016, all retrospective and prospective clinical studies of this disease were reviewed. As there was no international guideline for management of DMG yet, the guidelines for the treatment of ‘DIPG’ or ‘brain stem glioma’ were also reviewed to develop this new guideline. If available, existing guidelines from national multidisciplinary neuro-oncological societies such as the National Comprehensive Cancer Network (NCCN) and European Association of Neuro-Oncology (EANO) were also collected. The language was limited to English and Korean. The publication year was not limited, but the papers published after 2016 were weighted more because DMG is a newly established disease entity since 2016. The selection of search terms and selection of suitable papers were conducted by reflecting the opinions of the members in charge. After reviewing the papers, a total of 51 papers were selected as references for this guideline.
Scientific evidence was evaluated and graded according to the following categories: high level evidence (obtained from multiple populations and derived from randomized clinical trials or meta-analysis or systemic review), and low level evidence (obtained from limited population and derived from non-randomized studies, including observational studies, cohort studies, and case-control studies).
To establish the recommendation levels, the following criteria were used. Level I (strong recommendation) required a high level evidence and uniform agreement among panels. Level II (weak recommendation) required a high level evidence but not uniform agreement among panels or low level evidence but uniform agreement among panels. Level III (no consensus; individual decision) required a low level evidence but not uniform agreement among panels. Level IV (not recommended) required contents being not beneficial or harmful.
Go to :
DIAGNOSIS OF DIFFUSE MIDLINE GLIOMA
DMG is a rare type of glial tumor that occurs in the CNS. Previously, it referred to as ‘DIPG.’ More recently, it was known that some DIPGs with a specific mutation (H3K27M mutation) show characteristically dismal prognosis. Therefore, the 2016 revised WHO classification redefined this type of tumors as ‘diffuse midline glioma, H3K27M-mutant’, a new diagnostic entity based on its unique genetic signature [1]. Characteristically, 1) it is located in the midline of the brain (brain stem, spinal cord, cerebellum, thalamus, etc.), 2) shows a diffuse growth pattern, and 3) shows K27M mutation in H3F3A or HIST1H3B/C (H3K27M mutation) [789]. Because surgical resection is often difficult due to the delicate location of the tumor [1011], proper imaging and biopsy are required for accurate diagnosis of DMG [1213]. However, in some tumors, the location is often not suitable to perform a biopsy [1011]. According to the previous European survey for health care professionals treating DIPG patients, only 13.5% of the respondents said to do biopsy all of their patients, while 41.9% of the respondents said to do biopsy their patients infrequently [14]. Characteristic radiologic findings shown only in DMG have not yet been clearly defined, and studies involving adult patients are further lacking. In general, when diagnosing by imaging findings without confirming the presence of H3K27M mutation, the presence of ‘extensive invasion’ in the midline structures of the CNS is an important finding. However, as these radiologic features are not shown in all cases, and histologic confirmation is more critical, sufficient discussion should be preceded when physicians diagnose this disease entity radiologically.
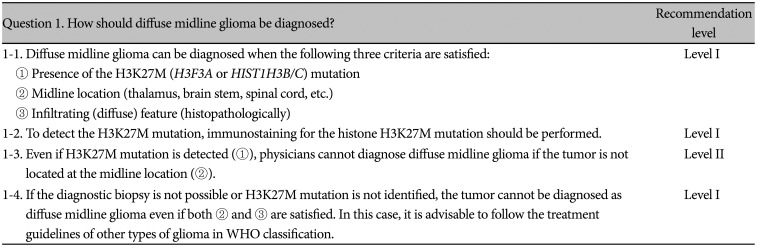
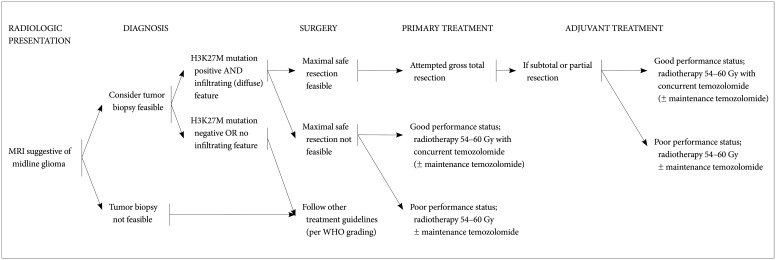
In summary, DMG can be diagnosed when all of the following three criteria are satisfied: 1) the presence of the H3K27M (H3F3A or HIST1H3B/C) mutation, 2) midline location (thalamus, brain stem, spinal cord, etc.), and 3) infiltrating (diffuse) feature (Level I). Since the confirmation of H3K27M mutation is the most important diagnostic criteria for DMG rather than clinical and imaging features, tumor biopsy should be considered first (Level I) and immunostaining for the histone H3K27M mutation should be performed to detect the H3K27M mutation (Level I) [15]. Instead, detection of EGFR hotspot mutation or EZHIP overexpression can be used to diagnosis DMGs [16]. If histopathological feature of diffusely infiltrative growth in glioma at midline location and H3K27M mutation are detected, physicians can diagnose DMG (Level I). Even if H3K27M mutation is detected, physicians cannot diagnose DMG if the tumor is not located at the midline location (Level II). If the diagnostic biopsy is not possible or H3K27M mutation is not identified, the tumor cannot be diagnosed as DMG even if both location (midline) and infiltrating feature are satisfied. In this case, it is advisable to follow the treatment guidelines of other types of glioma in WHO classification (Level I) (Fig. 1, Table 1).
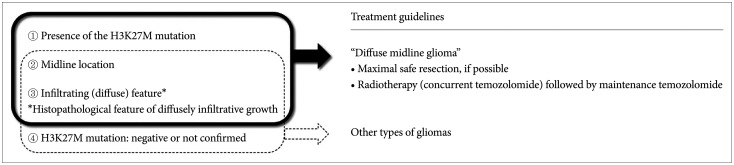 | Fig. 1Diagnosis algorithm for diffuse midline glioma (DMG). To diagnose DMGs, detection of H3K27M mutation, the location of tumor (midline location), and infiltrating feature are essential (➀+➁+➂). In other words, physicians are not recommended to diagnose DMG if the tumor is not located at the midline location (➁), even if H3K27M mutation is detected (➀). Also, if the diagnostic biopsy is not possible or H3K27M mutation is not identified (➃), the tumor cannot be diagnosed as DMG even if both location (midline) (➁) and infiltrating feature (➂) are satisfied.
|
Table 1
Guideline for diagnosis of diffuse midline glioma
![]()
Go to :
PRINCIPLES OF MANAGEMENT OF DIFFUSE MIDLINE GLIOMAS
Decision for primary treatment
Customarily, managements of DMG have followed the standards of care for gliomas of the same WHO grade [1718]. Combinations of surgery, radiotherapy, and chemotherapy can be considered as the treatment options for DMG [141519]. For tumors that can be surgically resected safely, maximal safe resection should be considered first (Level II). The goal of surgery is to obtain tissue for genetic diagnosis and to reduce the tumor burden without harming neurological status of the patient [15181920]. However, the brainstem, thalamus, and spinal cord are neurologically critical structures and surgical procedures in these areas can cause serious irreversible deficits. Thus, management strategies including the scope and purpose of the surgery must be carefully determined through multidisciplinary discussion (Level II). Even if maximal safe resection is not feasible, biopsy of the tumor should be essentially considered to confirm the presence of H3K27M mutation for the diagnosis of DMG (Level II).
In addition to the surgical resection, radiotherapy and chemotherapy can also be added for the management of DMG [1014151719]. Radiotherapy is the primary treatment option when the complete surgical resection is not feasible which is in the majority of cases (Level II). Concurrent chemotherapy using temozolomide can be considered when performing radiotherapy (Level II). Sequential chemotherapy after radiotherapy can also be performed in some cases. However, there has been no chemotherapy regimen which demonstrated meaningful benefit in DMG [212223]. There is also a lack of reports that concurrent chemotherapy is superior to radiotherapy followed by chemotherapy, radiotherapy alone, or chemotherapy alone. Given these limitations, each plan should be tailored to each patient. A multidisciplinary discussion among experts including neuro-oncologists, neuroradiologists, radiation oncologists, and neurosurgeons, is important to determine the best treatment plan. At any time during the course of treatment, it is necessary to actively apply symptom-controlling drugs or procedures such as steroids or ventriculoperitoneal shunt when necessary (Level I) (Table 2).
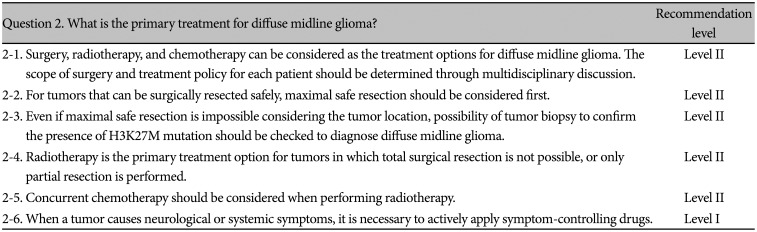
Table 2
Guideline for primary treatment decision of patients with diffuse midline glioma
![]()
Radiotherapy
To determine the dose scheme of radiotherapy, it would be reasonable to follow the radiotherapy policy of DIPG, as the relevant papers for DMG are still lacking. Radiotherapy has been regarded as an important treatment option for brainstem glioma. In current situation, similar doses and fields can be recommended when performing radiotherapy in DMG. A total dose of 54 Gy to 60 Gy with conventional fractionation (1.8–2.0 Gy daily given five days per week) is recommended (Level II) [24]. Total dose of radiation should be determined by radiation oncologists. The dose-constraint of the brainstem should always be kept (Level II). Dose escalation is not recommended (Level II). The radiotherapy field can be defined as 1–2 cm plus gross tumor volume (GTV) (Level II) [25]. GTV includes not only contrast-enhancing lesions but also hyperintense lesions seen on T2-weighted, FLAIR images (Level II). For radiotherapy techniques, three-dimensional conformal radiation therapy using X-rays, intensity-modulated radiation therapy, and proton therapy [26] can be considered for radiotherapy techniques (Level II).
Despite multiple trials of dose escalation, hyperfractionated radiotherapy [272829303132333435], hypofractionated radiotherapy [3637383940], and radiosensitization, none of these modulations have been proven more effective than the conventional radiotherapy. Patients with severe symptoms may require urgent initiation of radiotherapy. Due to the poor prognosis in patients with DIPG, hypofractionated radiation therapy has been evaluated to minimize the time spent in treatment. In a randomized trial of 71 children with newly diagnosed DIPG, a regimen of thirteen 3.0 Gy fractions was well tolerated, and median overall survival approached that of radiation therapy given over six weeks (7.8 versus 9.5 months) [3641]. Based on this result, depending on regithe patient's condition and tumor location, the corresponding dose with hypo-fractionation can also be prescribed instead of 54–60 Gy with conventional fractionation in DMG (Level III).
Fractionated re-irradiation may be considered at the time of progression to temporarily extend palliation, although increased toxicities may result from this approach [4243]. In a small prospective dose-escalation study of DMG, the lowest dose level (24 Gy in 12 fractions) was well tolerated and achieved imaging, clinical, and/or quality-of-life improvement in most patients; in all 12 patients, progression-free and overall survival from the start of re-irradiation were 4.5 and 5.8 months, respectively [44]. Also, re-irradiation may be considered to control symptoms and improve the survival outcomes in well-selected patients with persistent disease progression [42454647]. For the re-irradiation dose, 20–40 Gy with conventional fractionation can be recommended based on recent studies (Level III). Depending on the patient's condition, corresponding dose with hypo-fractionation radiotherapy (≤3 Gy per fraction) can also be prescribed (Table 3).
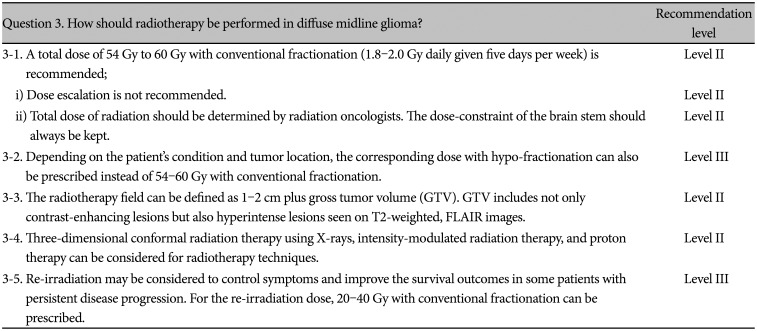
Table 3
Guideline for radiotherapy of patients with diffuse midline glioma
![]()
Chemotherapy
No chemotherapy has been proven to be effective in DMG or DIPG. Numerous treatment protocols, including single chemotherapy agents, multi-drug combination regimens, and high-dose therapy with stem cell rescue, have been tested in both adults and children without clear evidence of benefit [144849505152535455]. Although temozolomide has become part of standard therapy for most adult patients with high-grade gliomas, testing in combination with radiotherapy for newly diagnosed DIPG has demonstrated no improvement in activity compared with radiation alone and is associated with increased risk for side effects and toxicity [385255]. Besides, the incidence of O6-methylguanine-DNA methyltransferase (MGMT) methylation itself was reported to be low in DMG [9]. Clinical trials using other drugs, such as gefitinib, ONC201, and panobinostat, failed to show any clear benefits [5657585960].
Nevertheless, temozolomide can be considered first as a chemotherapy regimen in DMG during- and post-radiotherapy (Level II) in the absence of other suitable chemotherapy regimen. The reason is that temozolomide has been proven to be an effective and safe drug for the same WHO grade (grade IV) of other brain tumors. In addition, temozolomide acts as a radio-sensitizer when administered together with radiotherapy, thereby enhancing the therapeutic effects of radiation. Therefore, concurrent chemoradiotherapy (± maintenance chemotherapy) can be considered a primary treatment or adjuvant treatment after surgery in DMG (Level II). However, since concurrent chemoradiotherapy may increase treatment-related toxicity, careful decision case by case is needed considering the patient's condition. If the patient is in old age or in poor condition, temozolomide may be prescribed sequentially after radiotherapy or radiotherapy alone is recommended (Level II). If the disease progresses after radiotherapy, maintenance chemotherapy using temozolomide can be applied (Level III). The single agent or combination therapy of chemotherapeutic agents other than temozolomide can be tried only after full multidisciplinary discussion (Level III). Clinical trials are currently being attempted to prove the effectiveness of other chemotherapeutic agents in DMG, and according to the results, recommendations for chemotherapy may change shortly (Table 4).
Table 4
Guideline for chemotherapy of patients with diffuse midline glioma
![]()
Go to :
CONCLUSION
Until now, there has been no practical guideline for the management of adult patients with DMG in Korea. Thus, the KSNO developed this guideline applicable to the current medical circumstances in Korea. “The KSNO Guideline for Adult Diffuse Midline Glioma: Version 2021.01” is the first guideline for H3K27M-mutant diffuse midline glioma in Korea (Fig. 2), prepared by the KSNO Guideline Working Group.
In summary, it is recommended to confirm the presence of H3K27M mutation after the maximal safe resection or biopsy to diagnose the DMG. Radiotherapy is recommended as a primary (or adjuvant) treatment option for tumors incapable of complete resection and concurrent chemotherapy with temozolomide can be considered. However, considering that evidence is still lacking, and treatment-related toxicity may be increased in some patients after concurrent radio-chemotherapy, treatment policy for each patient should be determined through sufficient multidisciplinary discussion.
Go to :
 XML Download
XML Download