

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioblastoma (GBM) leptomeningeal spread (LMS) results from the spread of tumor cells from the brain parenchyma to the leptomeninges and cerebrospinal fluid (CSF) space and is considered one of the most severe complications of GBM [123].
The reported incidence of LMS after the diagnosis of GBM is approximately two-thirds of patients within the first two years of diagnosis. However, the estimated incidence of symptomatic LMS has been reported to be 2%. This is probably underestimated because of the undiagnosed and asymptomatic cases [1].
Since there is no standard treatment guideline for LMS in patients with GBM, it is considered as end-stage complication of the disease. The post-LMS diagnosis survival time was 0.2–9.7 months with a mean of 4.7 months [145].
Several therapeutic approaches for LMS, including intrathecal chemotherapy, radiation therapy, and recently, molecular targeted therapy, have been attempted; however, survival after diagnosis of LMS in GBM is not lengthened for more than eight months [6789101112].
We present a case of 31-year-old man with GBM and LMS diagnosed by early enhanced MRI and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) studies, which can suggest primary LMS.
CASE REPORT
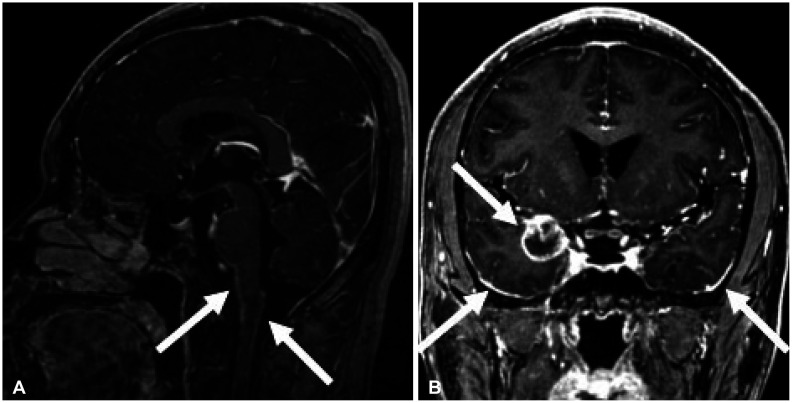
A 31-year-old man was transferred from Dankook University Medical Center at Cheonan, where he presented with seizures, headache, and incipient papilledema. However, his neurological examination were normal with no history of extracranial primary carcinoma. Brain MRI revealed a small mass lesion localized in the right temporal lobe with leptomeningeal enhancement on the ventral side of the brain stem. No peritumoral edema or restricted diffusion was observed (Fig. 1). Contrast-enhancing lesions in the right temporal lobe and leptomeningeal contrast enhancement on the ventral side of the brain stem were seen on MRI, in addition 18F-FDG PET/CT showed multifocal high metabolic uptake lesions in the brain and spinal cord. We suspected a primary brain tumor with the LMS at the time of GBM diagnosis, which is very rare even in malignant primary brain tumors.
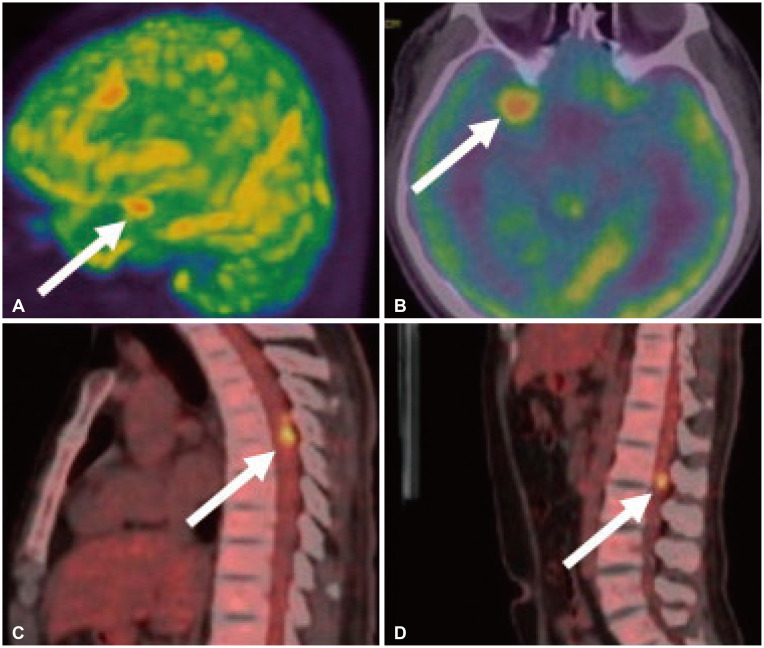
However, metastasis from an extracranial source needs to be ruled out; therefore, brain metastasis workups were performed. There was no enhancing tumorous lesion on CT scans of the abdomen and chest. Whole-body 18F-FDG PET/CT was also performed, which revealed high metabolic uptake lesions at the left central sulcus, left Sylvian cistern, skull base, and spinal cord of T5/6, L1 spinal levels (Fig. 2). A subsequent spinal MRI showed enhanced lesions corresponding to the 18F-FDG PET/CT image. Optic fundus examination revealed papilledema.
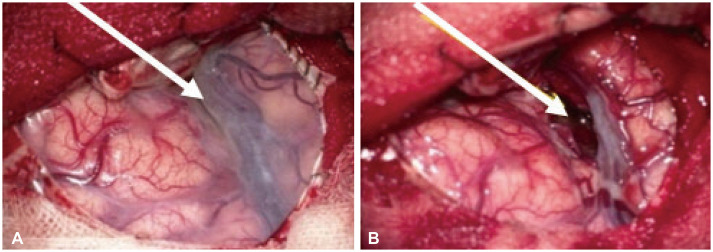
Craniotomy was performed for accurate diagnosis and excision of the tumor (Fig. 3). During surgery, the cortical surface anatomy appeared normal and the mass was located in the deep proximal Sylvian fissure. The superficial cortical subarachnoid space appeared normal, and leptomeningeal thickening was not observed. The tumor was composed of gray-colored soft tissue with no cystic portion. Gross total removal was performed. Intraoperative frozen biopsy revealed the tumor as a high-grade malignant tumor, such as metastasis or lymphomatous tumor, and is unlikely to be a high-grade glial tumor.
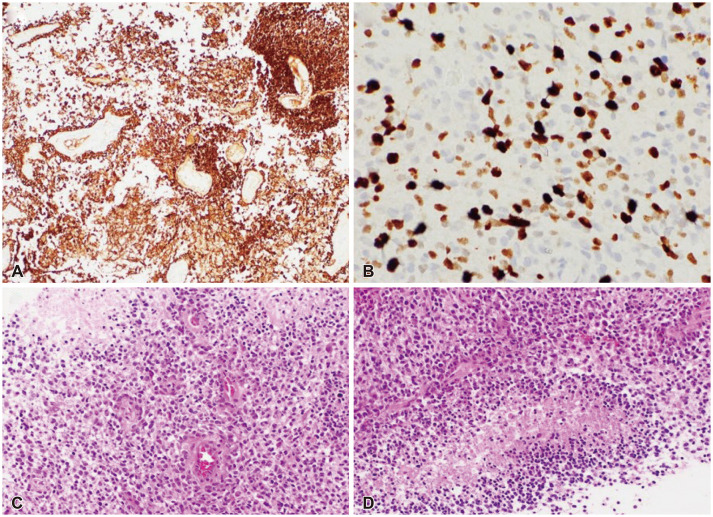
Pathologic examination of the specimen showed as follows. A microscopic view of the hematoxylin and eosin (H&E) stain revealed nuclear pleomorphism, mitosis, microvascular proliferation, and necrosis (Fig. 4). Immunohistochemical staining was positive for glial fibrillary acidic proteins. The final pathologic report revealed GBM with isocitrate dehydrogenease (IDH)-wild type (Grade 4) and positive O6-methylguanine methyltransferase (MGMT) promoter methylation.
Therefore, concurrent chemoradiation therapy was initiated. However, five days after surgery, the patient fell into a stupor and was unable to obey verbal commands. A follow-up brain CT scan showed no definite changes or intracranial hemorrhage, but the electrolyte profile exhibited salt-wasting syndrome. Seven days after craniotomy, the patient presented with uncontrolled intracranial hypertension and a decreased heart rate. Under the diagnosis of increased intracranial pressure (ICP) and papilledema with acute hydrocephalus, a ventriculo-peritoneal (VP) shunt was performed. Although a small amount of CSF had spilled out of the dura, the ICP was still 54 cm H2O. The dura mater was bulged and tense upon palpation. One week after the VP shunt, the patient recovered his alert mental status but exhibited paraplegia, and MRI confirmed increased tumor size at L1 spinal lesion (from 2.3 cm to 2.8 cm).
One month after craniotomy, the patient underwent modified low-dose raditherapy at 39.6 Gy due to bone marrow suppression. Temozolomide treatment was postponed for three weeks due to multi-focal pneumonia and fever.
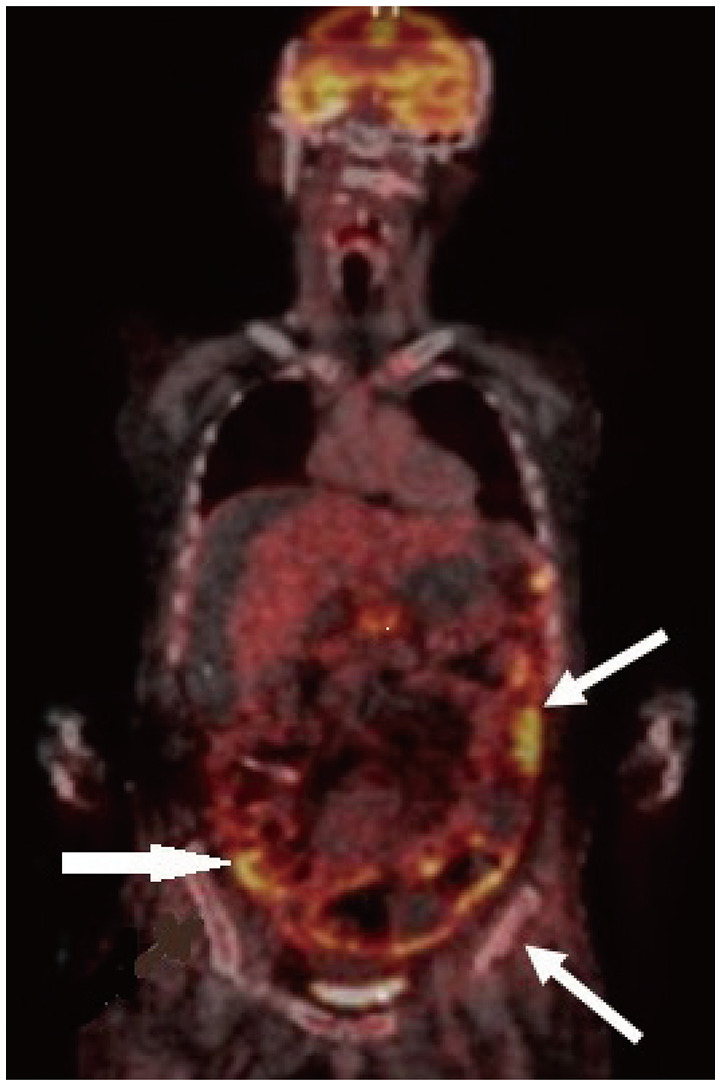
The patient experienced moderate upper right quadrant abdominal pain. Abdominal CT has shown no definite changes since the last study. Since the circumference of the patient’s abdomen continued to increase, suggesting a normal-functioning VP shunt, abdominopelvic CT and whole-body 18F-FDG PET were performed. Follow-up abdominopelvic CT showed increased ascites, peritoneal thickening, and nodular infiltration. In addition, 18F-FDG PET/CT showed lesions with high metabolic uptake in the abdomen and pelvic bone, which was considered abdominopelvic metastasis (spread) of the GBM (Fig. 5). Paracentesis for relieving the distended abdomen was performed seven times. Nonetheless, evidence of malignant cells was not found in any of the cytological studies of ascitic fluid. The clinical status progressively deteriorated.
Nine months after the diagnosis of GBM and LMS, the patient succumbed to the disease with multiorgan failure due to septic conditions.
DISCUSSION
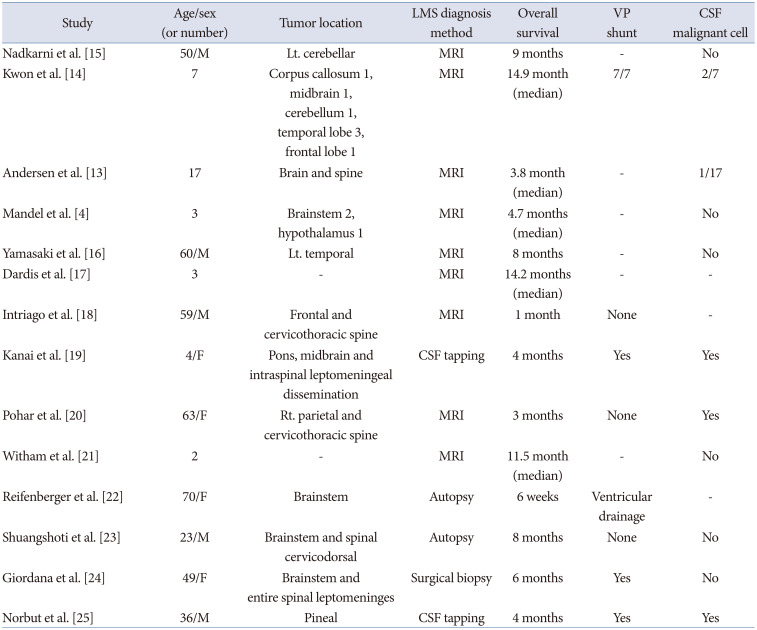
We present a rare case of primary GBM with simultaneous LMS (brain and spinal cord, primary LMS), followed by abdominal metastasis via a VP shunt. Other case reports of primary GBM with concurrent LMS at the time of diagnosis are summarized in Table 1 [413141516171819202122232425]. The LMS results from the spreading of tumor cells from the brain parenchyma via the perivascular space to the subpial, leptomeninges, and CSF. It is one of the most severe complications of GBM and implies a more aggressive behavior and a worse prognosis. Patients with LMS may experience increased ICP, hydrocephalus, and cranial nerve palsies [226]. Intractable vomiting may occur in patients with fourth ventricular involvement, but the frequency of seizures does not seem to increase because of LMS [27]. Moreover, a recent review article reported that two-thirds of patients with GBM develop LMS within the first two years after the diagnosis of GBM, and the median delay to the diagnosis of LMS varies from 5 to 16.4 months. In addition, this delay may be shorter in specific tumor locations, such as the pineal, spinal, periventricular, and infratentorial regions [1228]. In this case, the LMS was present in the whole brain and spinal cord at the time of the diagnosis of temporal lobe GBM, which was in contact with the Sylvian cistern and may have contributed to the LMS. This pattern of LMS at the time of GBM diagnosis is very rare compared to secondary LMS during the treatment or recurrence of GBM.
No risk factors for LMS of GBM have been demonstrated, although multiple factors have been suggested, such as age, histological features, molecular alterations, anatomical tumor site, tumor volume, and therapeutic interventions [1].
In retrospective studies and case series regarding GBM with LMS, the mean overall survival after diagnosis of treated LMS was 4.94 months (range, 2–9 months). Our patient survived for 9 months after the diagnosis of LMS and GBM. However, the patient showed rapid initial disease progression. One week after tumor removal, the patient underwent a VP shunt due to increased ICP and hydrocephalus with a stupor mentality. One month after the tumor removal, the patient developed paraplegia.
The LMS of GBM can be classified into two types. The first type is a positive parenchymal GBM with concurrent LMS at diagnosis (primary LMS). The second type is GBM with delayed LMS during treatment or recurrence of GBM (secondary LMS). Most LMS cases of GBM are of the secondary LMS type. However, our case was of the first type (primary LMS).
A comparison between the survival time of our patient (primary LMS) and the current mean overall survival data for GBM (secondary LMS) indicated a shorter overall survival of our patient (9 months); however, if survival after diagnosis of LMS was compared, the survival time of our patient was in the upper range of the survival data (2–9 months). Primary and secondary LMS survival after the diagnosis of LMS did not seem to differ, which means that LMS negatively affected the overall prognosis of GBM.
As the patient’s abdominal circumference continued to increase, we had to do consecutive paracentesis seven times to relieve abdominal distension and alleviate compromised respiration. The aspiration fluid volume varied from 200 mL to 1,000 mL each time. All the samples were used for the fluid cytology test, which was negative for malignant cells. A direct peritoneal biopsy may be an option for the diagnosis of LMS in cases with repeated negative ascitic fluid analysis of malignant cells. However, in this case, a surgical peritoneal biopsy was not performed because of poor performance status and physical burden, a probable surgical complication related to a distended abdomen due to ascites, and no additional treatment modality could be beneficial to the patient. CSF cytologic positivity in GBM with LMS is variable, 4%–75% of cases [131329]. From a practical point of view, there is no doubt that persistent ascites despite repeated paracenteses are related to the peritoneal spread of GBM cells and compromising the peritoneal CSF absorption capacity, not the problem of shunt malfunction. In this case, 18F-FDG PET/CT was helpful for the clinical diagnosis of LMS in the peritoneal cavity.
In conclusion, the overall survival of primary LMS with GBM in our case was nine months, which is shorter than that of secondary LMS with GBM. The survival period after the diagnosis of LMS did not seem to be significantly different between primary and secondary LMS. To evaluate the prognostic effect and differences between primary and secondary LMS, further cooperative studies with large volumes of data are warranted.
 XML Download
XML Download