

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioblastoma multiforme (GBM) is notorious for its poor prognosis due to the high recurrence rate, even after surgical resection [12]. The highly infiltrative nature of GBM cells makes them difficult to completely remove by incision surgery without damaging normal brain tissue [34]. Consequently, adjuvant therapies including radiotherapy and chemotherapy are also administered as standard postoperative treatment; however, their therapeutic efficacy is limited by the inherent features of GBM [56]. Radiotherapy is hindered by radiation tolerance induced by genetic heterogeneity and frequent mutation of GBM cells [78]. Additionally, chemotherapy (e.g., oral administration of temozolomide) is impeded by the blood-brain barrier (BBB), which lowers the efficiency of systemic drug delivery to GBM cells [9].
However, the systemic administration of drugs is still preferred among treatment options for GBM, as this method is easily accessible and less burdensome to patients [10]. Therefore, systemic drug delivery strategies to penetrate the BBB and increase delivery efficiency have been developed [11]. For example, nanoparticles with modified ligands capable of crossing the BBB have been suggested [121314]. In addition, temporal opening of the BBB using external stimuli such as ultrasound has been studied to promote systemic drug delivery efficiency [1516]. Although many studies have successfully improved systemic drug delivery efficiency, they are still insufficient to completely cure GBM. Systemic drug delivery strategies exhibit clear limitations as their long delivery routes induce a high probability of drug absorption by other organs, or drug clearance during blood circulation. Additionally, the risk of systemic toxicity remains a concern [1718].
Thus, local drug delivery methods that directly administer drugs to the brain have been proposed as promising solutions. The local delivery approach can dramatically enhance delivery efficiency by bypassing the BBB. Various types of local drug delivery strategies, such as intracranial delivery [1920], convection-enhanced delivery (CED) [2122], and intracranial implant-based delivery [2324], have been developed [1025]. These macroscopic approaches have been further strengthened by the integration of microscopic approaches including the molecular design of drugs and/or incorporation of therapeutic nanomaterials. Recently, the use of electronic devices (e.g., sensors and actuators), which were already approached for the theranostic applications of brain [26272829], has also been proposed. The integration of electronics with soft and nanomaterials applied for other biomedical applications [30313233] shows the great potential of such approaches to GBM treatment. These advances in local drug delivery methods have allowed for the introduction of new perspectives on GBM treatment.
In this article, we review the recent progress in local drug delivery technologies for GBM treatment with a focus on electronics-assisted drug delivery methods. First, we introduce various conventional local drug delivery strategies, and the characteristics of commercialized drug delivery methods are described. Subsequently, representative research-level local drug delivery methods, classified into macroscopic and microscopic approaches, are presented. We then focused on studies using electronic devices for GBM treatment, a recent innovation in local drug delivery technology. Finally, we conclude this review by presenting the issues to be addressed in the future, and the developmental direction of local delivery approaches to achieve complete recovery from GBM.
Go to : 
LOCAL DRUG DELIVERY STRATEGIES FOR GBM TREATMENT
The local drug delivery strategy for GBM treatment has many advantages over systemic drug delivery, including superior drug delivery efficiency and minimal systemic side effects of the toxic chemotherapeutic drugs. However, it should be accompanied by surgery of the skull and dura to obtain direct access to the target site of the brain, resulting in a large physical and economic burden to the patient. To minimize this disadvantage, local drug delivery devices can be implanted during surgical resection of brain tumors, or applied through minimally invasive procedures [3435]. This chapter comprises three subchapters on clinically available, research-level, and electronics-assisted local drug delivery strategies, and describes various local delivery strategies with explanations of both their advantages and disadvantages.
Clinically-available local drug delivery strategies
Among the various local drug delivery strategies, the therapeutic efficacy and biocompatibility of several methods could be proven; these methods could thus be approved for clinical implementation in GBM patients. This subchapter describes these clinically available local drug delivery methods (e.g., intracranial injection, CED, and solid-state implants).
Intracranial injection of therapeutic agents can deploy therapeutic moieties directly into the target brain region. Since the drug is directly injected into the target site, this method exhibits the clear advantage of excellent drug delivery efficiency. Furthermore, the location of the injection can be controlled at a high spatial resolution using a catheter or syringe, which minimizes unwanted exposure of chemotherapeutic drugs to normal brain tissue. However, this bolus injection method still shows therapeutic efficacy below expectations owing to the rapid dissipation and backflow of the injected drugs. To overcome these shortcomings, macroscopic drug injection tools (e.g., infusion convection pump) (Fig. 1A) [363738] or microscopic drug delivery vehicles (e.g., liposomal doxorubicin) (Fig. 1B) [3940] have been used together. In particular, CED using a pressure gradient generated by the pump has shown a noteworthy potential to promote drug delivery to the deep brain tissue as well as improve the drug injection procedure.
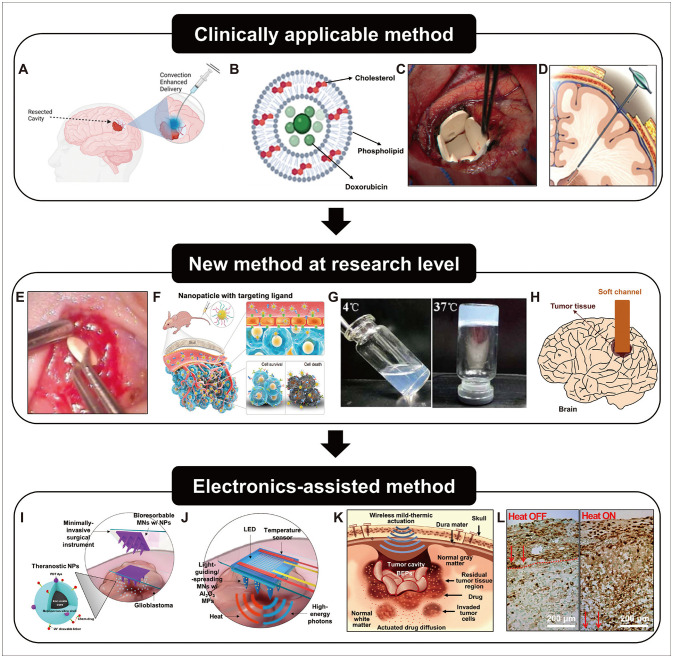 | Fig. 1Local drug delivery strategies. A: Schematic illustration of convection enhanced drug delivery compared to the normal diffusion method. B: Schematic illustration of the structure of the liposomal doxorubicin. C: Optical image of the Gliadel wafer implanted on the cavity after resection. D: Schematic illustration of the Ommaya reservoir implanted into the brain. E: Optical image of a nanofiber wafer implanted on the brain. F: Schematic illustration of the administration of the therapeutic nanoparticles conjugated with targeting moieties for the glioblastoma multiforme treatment. G: Optical image of the GemC12-lipid nanocapsules hydrogel implanted on the cavity after resection. H: Schematic illustration and optical image (inset) of the tumor-guiding conduit implanted on the tumor tissue in the brain. I: Schematic illustration of the delivery of theranostic nanoparticles (NPs) using bioresorbable microneedles (MNs). J: Schematic illustration of the delivery of the high-energy photons using light-guiding microneedles with microparticles (MPs), light-emitting diode (LED), and bioelectronics. K: Schematic illustration of drug delivery by the bioresorbable electronic patch (BEP) with magnetic actuation. L: Optical image of tumor tissues without (left) and with (right) the magnetic actuation. A: Adapted from Pena et al. Int J Mol Sci 2021;22:13160 [38]; B: Adapted from Ibrahim et al. Pharmaceutics 2022;14: 254 [40]; C: Adapted from Kleinberg. Patient Prefer Adherence 2016;10:2397-406 [42]; D: Adapted from Lau et al. Cureus 2012;4:e66 [43]; E: Adapted from Ramachandran et al. Sci Rep 2017;7:43271 [48]; F: Adapted from Meng et al. Nat Commun 2020;11:594 [50]; G: Adapted from Shi et al. Sci Rep 2016;6:19077 [52]; K and L: Adapted from Lee et al. Nat Commun 2019;15;10:5205 [58]; under the Creative Commons license. I and J: Adapted from Lee et al. Adv Mater 2021;33:2100425, with permission from John Wiley and Sons [57].
|
Implantable solid-state intracranial drug reservoirs have been developed for drug release over a longer period of time; they can significantly increase the drug loading capacity, and the nonfluidic property of the drug reservoir prevents rapid drug dissipation. However, this method requires a surgical opening of the skull for implantation of the solid-state device; thus, they are usually implanted during the surgical resection of tumors.
One representative example of solid-state implants is the Gliadel wafer (Arbor Pharmaceuticals, LLC, Atlanta, GA, USA) (Fig. 1C) [244142]. It includes a mixture of biodegradable polymers and alkylating agents (i.e., carmustine; 1,3-bis(2-chloroethyl)-1-nitrosourea) and is implanted in the cavity after resection of the brain tumor. After implantation, the drug is released into the brain tissue from the Gliadel wafer by natural diffusion, preventing GBM recurrence. However, its rigid cylindrical structure has a disadvantage in its application, as the drug released from the wafer is often washed away by the cerebrospinal fluid (CSF) that permeates the gap between the wafer and curved brain surface. This can diminish drug delivery efficiency and therapeutic efficacy. In addition, potential inflammatory issues exist due to the mechanical mismatch between rigid wafers and soft brain tissue.
The Ommaya reservoir (Fig. 1D), another type of solid-state implant, provides a conduit for drug administration from outside the brain [4344]. The device, made of soft plastic, consists of a reservoir dome located on the brain surface and a catheter that penetrates brain tissue. The drug can be periodically administered to the target region via the Ommaya reservoir. Consequently, the type and dosage of drugs can be changed to suit the patient’s condition during treatment. These advantages, achieved by adopting the Ommaya reservoir, are suitable for the long-term treatment of GBM. Furthermore, it can perform additional functions—such as CSF perfusion—which may help to monitor unexpected side effects by observing the status of the CSF. However, several side effects (including inflammation and infection) may occur due to prolonged exposure of the brain to the external environment via the Ommaya reservoir [45]. Although the small size of the device (e.g., the size of a quarter) minimizes the inconvenience of patients equipped with the Ommaya reservoir, they may face uncomfortable situations in their daily lives due to the permanent installation of the external device.
Research-level local drug delivery strategies
Clinically available local drug delivery strategies have shown significant improvements in treatment efficacy. However, further improvements are still required, as the median survival can only be extended by several months. Hence, various studies on novel and/or improved local drug delivery strategies have been conducted to enhance the therapeutic effect.
One research direction involves changing the materials used in conventional drug delivery devices. For example, solid-state drug-releasing implant (e.g., Gliadel wafer) can be replaced by soft drug-releasing materials, such as hydrogels [4647] and fibers [4849] (Fig. 1E). As soft and deformable material properties are compatible with soft brain tissue and curved surfaces, they can be advantageous for enhancing delivery efficiency and decreasing potential side effects. For example, the softness of implants prevents neurological side effects (e.g., seizure) induced by the mechanical mismatch between soft brain tissue and rigid implants. Furthermore, deformable features enable conformal integration of the drug delivery implant with curvilinear brain surface.
Another direction is to introduce nanotechnology into GBM treatment. Nanoparticles have been suggested as drug carriers for enhancing drug delivery efficiency by encapsulating the drugs and decorating the nanoparticle surface with functional moieties (Fig. 1F) [50]. To enhance the specificity of drug delivery, a tumor-targeting or stimuli-responsive moiety (e.g., pH-responsive group) is conjugated to the surface of the nanoparticles (Fig. 1F). Additionally, other functional moieties that could control drug release behavior (e.g., control of the degradation rate) or facilitate drug penetration (e.g., PEGylation) were studied. These approaches can be integrated with other macroscopic approaches to achieve synergistic therapeutic efficacy.
A new therapeutic platform with optimized administration methods has been reported. For example, a thermo-responsive injectable hydrogel, which can be administered to the brain via a minimally-invasive route, has been employed for GBM treatment (Fig. 1G) [5152]. When implanted, it gelates in response to body temperature without any external energy and can be fixed to the target site. These injectable-type implants can offset the shortcomings of solid-state devices that require incision surgery for implantation. The other advantages of hydrogels (e.g., softness, deformability, and high drug dose) [5354] for GBM treatment are also valid for soft drug-releasing implants based on injectable hydrogels.
Another approach is to exploit soft materials as a migration route that induces the movement of tumor cells to the drug reservoir [55]. This soft device comprises aligned nanofibers and polymers as channels, and a hydrogel as the drug reservoir. For treatment, the channel is inserted directly into the tumor, serving as a conduit between the hydrogel drug reservoir and tumor tissue (Fig. 1H). Owing to the aligned nanostructure, tumor cells preferentially move along the implanted conduit. Finally, these cells reach the drug reservoir and undergo apoptosis. Since all material components of the channel feature softness and biocompatibility, the suggested platform is relatively free from long-term safety issues when compared to platforms using a similar administration method, such as the Ommaya reservoir.
Electronics-assisted local drug delivery strategies
Several strategies have been suggested to improve the efficacy of GBM treatment. However, these efforts have not yet achieved the desired efficacy. New functions and capabilities, such as real-time sensing and meticulous drug delivery control, may further improve therapeutic efficiency. Several recent studies have presented novel drug delivery platforms that integrate flexible and/or biodegradable electronics with drug delivery nanoparticles or drug-releasing reservoirs [56].
For example, Lee et al. [57] presented a minimally-invasive local drug delivery and therapy platform comprising two types of microneedles integrated with bioelectronics. One was a bioresorbable microneedle containing theranostic nanoparticles for drug delivery and the generation of therapeutic reactive oxygen species (ROS) (Fig. 1I); the other was a light-guiding microneedle containing light-scattering alumina microparticles integrated with flexible electronics, containing an ultraviolet light-emitting diode (LED) and temperature sensor. When the bioresorbable microneedles dissolved, the nanoparticles were delivered to the target tumor tissue. Ultraviolet light generated by the LED then activates the nanoparticles to release the loaded chemotherapeutic drugs and generate ROS for photodynamic therapy (Fig. 1J). In addition, the LED generates heat, which accelerates the diffusion of the delivered/generated therapeutic moieties. The temperature increase is monitored by a temperature sensor; thus, thermal overshoot can be prevented.
Despite the potential of electronics-assisted local drug delivery as a minimally invasive treatment tool, its therapeutic efficacy remains insufficient. The major cause is the noncontinuous, rather than continuous long-term treatment protocol. Continuous treatment can be performed using implantable patches with onboard biodegradable electronics. For example, a wirelessly controllable bioresorbable electronic patch (BEP) was developed and implanted inside the surgical brain cavity for long-term drug delivery and tumor treatment [58]. The heater on the BEP was wirelessly actuated by an external magnetic field, promoting drug diffusion to deep brain regions (Fig. 1K). As a result, deeply infiltrated tumor cells were treated (Fig. 1L). Such actuation can be periodically conducted until the biodegradation of the heater, and subsequent drug delivery from the BEP is carried out via natural diffusion of the remaining drugs. Furthermore, a second surgery to remove the implanted device is not required, as the BEP is biodegradable. Owing to these advantages, BEP may show improved therapeutic efficacy in mouse/canine tumor models.
Go to :
REMAINING CHALLENGES AND FUTURE OUTLOOK
Although local drug delivery strategies have shown progress in GBM treatment, complete recovery from GBM remains a daunting goal. The major cause of GBM recurrence is the infiltration of tumor cells, and although several electronics-assisted strategies have attempted to counter this challenge, the penetration/diffusion depth of the drug into brain tissues is still limited. Other methods, such as CED, exhibit better delivery efficiency; however, liquid-state drugs dissipate rapidly and thus often result in low treatment efficiency. While the electronics-assisted drug delivery method can potentially deliver drugs to the deep brain region over a much longer period, both the drug penetration depth and delivery period should be further improved. Additionally, the biocompatibility and biodegradability of implantable devices should be considered.
Many practical issues must be resolved for clinical translation. For example, since each GBM case exhibits various characteristics owing to the highly pathological and genetic heterogeneity of GBM, the applicability of the platform device for a broad range of personalized therapeutic moieties and drugs should be guaranteed. Furthermore, the treatment efficacy should be verified in GBM models of large animals. At present, small animal models are mostly used, and a large animal model test is critical before human applications. Thus, the development of reliable GBM models in large animals is required. The biocompatibility of implantable platforms should also be systematically examined in a larger number of subjects. For clinical applications, additional protocols must be developed to increase friendliness of the patients and reduce the economic burden on patients. Utilizing new digital technologies, such as wearable and/or implantable bioelectronics connected to wireless networks, may provide new opportunities. Despite the many remaining challenges, there is potential for the development of novel treatment strategies to make a breakthrough in GBM treatment.
Go to :
 XML Download
XML Download