

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Viral antigens expressed within cancer cells have long been investigated as attractive immunological targets in regard to tumor-specific cancer immunotherapy, including cytotoxic T lymphocyte (CTL) or dendritic cell (DC)-based vaccines, because a viral antigen, as a non-self antigen, can elicit potent antitumor immunity in vivo and ex vivo, compared to tumor-associated antigens. Over the last two decades, numerous studies have investigated the presence of cytomegalovirus (CMV) within glioblastoma or gliomas; however, the results are severely conflicting. While a few researchers have suggested the potential benefits of CTL or DC vaccines for recurrent or newly diagnosed glioblastoma patients, several studies did not at all agree with the existence of CMV in glioblastoma cells [123456789101112]. In this context, we summarized the conflicting results and issues about the detection of CMV in glioblastoma or glioma patients. We also provided the clinical data of published and unpublished clinical trials using CMV-specific immunotherapy for glioblastomas.
Electronic databases, PubMed, Google Scholar, Directory of Open Access Journals, and Web of Science were searched from January 2022 to February 2022. Database searches included the following key words: ‘glioblastoma or glioma’ and ‘cytomegalovirus or CMV.’ Two researchers (CS and JA) extracted the relevant information and validated their inclusion in the current review.
HUMAN CMV AS A THERAPEUTIC TARGET FOR GLIOBLASTOMA TREATMENT?
Detection of human CMV in patient’s glioblastoma samples
The presence of human CMV in patients with malignant gliomas was first reported using the methods of immunohistochemistry (IHC) and in situ hybridization (ISH) by Cobbs et al. [13]. Since then, various methods have been utilized to detect human CMV from glioblastoma specimens. Mitchell et al. [14] was the first to detect CMV DNA using polymerase chain reaction (PCR), analyzing glioblastoma specimens and peripheral blood. Western blot, flow cytometry, and next-generation sequencing (NGS) also utilized. Among these methods, IHC is most frequently used to detect human CMV in glioblastoma samples. Based on several studies suggesting the relationship between human CMV and glioblastoma, consensus on the role of human CMV in glioblastoma was made in 2011 [15]. For high sensitivity in detection, a precise method involving cell culture, immunostaining, and RNA/protein extraction from glioblastoma tissue was also proposed by Cobbs et al. [16]. Nevertheless, results of recent studies are conflicting. Detailed results according to the detection method are described in Tables 1, 2, 3, 4.
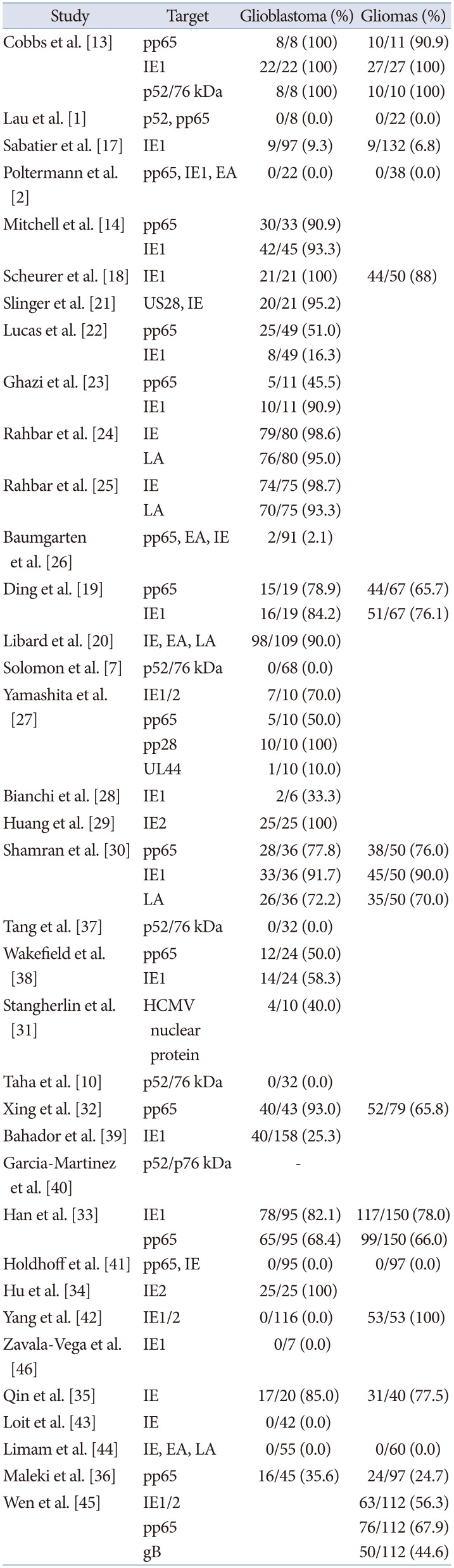
A total of 36 studies have evaluated the presence of proteins in paraffin sections of glioblastomas and/or gliomas using IHC methods and 23 studies suggested the presence of CMV proteins in patient’s specimens, while 13 studies did not demonstrate the presence of CMV proteins (Table 1) [127101314171819202122232425262728293031323334353637383940414243444546]. When using IHC, the median detection rates of CMV protein for gliomas or glioblastoma was 77.5% (range, 2.1% to 100%), and median detection rates for glioblastoma only was 90.5% (range, 2.1% to 100%). The detection rates of CMV proteins seemed higher in glioblastoma than in gliomas [13171819202930313233343536]. Immediate-early proteins (IEs) and phosphoprotein 65 (pp65) are popular targets when using IHC. Among the 36 total studies, 28 studies targeted IEs (17 studies targeted IE-1 specifically) and 16 studies targeted pp65.
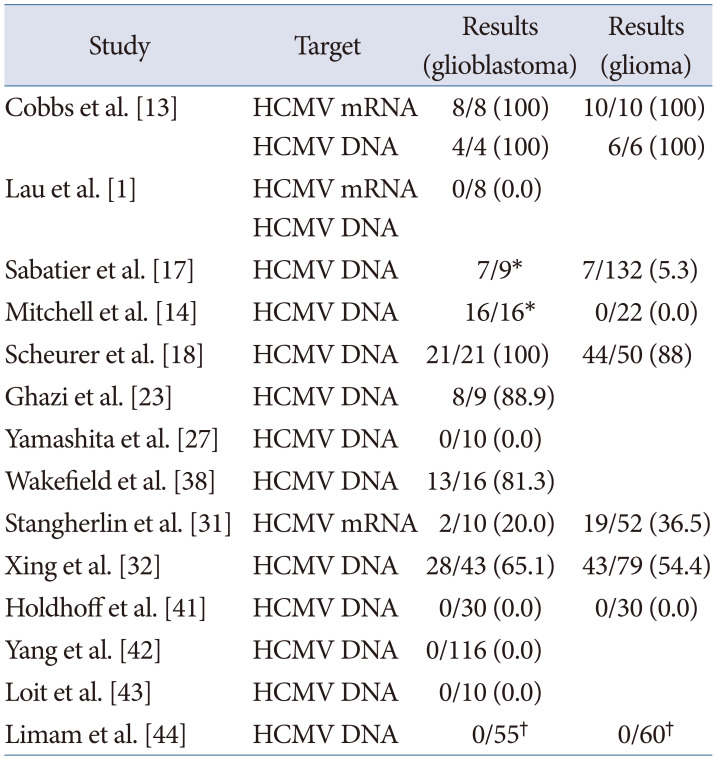
In addition, 14 studies utilized ISH to detect CMV DNA or mRNA in paraffin sections of glioblastoma and/or gliomas [113141718232731323841424344]. Seven studies showed positive results, while seven studies did not find CMV genomic products (Table 2). When using ISH, the median detection rate of CMV genomic products for gliomas or glioblastoma was 64.9% (range, 5.3% to 100%) [13171823313238].
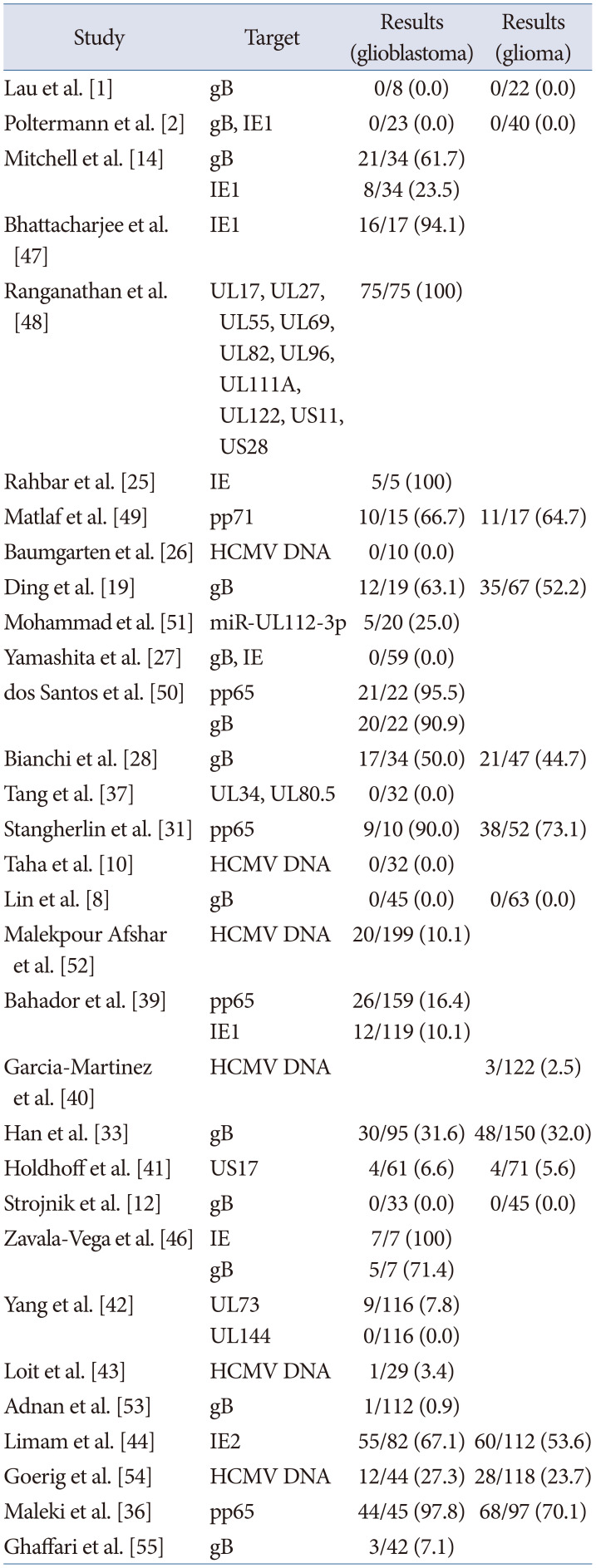
Thirty-one studies utilized PCR to detect CMV genes within tumors, and 16 studies showed positive results (range, 16.4% to 100%), while 15 studies failed to find CMV genome markers (Table 3) [12810121419252627283133363739404142434446474849505152535455]. Utilizing primers specific for the CMV glycoprotein B (gB) gene was the first attempt to detect CMV by PCR [1]. Primers of gB, IE, and pp65 were utilized in 15, 8, and 4 studies each, respectively.
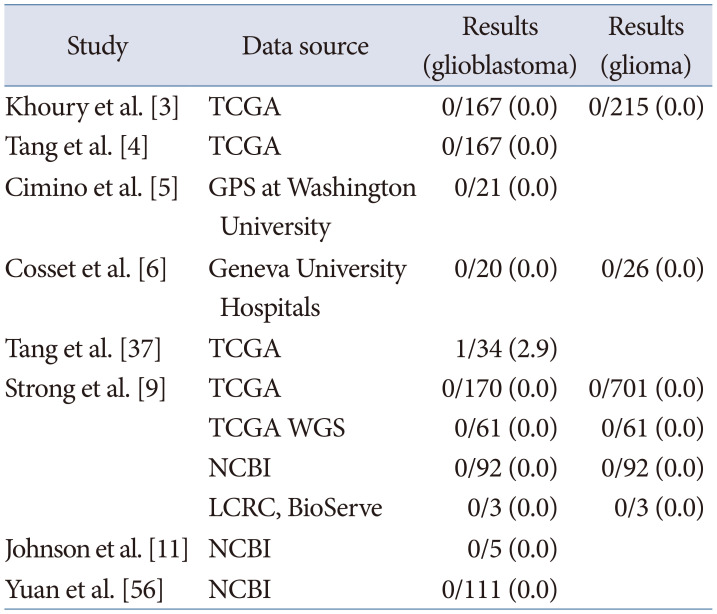
Researchers also utilized NGS to detect CMV genes within tumors based on their own samples, as well as public database. The most common data source is The Cancer Genome Atlas (TCGA) and National Center for Biotechnology Information (NCBI). Out of eight studies, four studies downloaded NGS datasets from the TCGA Cancer Genomics Hub repository (CGHub, now migrated to Genomic Data Commons; https://portal.gdc.cancer.gov) and three studies from NCBI Sequence Read Archive (SRA; https://www.ncbi.nlm.nih.gov/sra) or Gene Expression Omnibus (GEO; https://www.ncbi.nlm.nih.gov/geo/) (Table 4) [34569113756]. Unlike other methods, all studies using NGS failed to demonstrate the presence of CMV genes. There was only one positive case from a study, but it may be explained by the contamination of CMV protomer gene [37]. In summary, studies using, IHC, ISH, or PCR favored the presence of CMV in glioblastoma or gliomas, while studies using NGS method did not find the presence of CMV.
Controversy of detection results
The difference between studies may be explained by several reasons. First, CMV proteins and nucleotides could be readily detected if the entire protocol is optimized as suggested [1516]. In IHC, paraffin blocks of fresh brain autopsy specimens must be sectioned in 6 µm slices. Application of pepsin or trypsin at 37℃ for 4–6 min and of citrate at 85℃–90℃ for 2–4 min followed by washing in a 45℃–50℃ water bath for 2.5 hour should be performed carefully to avoid damage to viral antigens. Han et al. [33], following the methodology of Cobbs et al. [16], showed a high detection rate using IHC (82.1% and 68.4% in glioblastoma for IE-1 and pp65, respectively). In contrast, some studies utilizing thin formalin-fixed paraffin-embedded tissue sections (3–4 µm) or an automated immunostainer demonstrated low detection rates [364344]. Yang et al. [42] failed to detect IE protein in 116 samples using the methodology of Cobbs et al. [16]. The low detection limit of IHC, small sample size, and measurement error may explain the false negative results as well [26]. Second, the blood positivity of the CMV may also contribute to the detection results for human CMV. All eight studies showing the seropositive in patient’s blood, found the presence of CMV in tumors [1419233039464951].
Nevertheless, the results between studies are conflicting and not consistent according to detection methods, even within a single study. Further and larger studies to clarify this controversy are needed.
Onco-modulatory role of human CMV in glioblastomas
Over the past several decades, several viruses have turned out to elicit oncogenesis. Including human papillomavirus that causes cervical cancer and hepatitis C virus that causes liver cancer, oncogenic viruses are responsible for 10% to 15% of human cancers [57]. These viruses directly affect healthy cells and cause cancer transformation through spreading its nucleic acids. Meanwhile, other viruses, including human CMV, are known to cause cancer in a more indirect manner, which is known as onco-modulatory effect. In other words, human CMV infection, unlike oncovirus, is known to enhance malignancy via formation of tumor-related microenvironment [58].
Human CMV has recently been suggested to have a onco-modulatory role in several brain malignancies including glioma, medulloblastoma, and neuroblastoma [5960]. Onco-modulatory effects are defined as contributing to increase the extent of malignancy. In detail, human CMV infection induced the cells to be more vulnerable to carcinogenic materials due to lack of adhesion molecules in neurons, which are more aggravated when CMV re-activation occurred more frequently [5860]. In addition, human CMV-infected glioma cells showed stem-like characteristics with increased IE protein expression [34394561]. Several studies suggest specific onco-modulatory roles of CMV-infected glioma. These roles include self-sufficiency in growth signals, insensitivity to anti-growth signals, evasion of apoptosis, limitless replicative potential, sustained angiogenesis, tissue invasion and metastasis, deregulation of cellular energetics, avoiding immune destruction, tumor-promoting inflammation, and genome instability and mutation [5859].
CLINICAL TRIALS OF CMV-SPECIFIC IMMUNOTHERAPY for GLIOBLASTOMA PATIENTS
Published clinical trials
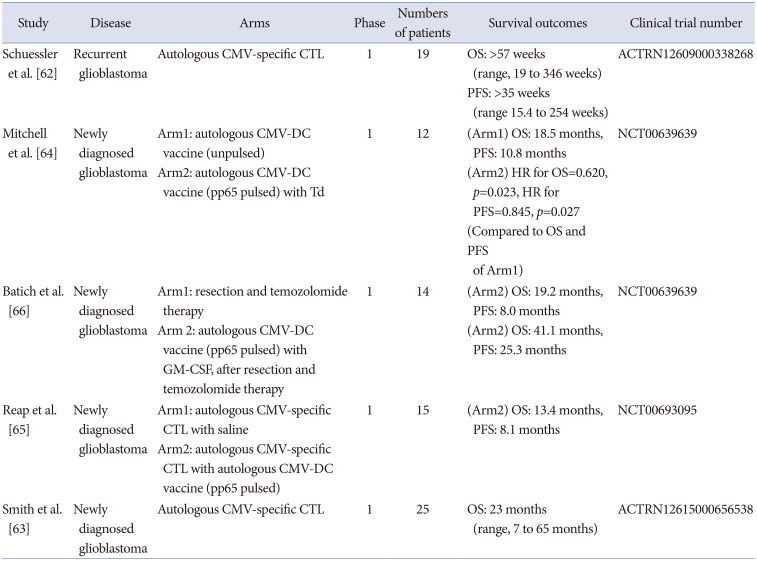
Until now, CMV-specific immunotherapy mainly includes autologous CMV-specific CTL or DC-based therapeutic vaccines. The first study using autologous CMV-specific CTL for recurrent glioblastoma was published in 2014 [62]. Autologous CMV-specific CTL generated by synthetic peptide epitope stimulation ex vivo was administered for 13 recurrent glioblastoma patients without severe adverse toxicities. The clinical outcomes suggested a substantially increased median survival (overall survival more than 57 weeks), compared to that of historical glioblastoma patients. Another study published in 2020 using autologous CTL for newly diagnosed glioblastoma showed the clinical experiences of 25 patients treated with CTL [63]. The group that received CTL before progression demonstrated longer overall survival (23 versus 14 months) than those who received CTL after progression.
Three studies reported the clinical outcomes of autologous CMV-specific DC-based vaccines for newly diagnosed glioblastoma patients. The first study, using a CMV-DC vaccine published in 2015, included 12 patients with newly diagnosed glioblastoma. The study showed better overall survival and progression-free survival (with hazard ratios of 0.620 in overall survival) [64]. Also, in the group treated with pp65-pulsed DC vaccine with tetanus and diphtheria toxoid (Td), increasing migration of DC toward lymph node was found than in a group treated with an unpulsed DC vaccine. A second study published in 2018 included 15 patients with newly diagnosed glioblastoma who received an autologous CMV-specific CTL and pp65 pulsed CMV-DC vaccine [65]. Patients treated with CTL therapy followed by CMV-DC vaccine showed better overall survival and progression free survival (13.4 month overall survival and 8.1 month progression-free survival after recurrence). These two studies suggested that the pp65-specific DC vaccine was associated with increased CMV-specific T cell frequency as well as survival outcomes, when combined with Td toxin or autologous CTL. Another study using a CMV-specific DC vaccine combined with the standard of care including concomitant chemoradiation followed by dose-intensified temozolomide, enrolled 14 patients with newly diagnosed glioblastoma [66]. When the patients were treated with pp65-specific DC vaccine with granulocyte macrophage-colony stimulating factor (GM-CSF) after temozolomide, the median overall survival was 41.1 months and progression-free survival 25.3 months. Table 5 summarizes the published results of clinical trials of CMV-specific immunotherapy for glioblastoma [6263646566].
Unpublished clinical trials
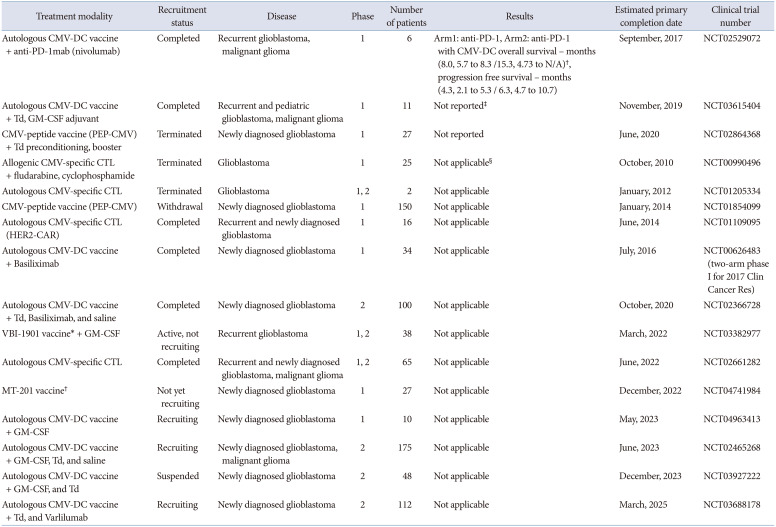
Unpublished clinical trials of CMV-specific immunotherapy include various combinational strategies. In detail, among four clinical trials using CMV-specific CTL therapy (NCT00990496, NCT01205334, NCT01109095, NCT02661282), one recent trial applied CMV-specific CTL with an engineered HER-2 chimeric antigen receptor (NCT01109095). Clinical trials using CMV-specific DC-based vaccines with various adjuvants such as GM-CSF (NCT04963413), Td toxin (NCT03615404, NCT02465268, NCT03927222), or cancer drugs including IL-2 receptor antagonist (NCT00626483, NCT02366728), anti-CD27 antibody (NCT03688178), and anti-PD-1 inhibitor (NCT02529072) are currently being investigated. Another type of CMV-specific vaccine including enveloped virus-like particle vaccine (VBI-1901), or pp65-specific monocyte vaccine are also being investigated (NCT03382977, NCT04741984). The summary of unpublished clinical trials of CMV-specific immunotherapy for glioblastoma is contained in Table 6.
CONCLUSION
As one of the novel immunotherapeutic strategies, clinical approaches using CMV-specific CTL and/or DC-vaccines have been tested. However, there are some limitations of previous studies. First, numerous studies have tried to evaluate the presence of CMV within glioblastoma; however, consolidative results for the presence of CMV within glioblastoma are needed. Second, the onco-modulatory role of CMV for gliomagenesis is unknown. Third, clinical trials have suggested positive clinical outcomes, but additional larger and randomized studies are needed. As viral antigens can elicit one of the most powerful immune repones, the presence of viral antigens within tumor cells can be an attractive immuno-therapeutic target for various cancer types. Therefore, further translational studies are needed to support the presence of CMV and the onco-modulatory role in gliomagenesis.
 XML Download
XML Download