

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intracranial extraskeletal myxoid chondrosarcoma (EMC) is an extremely rare disease, with only 13 cases reported since its first description in 1972 [12345678910111213]. However, due to lack of precise diagnostic criteria and histologic/genetic evidence of previously reported cases, it is uncertain if all reported cases are true intracranial EMC [14]. We hereby present a new case of intracranial EMC in fourth ventricle. We reviewed previously reported cases of intracranial EMCs to validate their diagnosis and to find out if there are clinical similarities among them.
Go to : 
CASE REPORT
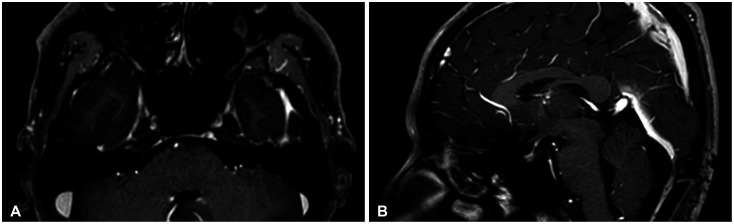
A 36-year-old male presented with 2 weeks of dizziness. MRI of the brain showed approximately 1.6 cm sized intraventricular tumor of fourth ventricle. The tumor showed low signal intensity on T1, high signal intensity on T2-weighted image and showed homogenous enhancement on contrast enhanced T1-weighted image (Fig. 1). Initial impression of diagnosis was hemangioblastoma, but preoperative angiography did not show any staining of the tumor. The tumor was approached with midline suboccipital craniotomy and telovelar approach. The tumor was attached to the choroid plexus of the rhomboid fossa; there was no other attachment to adjacent structures. The tumor was completely removed en bloc (Fig. 2). The whole operation was done under MRI navigation guidance and facial motor evoked potential monitoring.
 | Fig. 1Preoperative MRI of the patient. A: T1-weighted enhanced axial image. B: T2-weighted axial image. C: T1-weighted enhanced sagittal image. D: T2-weighted sagittal image. The tumor shows strong homogenous contrast enhancement on T1-weighted enhanced images and moderate to high signal on T2-weighted images.
|
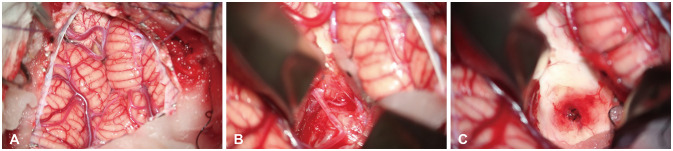 | Fig. 2Microscopic images of tumor. The tumor was removed via telovelar approach. A: Cerebellum is exposed after dura incision. B: Tela choroidea is exposed after retraction of right cerebelar tonsil and vermis. C: The tumor attached to the choroid plexus and the fourth ventricle floor is removed en bloc.
|
Microscopic examination of the specimen showed spindle shaped cells with scant eosinophilic cytoplasm on basis of abundant myxoid stroma. Overall pathologic morphology resembled that of a mesenchymal tumor (Fig. 3). Immunohistochemistry (IHC) staining results showed negative in glial markers isocitrate dehydrogenase 1 and glial fibrillary acidic protein (GFAP). Final pathology report was EMC. Immediate postoperative MRI showed no remnant enhancing lesion suggesting complete removal of tumor. The patient recovered well without any significant neurologic deficit, except mild dysphagia and hypesthesia of left thigh. Adjuvant radiotherapy (54 Gy/27 fx) started at 1 month postoperatively, and MRI followed at 3 months after surgery showed no recurrence of tumor (Fig. 4). Patient remained free of any neurologic deficit.
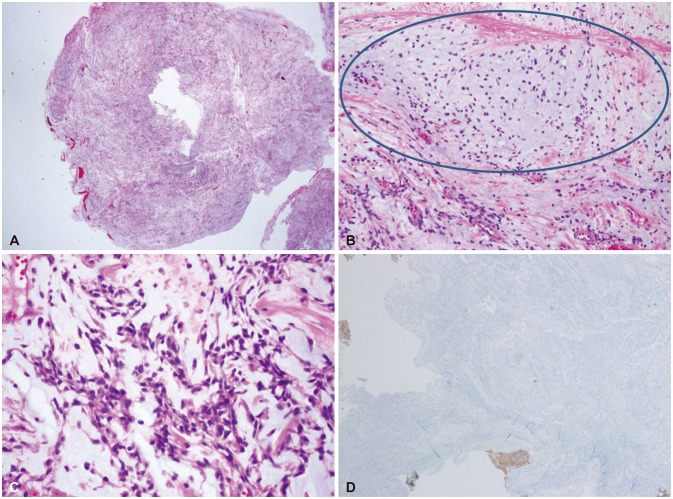 | Fig. 3Pathologic findings. A: Low power view (H&E stain, ×12.5) shows a somewhat well demarcated mass. B: In the mass, myxoid stroma (oval circle) is noted (H&E stain, ×200). C: High power view (H&E stain, ×400) shows haphazardly arranged spindle cells with myxoid stroma. D: The GFAP immunohistochemistry shows negative reaction (GFAP stain, ×400). These findings are compatible with extraskeletal myxoid chondrosarcoma. H&E, hematoxylin and eosin; GFAP, glial fibrillary acidic protein.
|
Go to :
DISCUSSION
Intracranial chondrosarcoma is a very rare disease entity, with a portion of 0.16%–0.5% of all intracranial neoplasms [1415]. It is categorized into three subtypes: classic (conventional), mesenchymal, and myxoid [16]. Of all, intracranial EMC is the rarest, with only 13 cases reported up to date (Table 1).
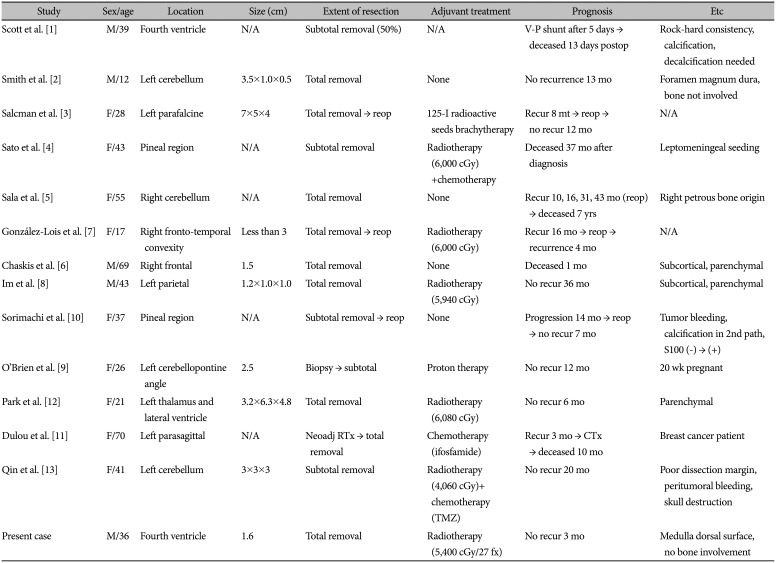
Table 1
Clinical characteristics of previously reported cases of intracranial myxoid chondrosarcomas
| Study | Sex/age | Location | Size (cm) | Extent of resection | Adjuvant treatment | Prognosis | Etc |
|---|---|---|---|---|---|---|---|
| Scott et al. [1] | M/39 | Fourth ventricle | N/A | Subtotal removal (50%) | N/A | V-P shunt after 5 days → deceased 13 days postop | Rock-hard consistency, calcification, decalcification needed |
| Smith et al. [2] | M/12 | Left cerebellum | 3.5×1.0×0.5 | Total removal | None | No recurrence 13 mo | Foramen magnum dura, bone not involved |
| Salcman et al. [3] | F/28 | Left parafalcine | 7×5×4 | Total removal → reop | 125-I radioactive seeds brachytherapy | Recur 8 mt → reop → no recur 12 mo | N/A |
| Sato et al. [4] | F/43 | Pineal region | N/A | Subtotal removal | Radiotherapy (6,000 cGy)+chemotherapy | Deceased 37 mo after diagnosis | Leptomeningeal seeding |
| Sala et al. [5] | F/55 | Right cerebellum | N/A | Total removal | None | Recur 10, 16, 31, 43 mo (reop) → deceased 7 yrs | Right petrous bone origin |
| González-Lois et al. [7] | F/17 | Right fronto-temporal convexity | Less than 3 | Total removal → reop | Radiotherapy (6,000 cGy) | Recur 16 mo → reop → recurrence 4 mo | N/A |
| Chaskis et al. [6] | M/69 | Right frontal | 1.5 | Total removal | None | Deceased 1 mo | Subcortical, parenchymal |
| Im et al. [8] | M/43 | Left parietal | 1.2×1.0×1.0 | Total removal | Radiotherapy (5,940 cGy) | No recur 36 mo | Subcortical, parenchymal |
| Sorimachi et al. [10] | F/37 | Pineal region | N/A | Subtotal removal → reop | None | Progression 14 mo → reop → no recur 7 mo | Tumor bleeding, calcification in 2nd path, S100 (−) → (+) |
| O'Brien et al. [9] | F/26 | Left cerebellopontine angle | 2.5 | Biopsy → subtotal | Proton therapy | No recur 12 mo | 20 wk pregnant |
| Park et al. [12] | F/21 | Left thalamus and lateral ventricle | 3.2×6.3×4.8 | Total removal | Radiotherapy (6,080 cGy) | No recur 6 mo | Parenchymal |
| Dulou et al. [11] | F/70 | Left parasagittal | N/A | Neoadj RTx → total removal | Chemotherapy (ifosfamide) | Recur 3 mo → CTx → deceased 10 mo | Breast cancer patient |
| Qin et al. [13] | F/41 | Left cerebellum | 3×3×3 | Subtotal removal | Radiotherapy (4,060 cGy)+chemotherapy (TMZ) | No recur 20 mo | Poor dissection margin, peritumoral bleeding, skull destruction |
| Present case | M/36 | Fourth ventricle | 1.6 | Total removal | Radiotherapy (5,400 cGy/27 fx) | No recur 3 mo | Medulla dorsal surface, no bone involvement |
![]()
EMC shows heterogenous histological morphology. Common findings of the reported cases include lobulated basophilic myxoid stroma with short spindle cells or small round cells. Cells consist of small, hyperchromatic nuclei with scant, eosinophilic cytoplasm. Mitoses counts are usually rare, and most of the reported cases showed no intra-tumoral bleeding or necrosis, suggestive of the relatively indolent nature of the tumor. Intraoperative findings of the reported cases vary; in most of the reports the tumor is described as a gray or brownish, well circumscribed, soft round mass without calcification.
IHC results are crucial in differentiating EMCs from other EMC-mimicking intracranial tumors. S100 staining shows diffuse, strong positivity in most of EMCs while only focal moderate staining in 40% of chordoid meningiomas. Pankeratin staining can be used to differentiate between chordoid gliomas and chordomas from EMCs. Epithelial membrane antigen staining shows positive in most cases of chordoid gliomas, chordomas, and chordoid meningiomas while only 25% of EMCs show positivity. GFAP staining is used to differentiate EMCs from gliomas like pilocytic astrocytoma [17]. Of 13 case reports, 10 studies had at least one IHC result reported. The results are described in Table 2. Neuronal markers such as GFAP, neuron-specific enolase, synaptophysin all showed negative, while vimentin was positive in all tested patients, and most of the patients showed negative in cytokeratin and EMA staining. These results are largely congruent with previous studies of extracranial EMCs, providing validity to their diagnosis [18].
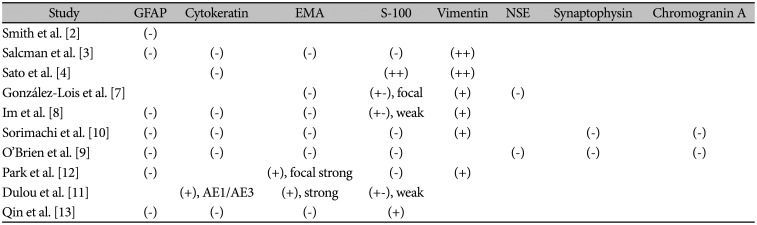
Table 2
Immunohistochemistry results of previously reported cases of intracranial myxoid chondrosarcomas
| Study | GFAP | Cytokeratin | EMA | S-100 | Vimentin | NSE | Synaptophysin | Chromogranin A |
|---|---|---|---|---|---|---|---|---|
| Smith et al. [2] | (−) | |||||||
| Salcman et al. [3] | (−) | (−) | (−) | (−) | (++) | |||
| Sato et al. [4] | (−) | (++) | (++) | |||||
| González-Lois et al. [7] | (−) | (+−), focal | (+) | (−) | ||||
| Im et al. [8] | (−) | (−) | (−) | (+−), weak | (+) | |||
| Sorimachi et al. [10] | (−) | (−) | (−) | (−) | (+) | (−) | (−) | |
| O'Brien et al. [9] | (−) | (−) | (−) | (−) | (−) | (−) | (−) | |
| Park et al. [12] | (−) | (+), focal strong | (−) | (+) | ||||
| Dulou et al. [11] | (+), AE1/AE3 | (+), strong | (+−), weak | |||||
| Qin et al. [13] | (−) | (−) | (−) | (+) |
![]()
Of 13 cases previously reported, two cases were questionable of their validity of diagnosis. The first case report of 1976 [1] reported the tumor had a ‘rock-hard’ consistency and ‘had to be attacked with... rongeurs and scissors’. Pre-op X-ray image showed prominent calcification of the tumor. Tumor specimen had to be decalcified before microscopic observation, which showed presence of osteoid tissue. No other case reported prominent calcification or presence of osteoid tissue. The tumor was more likely a mixed sarcoma with prominent osteoid formation as suggested in another case report [2]. Another case from Poland presented a known triple negative breast cancer patient diagnosed with parenchymal brain tumor of left frontal lobe [11]. Although the authors confirmed the histological diagnosis as myxoid chondrosarcoma, the report did not present any suitable IHC results to claim so. According to the report, the specimen showed strong staining in EMA and cytokeratin; no results regarding vimentin or GFAP were presented. EMA and cytokeratin are known to show positivity mostly in epithelial origin tumor and these findings do not match with other previously reported cases of EMCs. Chordoid meningioma can be a considerable diagnosis, considering its EMA positivity. But the tumor seems intraaxial in given MRI image, and the pathology report also claims infiltration of tumor into brain parenchyma. Considering the patient's medical history, the lesion could be a metastatic adenocarcinoma with myxoid stromal change [19] or a metastatic mucinous breast lesion mimicking myxoid stroma [20].
Because of the rarity of the disease, there is no solid theory or evidence regarding how a chondrosarcoma can primarily form inside a cranium. Intracranial chondrosarcomas are supposed to originate from embryonic rests of the chondrocranium or from metaplasia of meningeal fibroblasts and typically arise from the base of the skull [21]. Previous case reports presented choroid plexus, remaining multipotent mesenchymal cells of skull base or dura mater as possible origins of the tumor. To our knowledge, this case is the second intraventricular EMC reported [12] and first EMC to be histologically confirmed with IHC results that formed inside fourth ventricle.
Optimal treatment of EMCs is still debated. In most of the cases the tumor was separated well from surrounding tissue. In 9 out of 14 cases, including present case, the tumor was totally removed by surgery. However, it is unclear if the extent of removal is associated with lower recurrence or better prognosis. Three cases reported recurrence of tumor after total removal. Adjuvant therapy also varied widely. A recent phase II trial of pazopanib in advanced EMCs showed anti-tumor activity, but it is even more difficult to treat intracranial EMCs because central nervous system permeability needs to be considered [22]. Five cases have undergone adjuvant radiotherapy, of which two with concurrent chemotherapy. Further studies need to be done regarding necessity and efficacy of adjuvant treatment.
In conclusion, we present a rare case of intracranial EMC originated from the choroid plexus inside fourth ventricle. IHC staining results are crucial in differential diagnosis of intracranial EMCs from other intracranial tumors mimicking its pathologic morphology. Optimal treatment of the disease is still debated; more cases and further studies are needed regarding the necessity of radical excision, adjuvant chemotherapy and radiotherapy.
Go to :
 XML Download
XML Download