

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meningioma management options include regular monitoring especially for incidental tumours, symptom control, surgical excision, external beam radiotherapy (EBRT) and occasionally chemotherapy but, tailored maximal resection remains the treatment of choice. Further optimal management is difficult to establish as the role of post-operative radiotherapy (RT) remains controversial apart for malignant meningiomas [123].
Despite a generally indolent course, outcome of meningioma patients may be poor due to an aggressive behaviour of the tumour, not solely related to a malignant histopathology. Those requiring reoperation or EBRT often have reduced survival.
Confining the radiation to the planning target volume with minimum spillage of dose outside is critical. Protontherapy (PT) possesses singular physical properties that allow dose distribution with a relatively constant energy deposition with a sharp drop-off up to the distal edge of the tumour (Bragg peak). This may therefore decrease the given dose to the healthy surrounding tissues compared to standard RT by photon. In recent years, more facilities have been delivering PT which is now available in three centres in France with the recent opening of the Caen hadrontherapy centre (2018) beside Nice (1991, upgraded in 2016) and Orsay near Paris (1991, upgraded in 2010).
Administrative medical databases (AMDB) are massive repositories of collected healthcare data for various purposes with a constant and often on-going collection process [4]. They often encompass very large population and frequently the whole nation, ensuring high statistical power without biases related to the representativity of a sample. They can be used to conduct epidemiological studies and evaluate medical practices [5]. In that respect, the French nationwide health record database Système National des Données de Santé (SNDS) recently opened to researchers is a great opportunity to carry out comprehensive health studies at the country level [5].
Around 3,000 patients are operated on for a meningioma each year in France but only a small fraction have also been treated by PT usually for aggressive meningioma. The objective of this study was to describe and evaluate the survival of patients who received PT after meningioma surgery and search for associated prognostic factors.
Go to : 
MATERIALS AND METHODS
We performed a cross-sectional nationwide population-based descriptive observational and analytic retrospective study. Incidental meningiomas never operated were not considered in this study; only surgically treated tumours were taken into account. Data were extracted from the SNDS, the national French medico-administrative database. Patients who underwent the surgical resection of a meningioma between the first of January 2008 and the 31 December 2017 were included. Cases were selected using an algorithm combining two variables as described previously: the type of the surgical procedure identified by the Common Classification of Medical Acts (CCAM) and the primary diagnosis according to the International Classification of Diseases (ICD-10) [6789]. Benign meningiomas were considered as corresponding to the D32 ICD-10 code, atypical to D42 and malignant to C70. Meningioma were categorised into 8 anatomical locations according their dura mater insertion after categorisation of the 40 CCAM codes which aimed at precisely described intracranial extracerebral tumour resection. Patients below 18 years were not included in this study (n=118). We defined the first recorded date of meningioma surgery as the index date. The Mortality-Related Morbidity Index (MRMI) predictive of all-cause mortality and the Expenditure-Related Morbidity Index (ERMI) predictive of health care expenditure were used to assess the global health-state severity [10]. Progression was defined as any new treatment for meningioma recurrence e.g., redo PT and redo surgery, RT or stereotactic radiosurgery (SRS) given after the PT.
Statistical methods
For the description of the cohort presented in Table 1, continuous variables are summarised as means and standard deviations or as medians and interquartile ranges (IQR) for non-Gaussian distributed variables. Categorical variables are reported as frequencies and proportions. Because death is the most untoward event, mortality was the primary outcome of interest. Overall survival (OS) was measured from the date at meningioma first surgery to the date of last follow-up or death. Progression-free survival (PFS) was measured from the date at first meningioma PT to the date of any new treatment for recurrence, death or last follow-up. We used the Kaplan-Meier method to estimate the OS and the Mantel Cox log-rank test was used to compare survival curves. Cox proportional hazards regression modelling was implemented to identify predictors of death or recurrence and, to estimate hazard ratio (HR) with 95% confidence intervals (CI). Follow-up time was calculated by the reverse Kaplan-Meier estimator method. In essence, there is no lost to follow-up patient in the SNDS; those who died are automatically registered as such in the database. All tests were 2-sided and statistical significance was defined with an alpha level of 0.05 (p<0.05). Analysis was performed with both the SAS Enterprise guide version 7.15 (SAS Institute Inc., Cary, NC, USA), the R programming language and software environment for statistical computing and graphics (R version 4.0.4 [2021-02-15]; R Core Team, R Foundation for Statistical Computing, Vienna, Austria) and the survival package among others. The statistical programme and workflow was written in R Markdown v2 with RStudio for dynamic and reproducible research.
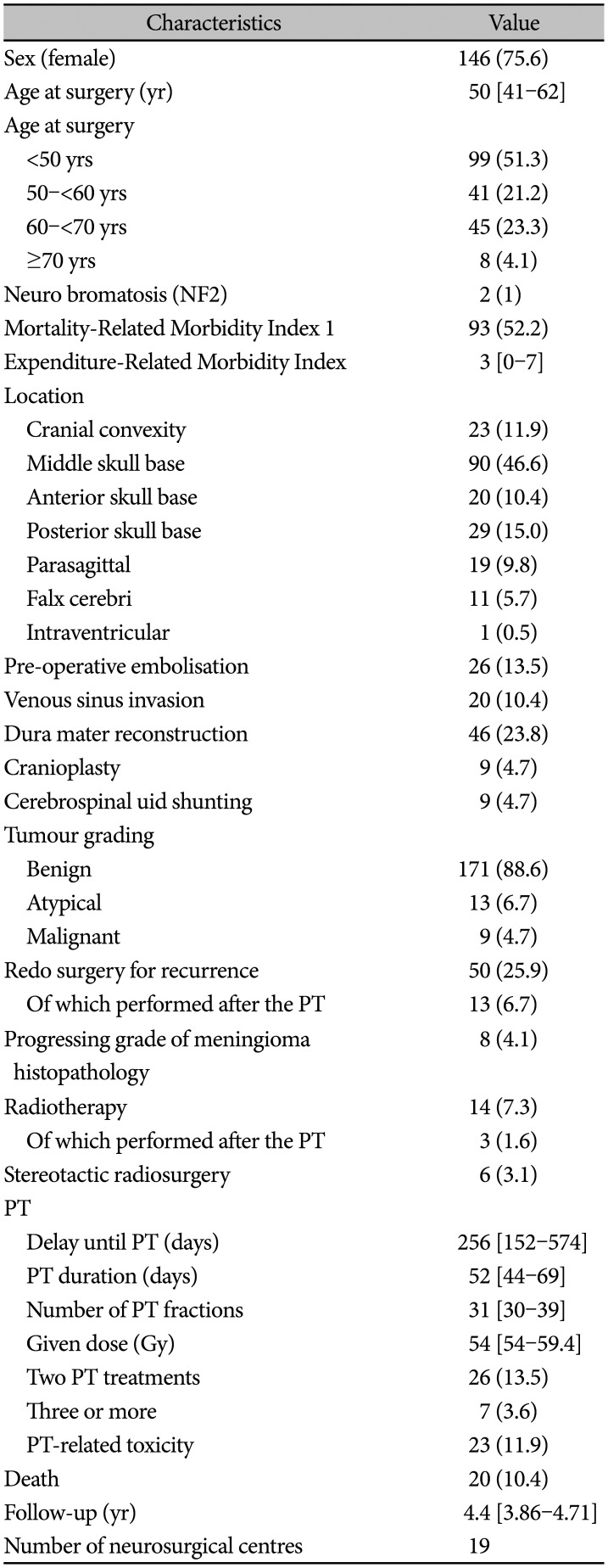
Table 1
Characteristics of the 193 patients who received PT
![]()
Go to :
RESULTS
Population description
Over a 10-year period, 193 patients (0.67%) who received PT were extracted from a nationwide population-based cohort of 28,924 meningioma patients. Of the 193 patients, 75.6% were female. Median age at surgery was 50 years (IQR 41–62). According the MRMI, male had significantly more co-morbidities compared to female (p=0.001). The level of co-morbidity also increased with the age (p=0.026). Most meningiomas (72%) were located on the skull base with the middle skull base being the most frequent location (46.6%) followed by the posterior skull base (15%). Benign meningioma represented 88.6%, atypical 6.7%, and malignant 4.7%. Median follow-up was 4.4 years (IQR 3.86–4.71) (Table 1). Median delay between meningioma surgery and PT was 256 days (IQR 152–574). The median number of PT fractions was 31 (IQR 30–39) given over a median duration of 52 days (IQR 44–69). Thirty-three patients (17.1%) had several PT treatments of which 26 patients (13.5%) two PTs and 7 patients (3.6%) three or four treatments. The median time between the first and the second PT was 2.6 years (IQR 1.8–3.5). If we considered solely the first PT treatment, the median number of fractions was 30 (IQR 30–33) given over a median time of 50 days (IQR 44–57). Fourteen patients (7.3%) also received standard RT and six patients (3.1%) SRS. A number of fraction above 33 (60 Gy) was not associated with an increase PT-related toxicity (p=0.723) neither was an associated standard RT, SRS included (p=0.123).
Progression-free survival
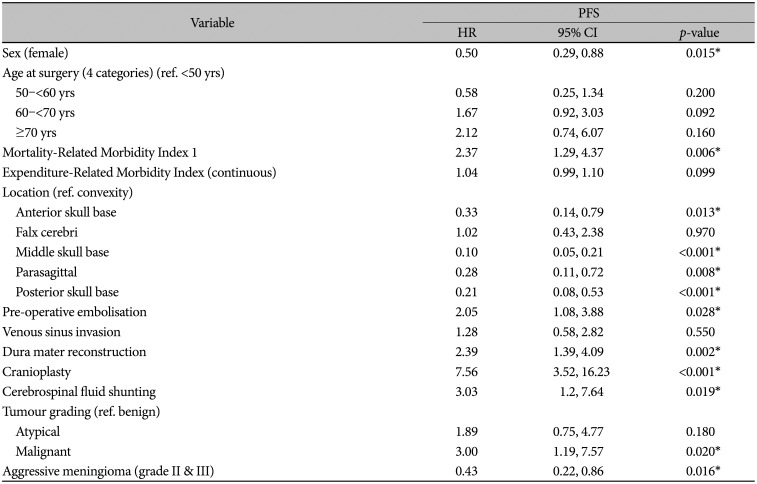
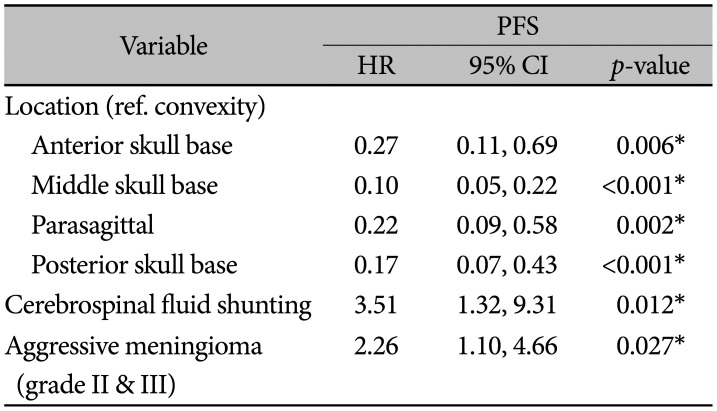
At data collection, 56 patients (29%) had relapsed. Median time until recurrence was 0.6 years (IQR 0.4–1.4). All grades considered, PFS rates at 5 and 10 years were: 69% (95% CI 62.1–76.6) and 64.4% (95% CI 55.8–74.2) (Fig. 1). For benign, atypical, and malignant meningioma, 5-year PFS were 71.5% (95% CI 64.4–79.4), 55.6% (95% CI 32.5–95), and 35.6% (95% CI 12.8–98.9), respectively (p<0.01). In univariable Cox regression, many variables were associated to the PFS (Table 2). In the adjusted regression, tumour location (HR=0.1, 95% CI 0.05–0.22, p<0.001), aggressive meningioma (HR=2.26, 95% CI 1.1–4.66, p=0.027), and the need of cerebrospinal fluid (CSF) insertion for hydrocephalus (HR=3.51, 95% CI 1.32–9.31, p=0.012) remained significantly associated to the PFS (Table 3).
 | Fig. 1Kaplan-Meier of PFS curves of entire patients (A) and according to sex (B), location (C), MRMI (D), grade (E), and CSF shunting (F). PFS, progression-free survival; MRMI, Mortality-Related Morbidity Index; CSF, cerebrospinal fluid.
|
Table 2
Univariable Cox regression of PFS after meningioma surgery and protontherapy
![]()
Table 3
Multivariable Cox regression of PFS after meningioma surgery and protontherapy
![]()
Overall survival
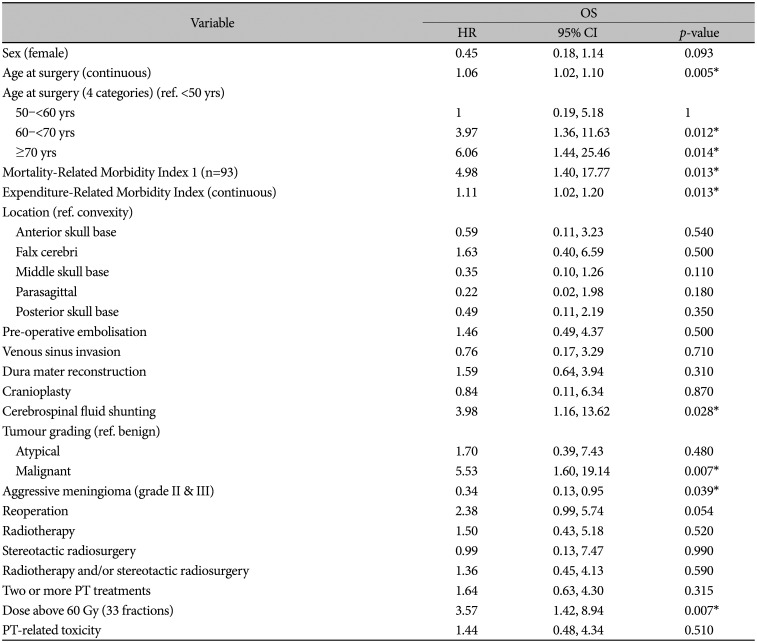
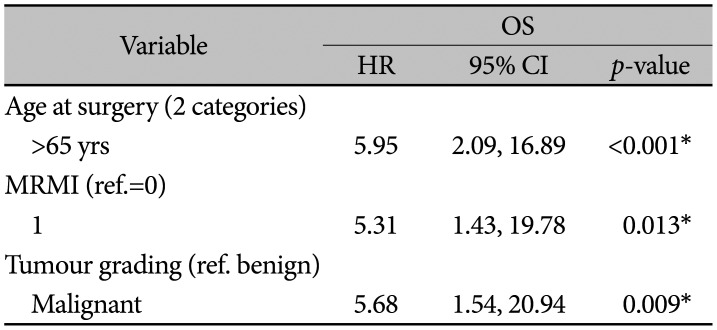
At data collection, 20 patients (10.4%) were dead. Median age at death was 66.5 years (IQR 53.9–73.8). All grades considered, OS rates at 5 and 10 years were: 89.7% (95% CI 84.6–95.1) and 80.8% (95% CI 72.4–90.2). For benign, atypical, and malignant meningioma, 5-year OS rates were 93% (95% CI 88.7–97.4), 76.4% (95% CI 51.4–100), and 44.4% (95% CI 16.7–100), respectively (p<0.01) (Fig. 2). In univariable Cox modelling, age at surgery (HR=1.06, 95% CI 1.02–1.1, p=0.005), MRMI (HR=4.98, 95% CI 1.40–17.77, p=0.013), ERMI (HR=1.11, 95% CI 1.02–1.2, p=0.013), CSF shunt insertion for associated hydrocephalus (HR=3.98, 95% CI 1.16–13.62, p=0.028), and malignant meningioma (HR=5.53, 95% CI 1.6–19.14, p=0.007) were associated to a shorter OS (Table 4). In the adjusted regression, an older age above 65 years (HR=5.95, 95% CI 2.09–16.89, p<0.001) with a high level of co-morbidities (HR=5.31, 95% CI 1.43–19.78, p=0.013) and a malignant meningioma (HR=5.68, 95% CI 1.54–20.94, p=0.009) remained significantly associated to a reduced OS (Table 5).
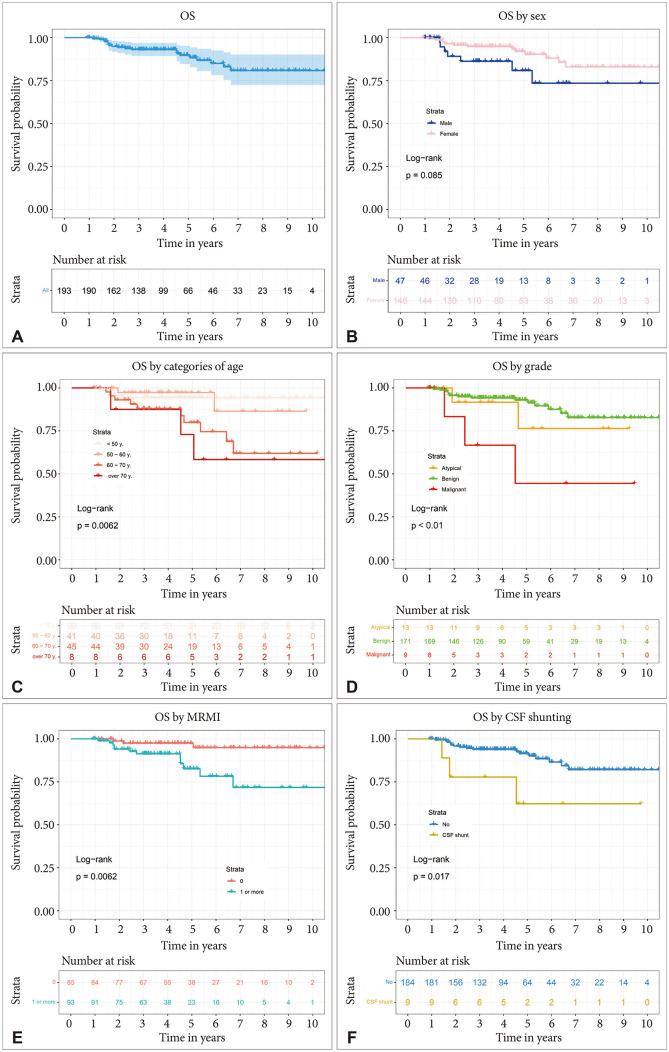 | Fig. 2Kaplan-Meier of OS curves of entire patients (A) and according to sex (B), categories of age (C), grade (D), MRMI (E), and CSF shunting (F). OS, overall survival; MRMI, Mortality-Related Morbidity Index; CSF, cerebrospinal fluid.
|
Table 4
Univariable Cox regression of OS after meningioma surgery and PT
![]()
Go to :
DISCUSSION
In this study, we evaluated PFS and OS after meningioma surgery and PT using the French health insurance national database SNDS.
Strengths and limitations
The strengths of the SNDS reside both in high number of patients and in exhaustive data available from every hospital in France. The database representativeness is nearly perfect, since it includes the whole country's population of nearly 68 million of inhabitants constituting one of the largest AMDB in the world [5]. Compiled from a number of institutions, its accuracy is nonetheless limited by inconstancies in data collection and recording. Moreover, important variables such as the quality of resection are not recorded in the SNDS [13]. Despite some limitations, the SNDS is an invaluable tool to assess meningioma outcome. It offers an incomparable means to explore associations with other pathology, medication or combine surgical treatment which has and could not be assessed before. The retrospective nature of this study, together with the lack of clarity regarding treatment rationales and non-homogeneous management strategies without random assignment, needs to be considered when evaluating the results.
EBRT for meningioma
With the emergence of modern irradiation techniques such as intensity-modulated radiation therapy (IMRT) or volumetric-modulated arc therapy (VMAT), the role of EBRT has significantly increased even as primary therapy for deep-situated meningiomas of which complete resection without permanent deficit is often difficult to achieve. As such, most meningiomas (72%) of our series are located on the skull base with middle skull base being the most common location (46.6%) vs. only 11.9% of cranial convexity meningiomas; the most common that usually constitutes around one quarter of all meningiomas [9]. This over-representation of skull base tumours may be a selection bias in the present cohort. Critically radiosensitive structures such as the optic tract or the hippocampus surrounding skull base meningiomas may be better spared by PT [14]. In general, for hardly-fully resectable meningiomas, most neurosurgeons prefer a safe cerebral decompression keeping the patient in a functional state and leave the tumour remnant for EBRT in case of progression.
In Kaur et al. [15] systematic review, 5-year OS after adjuvant EBRT for malignant meningioma was 55.6% with reported rates ranging from 27% to 80.8%. However, they noted that the prognostic impact of EBRT could not reliably be assessed given the lack of non-irradiated control groups [15]. Indeed, no randomised trial on RT after malignant meningioma surgery has been or will likely be undertaken, mainly due to the rarity of these tumours representing less than 3% of meningioma. Nonetheless, reported results suggest that malignant meningioma patients live longer after adjuvant EBRT [16]. Likewise, Kaur et al. [15] noted that no study was able to demonstrate a statistically significant improvement in any of the clinical outcomes with adjuvant EBRT for WHO grade II meningioma. RT after surgical resection of atypical meningioma remains thus controversial. Most neurosurgeons as we do, would not recommend systematic adjuvant RT for atypical meningioma, especially after total resection, preferring a wait and see policy and keeping EBRT in case of recurrence or residual progression. Ongoing clinical trials on EBRT for atypical meningioma such as the NRG-BN003 and the ROAM may clarify this controversy [17].
Several studies have found that higher radiation dose (≥52 Gy) correspond with better outcomes especially for aggressive meningiomas [1518]. In principle, PT offers a substantial clinical advantage over conventional RT. In contrast to photons, when protons penetrate matter, they slow down continuously as a function of depth. The rate of their energy loss increases with decreasing velocity. This process of dose deposition produces a characteristic depth-dose curve for a broad monoenergetic beam of protons. The point of highest dose is called the Bragg peak and dose deposited beyond the range is negligible. This unique depth-dose characteristic of protons can be exploited to achieve significant reductions in normal tissue. These may, in turn, allow escalation of tumour dose and greater sparing of normal tissues, thus potentially improving local control (LC) and survival while at the same time reducing toxicity. Protons, accelerated to therapeutic energies ranging up to 250 MeV, typically with a cyclotron or a synchrotron, are transported to the treatment room where they enter the treatment head mounted on a rotating gantry. The initial thin beams of protons are spread laterally and longitudinally and shaped appropriately to the tumour treatment. Spreading and shaping is achieved using magnetic scanning of thin “beamlets” of protons of a sequence of initial energies to treat patients with optimized intensity modulated PT, the most powerful proton modality. Despite the high potential of PT, the clinical evidence supporting the broad use of protons is mixed. It is generally acknowledged that PT is safe, effective and recommended for many types of paediatric cancers, ocular melanomas or adult chordomas. Although some promising results have been reported, they are based on small studies. PT has been used to treat meningiomas since the early 1980s, though with outdated technologies and planning tools available at the time. However, PT technology has rather improved with modulated protons by pencil-beam scanning now available in all three centres in France since 2016. Although PT may afford higher control rates, evidence is limited to single institution series without comparison group. Thanks to the recent availability of the SNDS database, we gather the largest population of meningioma treated by PT. The paucity of similar works renders difficult our findings comparison as only a few reports examining outcome after PT for meningioma have been published (Table 6). Moreover, there are some discrepancies between these studies including proportion of patients undergoing surgery prior to PT, numbers of atypical meningioma or malignant meningioma and, tumour volumes ranging from 15.6 cm3 to 55.9 cm3 [19].
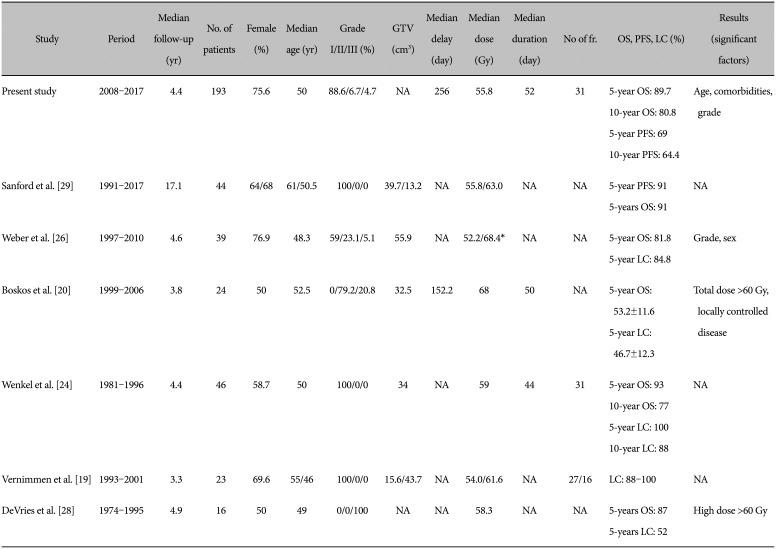
Table 6
Literature review on meningioma treated by protontherapy
| Study | Period | Median follow-up (yr) | No. of patients | Female (%) | Median age (yr) | Grade I/II/III (%) | GTV (cm3) | Median delay (day) | Median dose (Gy) | Median duration (day) | No of fr. | OS, PFS, LC (%) | Results (significant factors) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Present study | 2008–2017 | 4.4 | 193 | 75.6 | 50 | 88.6/6.7/4.7 | NA | 256 | 55.8 | 52 | 31 | 5-year OS: 89.7 | Age, comorbidities, grade |
| 10-year OS: 80.8 | |||||||||||||
| 5-year PFS: 69 | |||||||||||||
| 10-year PFS: 64.4 | |||||||||||||
| Sanford et al. [29] | 1991–2017 | 17.1 | 44 | 64/68 | 61/50.5 | 100/0/0 | 39.7/13.2 | NA | 55.8/63.0 | NA | NA | 5-year PFS: 91 | NA |
| 5-years OS: 91 | |||||||||||||
| Weber et al. [26] | 1997–2010 | 4.6 | 39 | 76.9 | 48.3 | 59/23.1/5.1 | 55.9 | NA | 52.2/68.4* | NA | NA | 5-year OS: 81.8 | Grade, sex |
| 5-year LC: 84.8 | |||||||||||||
| Boskos et al. [20] | 1999–2006 | 3.8 | 24 | 50 | 52.5 | 0/79.2/20.8 | 32.5 | 152.2 | 68 | 50 | NA | 5-year OS: 53.2±11.6 | Total dose >60 Gy, locally controlled disease |
| 5-year LC: 46.7±12.3 | |||||||||||||
| Wenkel et al. [24] | 1981–1996 | 4.4 | 46 | 58.7 | 50 | 100/0/0 | 34 | NA | 59 | 44 | 31 | 5-year OS: 93 | NA |
| 10-year OS: 77 | |||||||||||||
| 5-year LC: 100 | |||||||||||||
| 10-year LC: 88 | |||||||||||||
| Vernimmen et al. [19] | 1993–2001 | 3.3 | 23 | 69.6 | 55/46 | 100/0/0 | 15.6/43.7 | NA | 54.0/61.6 | NA | 27/16 | LC: 88–100 | NA |
| DeVries et al. [28] | 1974–1995 | 4.9 | 16 | 50 | 49 | 0/0/100 | NA | NA | 58.3 | NA | NA | 5-years OS: 87 | High dose >60 Gy |
| 5-years LC: 52 |
![]()
Nonetheless, the nationwide population-based cohort we described is quite alike these previous studies with proportions of female between 50% and 77% and median age at surgery ranging from 48.3 to 52.5 years. In our study, the median delay until PT was 256 days (IQR 152–574) vs. 152.2 days in Boskos et al. [20] series. Similarly, the median number of 30 fractions (IQR 30–33) given over a median time of 50 days (IQR 44–57) equals the PT duration of 50 days described by the former authors [20]. Usual PT practices in Orsay are to treat meningioma by fraction of 1.8 Gy of proton only. For benign meningioma, the treatment plan is 54 Gy in 30 fractions over 6 weeks vs. 59.4 Gy in 33 fractions for atypical meningioma and malignant meningioma. In Nice, the tendency is to deliver 60 Gy for atypical meningioma and up to 64 Gy in 2 Gy per fraction for malignant meningioma.
Outcome of patients treated for meningioma has been described as occasionally impaired with a 5-year OS of 80% all grades considered for Gennatas et al. [21] and, 5-year OS ranging from 86% to 91.5% (95% CI 87.4–95.5) for benign meningioma [2223]. Our 5-year OS rate of 89.7% (95% CI 84.6–95.1) compares favourably with other PT series with reporting 5-year OS rates between 53.2% to 100% (Table 6).
For the treatment of skull base tumours, high radiation dose greater than 54 Gy are usually required to obtain disease control. However, the close proximity of critical structures frequently precludes the delivery of such high dose even using the most advanced photon techniques such as non-coplanar VMAT. The physical properties of protons beams are well suited for the treatment of these deep-seated meningiomas with potential on the reduction of adverse effects, particularly cognitive dysfunction while sparing the hippocampi due to the possibility of highly conformal technique [14]. On 46 patients with benign skull base meningiomas treated with a combination of photons and protons, Wenkel et al. [24] reported recurrence-free rates of 100% and 88% at 5 and 10 years, respectively. For benign meningioma, fractionated or hypofractionated stereotactic PT led to 5-year LC rates ranging from 88% to 100% and equivalent to series with conventional RT [25]. For Weber et al. [26] who used only protons, 5-year LC and OS were 84.8% and 81.8% among 39 meningiomas of mixed grades with an average volume greater compared to other series (55.9 cm3). The 5-year grade 3/4 toxicity-free survival was 84.5%. Patients who experienced late-grade toxicities were those with large tumour volumes and optic tract meningiomas [26]. Thus, initial outcomes appear to support the use of PT for meningiomas, especially for lesions in close proximity to critical structures [14].
Dose escalation has been found to offer better 5-year PFS and OS for both atypical and malignant meningioma using dose ≥60 Gy [18202728]. On contrary, we found that dose escalation was associated to a shorter OS in univariable Cox regression analysis (HR=3.57, 95% CI 1.42–8.94, p=0.007). However, greater proton dose was given to aggressive meningioma (p<0.05). There is a statistical interaction between tumour grading, especially for malignant meningioma and PT dose above 60 Gy (p<0.001) which is therefore not an independent predictor of the OS. In a prospective randomized study of radiation dose escalation with combined proton-photon therapy for benign meningiomas, Sanford et al. [29] found no apparent benefit in dose intensification of 55.8 Gy to 63.0 Gy for benign meningioma. Further studies are thus needed to clarify the optimal treatment dose.
In our study, 33 patients (17.1%) had two or more PT treatments that did not improve the OS (HR=1.64, 95% CI 0.63–4.3, p=0.315). PT re-treatment for recurrent meningioma is feasible and allows good LC at moderate toxicity according to El Shafie et al. [30]. Our patients who had more than one PT irradiation or a calculated dose above 60 Gy did not demonstrate a higher frequency of toxicity (p>0.999 and p=0.723). Since recurrence may occur years after the initial treatment especially for benign meningioma, long-term follow-up is needed. Except the report by Sanford et al. [29] whose patients have been monitored for 17.1 years, most studies ours included, have a limited median follow-up time often below 5-years.
Factors affecting the outcome
Improved survival of females has already been described for many tumours and is attributed to fewer co-morbidities and higher clinical performance [31]. Our findings agrees this statement with males having significantly more co-morbidities (p=0.001). On the contrary to Weber et al. [26] findings, sex failed to be associated to the OS in our study (HR=0.45, 95% CI 0.18–1.14, p=0.093) probably because of the limited number of patients and the over-representation of females (75.6%) [26]. Without surprise, outcome after meningioma surgery and PT is better for younger adults. The age of 60 years marks a clear cut-off of reduced survival (Fig. 2C). The level of co-morbidities increases significantly along the lifetime (p=0.026) and was also associated to a decrease OS (HR=5.31, 95% CI 1.43–19.78, p=0.013). The SNDS allowed us to study several procedures associated to meningioma surgery such as preoperative embolisation, cranioplasty or internal CSF shunt insertion. The occurrence of hydrocephalus in meningioma patients is well documented and has been described to range from 2% up to 13%. For Burkhardt et al. [32] the incidence of communicating postoperative hydrocephalus was almost twice as high in patients with skull base lesions as in patients with convexity meningiomas. Moreover, they found that patient age and duration of surgery were the most significant predictors of postoperative hydrocephalus after skull base meningioma surgery [32]. CSF internal shunting reduced the morbidity and mortality of hydrocephalus. However, it is associated with a high level of complications such as shunt failure or infections [33]. These complications may require repeated surgeries and shunt revisions and is therefore associated with an increase risk of recurrence (HR=3.51, 95% CI 1.32–9.31, p=0.012) and an excess of mortality (HR=3.98, 95% CI 1.16–13.62, p=0.028).
Histopathological grading has been often reported as one of the uppermost predictors of the survival of meningioma patients. The proportions of benign (88.6%), atypical (6.7%), and malignant (4.7%) meningioma of the present study match somewhat usual figures. There is noticeable risk of decrease PFS and impaired OS for aggressive meningioma as displayed in the Fig. 1E and Fig. 2D, alike Weber et al. [26] findings.
PT possesses one main con: it is expensive. In France, the cost per treatment fraction is multiplied by 3.2, i.e., 743 € for protons vs. 233 € for photons [34]. No cost-effectiveness study of protons vs. photons has been undertaken in the treatment of meningioma nor has a study compared PFS or OS of meningioma patients after PT vs. conventional RT [35]. Considering its cost, it seems appropriate to assess whether PT improve outcome for meningioma not to mention Lesueur et al. [25] point of view: for skull base meningiomas, data from stereotactic series and IMRT present excellent LC with minimal side effects, thus any improvement with protons might only be marginal. The SNDS appears to be a suitable tool to answer the above-mentioned queries best after integration of more patients and extended follow-up.
Using this unique database, we found that 5-year PFS and OS after meningioma surgery and PT is favourable but impaired for older patients with high level of morbidities, tumour of the convexity, malignant histopathology and for those having a hydrocephalus requiring internal CSF shunting. Further inclusion and prolonged follow-up is required to assess other predictors such as sex, tumour volume, or given dose.
Go to :
 XML Download
XML Download