

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neurenteric cyst of the central nervous system is a congenital lesion characterized by misplaced endodermal epithelial cells. It is a rare benign lesion of the central neural axis that primarily occurs in the lower cervical or upper thoracic spine and accounts for 1.3% of all spinal cord tumors [12]. To date, only 80 cases of intracranial neurenteric cysts have been reported in the literature, and these cysts were located at the midline of the posterior fossa, cerebellopontine angle, fourth ventricle and brain stem [3]. Since only a few cases of neurenteric cyst at the anterior craniocervical junction have been reported, its treatment and prognosis remain unclear [45]. We present a case of neurenteric cyst at the anterior craniocervical junction that was surgically treated using the far-lateral transcondylar approach.
CASE REPORT
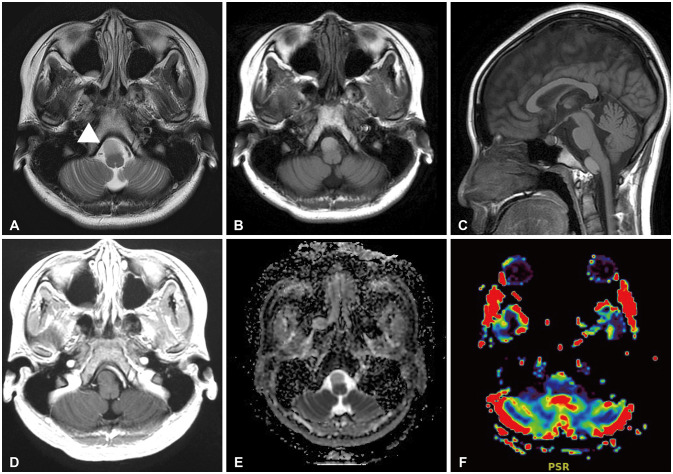
A 16-year-old girl presented with slowly progressive headache. MRI showed a well-defined, 14×16×20 mm, intradural extramedullary cystic lesion in the premedullary cistern (Fig. 1). The lesion was homogeneously hyperintense on T1- and T2-weighted images. There was no restriction on diffusion-weighted imaging. Slightly elevated cerebral blood flow and cerebral blood volume were noted in the anterior part of the cystic mass on perfusion-weighted imaging. There was no gadolinium contrast enhancement on MRI.
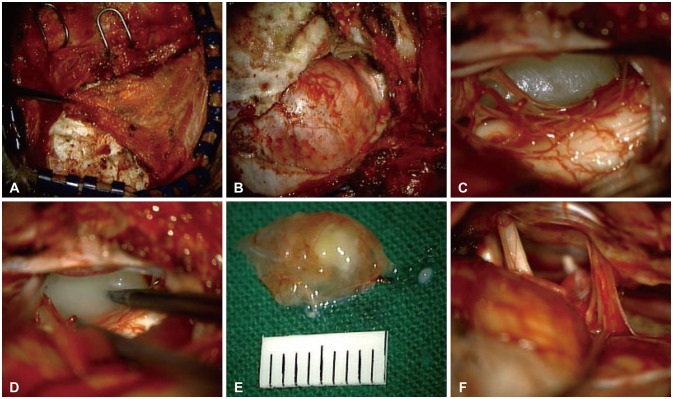
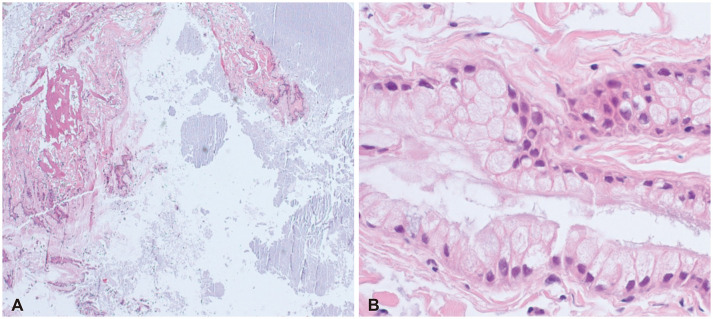
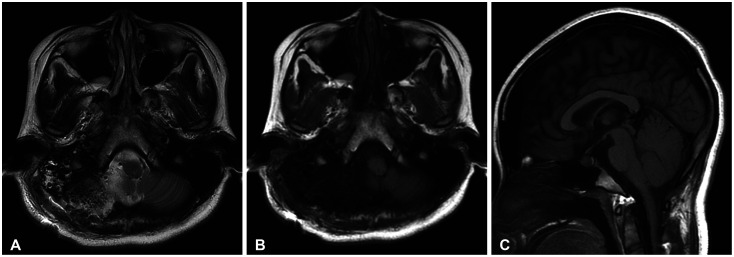
We decided to perform surgery to prevent symptom progression and avoid neurologic deficit. A far-lateral transcondylar approach was chosen to secure the surgical field and prevent cranial nerve injury (Fig. 2). We performed lateral suboccipital craniotomy with minimal condylectomy and secured the surgical field, which included the anterior aspect of the medulla and the premedullary cistern. The cyst was located following arachnoidal dissection of the cranial nerves and vertebral artery. The cyst was covered by a light gray capsule, which was loosely connected to the brain parenchyma. The cystic wall was punctured, and an amorphous gray-yellowish fluid was drained. The residual cyst capsule was completely detached from the adjacent neurovascular structures. Histopathological examination revealed non-ciliated, mucin-producing columnar and cuboid epithelial cells with isolated goblet cells, which are characteristic features of neurenteric cyst (Fig. 3). Complete surgical resection of the cyst was performed without any complications. MRI conducted postoperatively confirmed that the mass had been completely resected (Fig. 4). No adverse events occurred during 6-month follow-up period.
DISCUSSION
Neurenteric cyst is a rare congenital anomaly that usually associated with vertebral anomalies [6]. Embryologically, it is a central nervous system lesion of endodermal origin, and it has been known as enterogenous cyst, teratoid cyst, enteric cyst, respiratory cyst, endodermal cyst, gastrocytoma, intestinoma, and archenteric cyst [7]. Most intracranial neurenteric cysts are located at the craniocervical junction, fourth ventricle, or basal cistern, that is, anterior to the brain stem. Acute neurologic deficit is rare, and most symptoms are due to the mass effect of the slowly growing cysts [8].
The treatment of choice in symptomatic patients is complete surgical resection. Because of the risk of recurrence or malignant change due to incomplete resection, the goal of surgery is to resect both the cyst wall and its contents, completely [9]. The major determinant for complete neurenteric cyst resection is whether the arachnoid plane between the tumor and the surrounding tissue is preserved. Subtotal cyst resection is an alternative technique used in patients with severe adhesion to prevent damage to adjacent neurovascular structures [10]. However, revision surgery may be required if neurenteric cyst recurrence occurs from the remnant of cyst wall [1112]. The rate of recurrence following incomplete cyst resection varies, with overall recurrence rates is between 11.6% and 37% reported in different studies [1314]. To resect neurenteric cyst located in ventral craniocervical junction completely, many different surgical approaches have been discussed in literature. In many cases, the cyst was resected through suboccipital craniotomy, with or without cervical laminectomy, using a conventional posterior approach [1516]. Since the neurenteric cysts are located anterior to the medulla and cervical cord, a secure surgical field is necessary for the resection of the cyst using decompression through cyst aspiration. However, when the cyst wall is adhered to the anterior structure, it is difficult to view the cyst from its posterior side, there is a high risk of damage to the medulla and cervical cord due to intraoperative manipulation and retraction.
In some cases, an anterior approach such as a transoral approach is used for complete neurenteric cyst resection [1718]. Although the transoral approach provides a wide intraoperative view and access to the anterior craniocervical lesion, it is technically difficult and is often associated with fatal postoperative complications such as infection [18].
The far-lateral transcondylar approach is considered the most effective technique for managing anterior craniocervical lesions [19]. Satisfactory surgical outcomes and prognoses have been reported for cyst resection using the far-lateral transcondylar approach [2021]. This approach provides a direct intraoperative view of the lower clivus, anterior craniocervical junction, and neurenteric cysts at the anterior brain stem and cervical cord without retraction of the medulla and cervical cord. In the case series on the surgical resection of neurenteric cysts at the anterior craniocervical junction using a far-lateral transcondylar approach, Menezes et al. [22] reported that in all 5 patients, who had extramedullary neurenteric cysts located anterior to the foramen magnum, the lesion was completely resected using far-latral transcondylar approach. After complete resection, all symptoms and signs were improved, and there was no recurrence for 1 to 28 years. Adequate working space can be secured through condylar resection and vertebral artery exposure. Depending on the extent of occipital condylar resection, there may be increased instability, necessitating occipitocervical fusion. In general, it is known that removal of one-third of the occipital condyle does not cause instability [23].
Clinical and radiological follow-up is needed for at least 5 to 10 years after surgery [24]. Because of the risk of recurrence, patients with a residual mass or residual cyst wall may require longer follow-up.
Neurenteric cyst is a rare, benign central nervous system lesion. Although it usually occurs in the cervical or thoracic spine, intracranial neurenteric cysts should be considered during the differential diagnosis of intracranial cystic lesions. When symptoms developed and surgical resection is to be performed, based on our experience, the far-lateral transcondylar approach is the optimal technique for improving the prognosis through complete cyst resection as it provides a good intraoperative view of the cyst and adjacent neurovascular structures while minimizing brain retraction.
 XML Download
XML Download