

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Petroclival meningioma (PCM), closely associated with various cranial nerves and vascular structures, frequently extends into the cavernous sinus or middle cranial fossa, leading to difficulty in exposure during surgery and relatively high surgical morbidity or mortality [12]. Even though most PCMs follow a benign clinical course, gross total resection (GTR) is considered the ideal treatment if possible. When GTR is not possible or postoperative complications are anticipated, the recent trend is to perform radiation treatment or radiosurgery by adjuvant treatment after subtotal resection [3]. In addition, Gamma Knife radiosurgery (GKRS) can be conducted as an initial alternative treatment for PCM, as in skull base meningiomas. Although the effectiveness of adjuvant or alternative GKRS for PCM has already been demonstrated in several studies [345678], the precise treatment guidelines have not yet been established.
In this study, we investigated the tumor control and complication rates in patients undergoing alternative or adjuvant GKRS in our institution. In addition, considering factors influencing the therapeutic effect of GKRS, we tried to determine which patients with PCM were eligible for GKRS.
Go to : 
MATERIALS AND METHODS
Patient population
This study was approved by the Institutional Review Board of the hospital, which waived the requirement for informed consent due to the retrospective nature of the study. The subjects of this study were 64 patients who underwent GKRS for PCM in our hospital from 2004 to 2019. The patients were diagnosed with meningioma by MRI and pathologic reports. To define the clinical characteristics of the patients with PCMs, clinical data at the time of GKRS, including age, sex, KPS score, the type of treatment, pretreatment symptoms, multiplicity, perilesional edema, T2 signal intensity, initial volume, maximal diameter, the use of fractionation, and the presence of progression were collected.
Progression-free survival (PFS) of PCM was defined as the interval until the progression of PCM after GKRS. After GKRS, we defined complications as permanent neurologic deficits or sequelae, not transient. If the deficit persisted longer than 6 months or needed surgical intervention, it was regarded as a permanent complication. Minor symptoms, such as headache and dizziness, controlled by usual medications were not considered complications.
Radiosurgical technique
Radiosurgery was performed as usual. After applying the Leksell stereotactic frame under local anesthesia, high-resolution MRI was performed to obtain information about the shape and volume of the tumors. The treatment plan was carried out by a neurosurgeon and a medical physicist. The median isodose line of the tumor was 50% (range, 45–50%) and the median marginal dose was 12 Gy (range, 10–14 Gy). When fractionated GKRS was needed, the number of fractions was classified as 2–3 based on the tumor status (three fractionations in 14 patients, two fractionations in 5 patients). The frame was maintained until the last irradiation fractionation was completed. The linear quadratic model was used to calculate the biologically effective dose for fractionation. Detailed methods for the fractionations appear in a previously published paper [9].
Volumetric analysis
A follow-up MRI was initially obtained 6 months after GKRS and then annual imaging was conducted for the rest of the patient's life. Tumor volume (TV) analysis was performed by Leksell GammaPlan Ver. 10.1.1 (Elekta AB, Stockholm, Sweden). Using the volumetric tools included in Leksell GammaPlan, we drew slice-by-slice anatomical regions of interest (ROI) in the MRI and defined the three-dimensional volume in the ROI. Since the ROI was manually outlined by freehand drawing, it was important to describe the boundary between the tumor and normal tissue. In order to more accurately contour the ROI and more accurately track changes in the TV, co-registration image studies using a reference MRI (pre-GKRS) and follow-up MRI were performed. The collaboration process was automatic and based on an algorithm consistent with mutual MRI information. The ROI for the subsequent MRI was outlined in the co-registered image window overlaid with the ROI from the reference MRI. From the ROI obtained from this image, the study produced a three-dimensional TV and calculated its size. More than 20% increase in volume compared to the initial MRI at the time of GKRS was conducted tumor progression.
Statistical analysis
PFS and the tumor control rates were determined using the Kaplan-Meier method with a log-rank test. For univariate analysis, Fisher's exact test or a chi-square test was used for the categorical variables, and Student's t-test was used for the continuous variables. For multivariate analysis, binary logistic regression for post-GKRS complications and Cox regression for PFS were used. All statistical analyses were performed using SPSS version 20.0 for Windows (IBM Corp., Armonk, NY, USA). A p-value of <0.05 was considered significant.
Go to :
RESULTS
Patient population and treatment characteristics
Table 1 summarizes the clinical and radiological features of the patients. Among 64 enrolled patients, the tumor was restricted to the petroclival region in 30 patients and 34 patients showed tumor extension into other portions. GKRS was adopted as an initial alternative treatment in 52 patients and as an adjuvant treatment after surgical resection in 12 patients. Multiplicity was observed in 10 patients. The mean tumor size was 2.9 cm (range, 1–6 cm) and the mean TV was 13.4 cm3 (range, 0.4–64.9 cm3). The tumor size and volume based on 5 cm and 15 cm3, respectively, were used to classify the patients. Fifty patients had incidentally detected tumors or complained only of minor symptoms, and 14 patients had motor or sensory deficits, multiple cranial nerve signs, or brainstem signs. Moderate to severe perilesional edema was found in 14 cases on pretreatment MRI and the remaining 50 showed little or only mild edema.
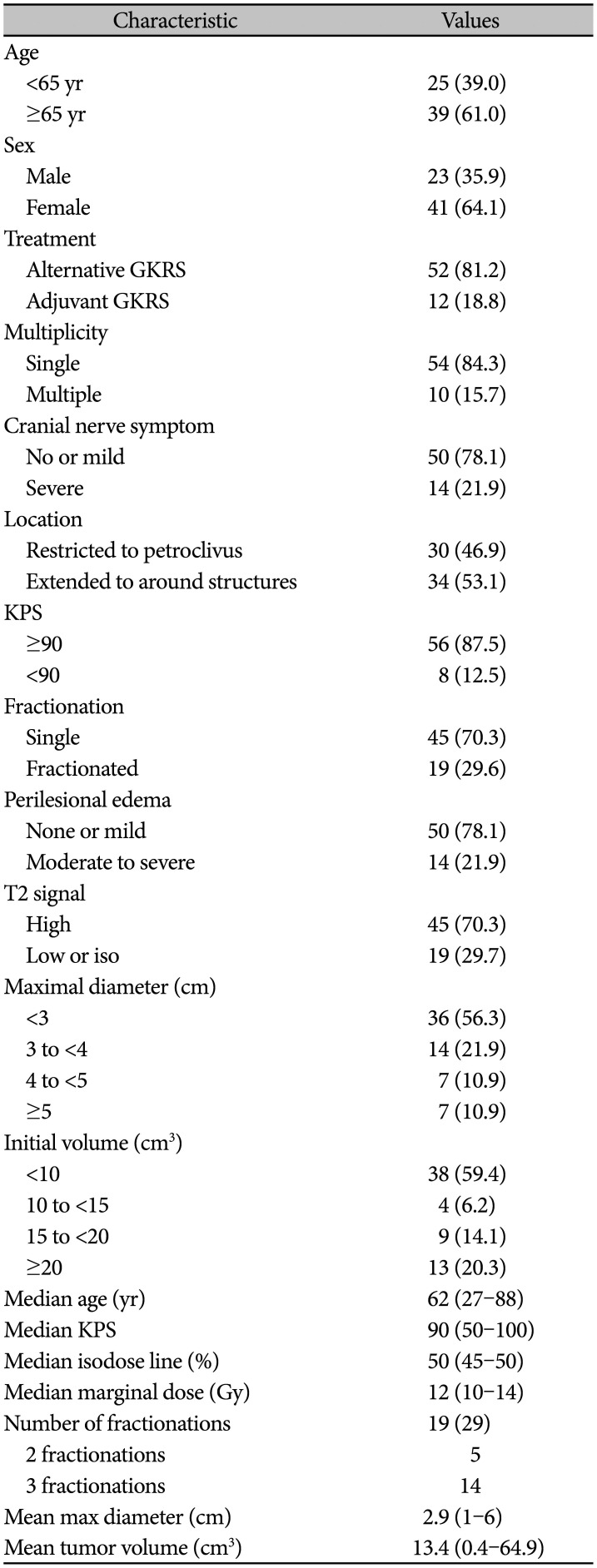
Table 1
Clinicoradiological characteristics of 64 patients with petroclival meningioma
![]()
Tumor control
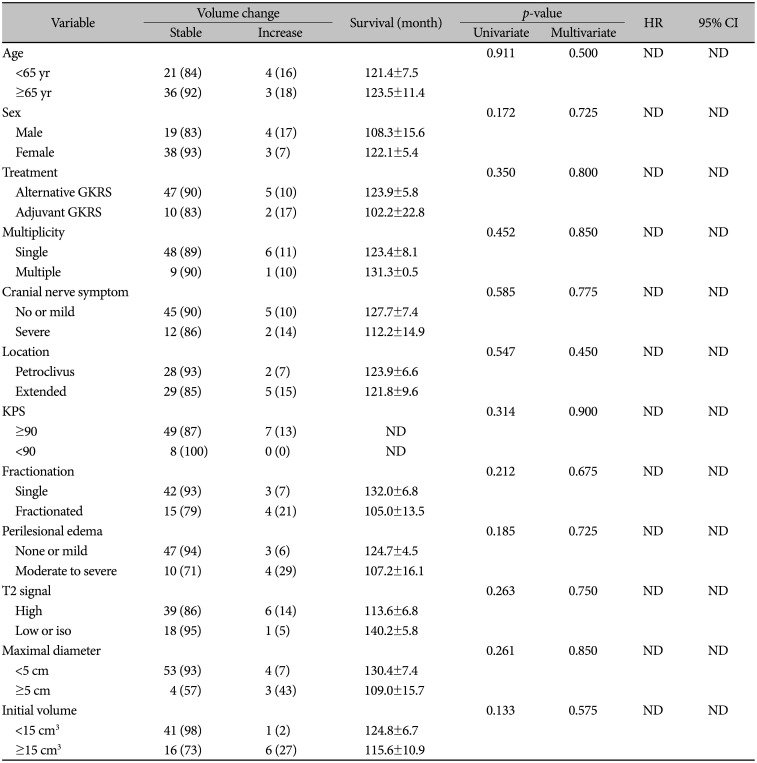
The mean radiologic follow-up duration was 58.4 months (range, 6–164 months). The overall 5-year PFS rate was 91.1% and the 10-year PFS was 69.6% (Fig. 1). Although no clinicoradiological factor showed statistical significance, some factors, including sex, peritumoral edema, and large volume, were marginally correlated with survival benefit on univariate analysis. On multivariate analysis, no factor was associated with PFS (Fig. 2, Table 2).
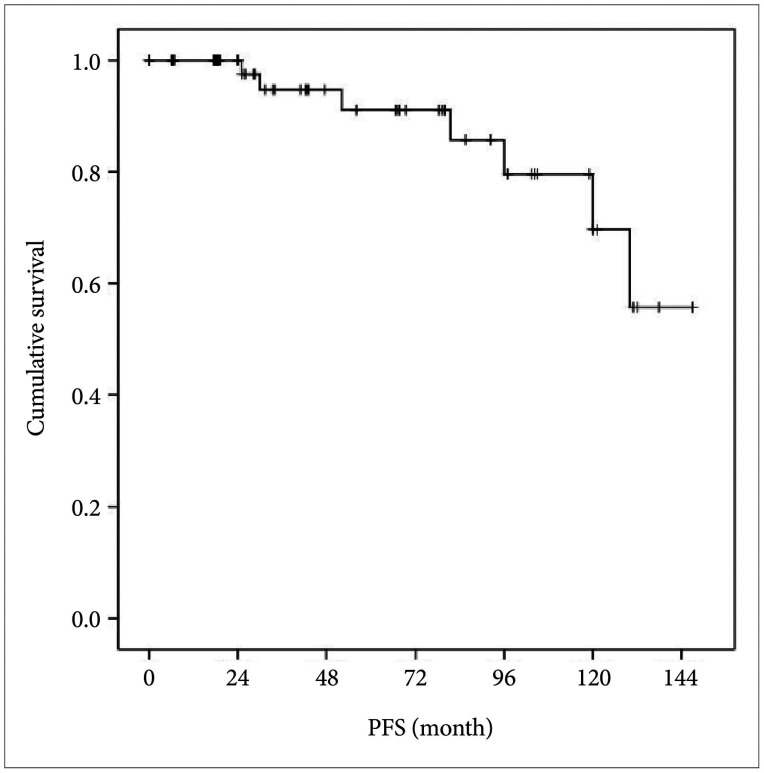 | Fig. 1Kaplan-Meier curves showing the progression-free survival (PFS) and cumulative survival of the enrolled patients in this study (overall comparison was estimated using a log-rank test). The overall 5-year PFS rate was 91.1% and the 10-year PFS was 69.6%.
|
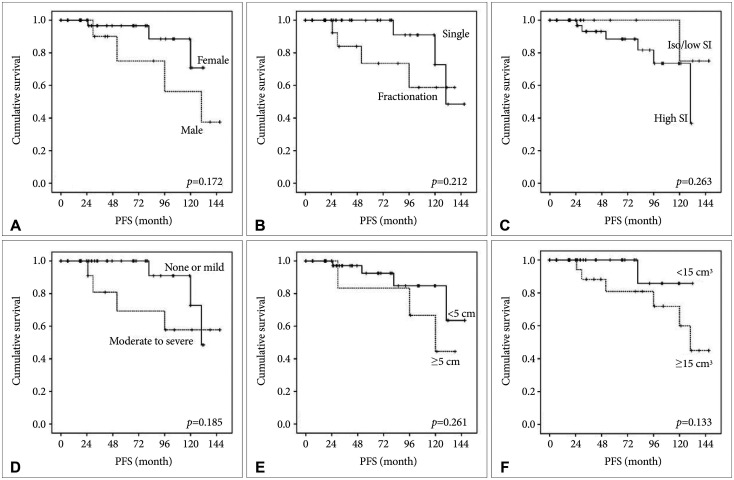 | Fig. 2Kaplan-Meier curves showing progression-free survival (PFS) according to different predictors (overall comparison was estimated using a log-rank test). The number on the right upper of each curve represents the p-value. A: sex, B: fractionation, C: T2 signal intensity (SI), D: perilesional edema, E: maximal diameter, F: tumor volume.
|
Table 2
Statistical analyses for progression-free survival of the patients with petroclival meningioma
![]()
Post-GKRS complications
Ten patients developed new symptoms after GKRS. Fifty-four out of 64 patients did not reveal any permanent neurologic deficits or sequelae, indicating a stable neurologic state of 84.4%. The most common complication was cranial nerve deficits (n=8, especially 5th and 7th cranial nerve symptoms) followed by hemiparesis, cognitive dysfunction, and hydrocephalus. The presence of multiplicity [p=0.009, hazard ratio (HR) 0.102, 95% confidential index (CI) 0.018–0.573] and large maximal diameter (p=0.013, HR 0.091, 95% CI 0.014–0.608) on pre-GKRS MRI were independent predictive factors for developing post-GKRS complications (Table 3).
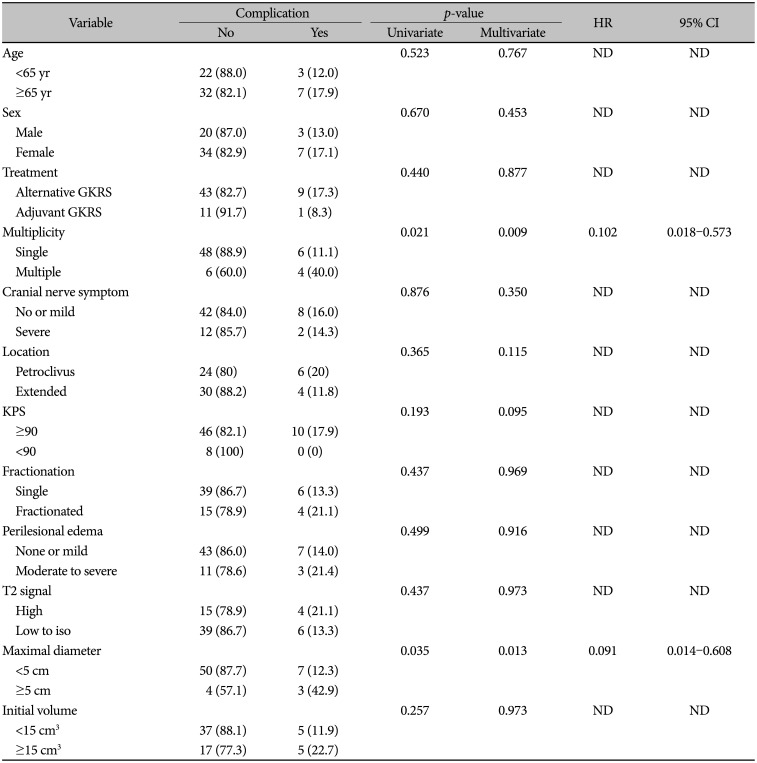
Table 3
Univariate and multivariate analyses for post-GKRS new onset symptoms from the treatment for petroclival meningioma
![]()
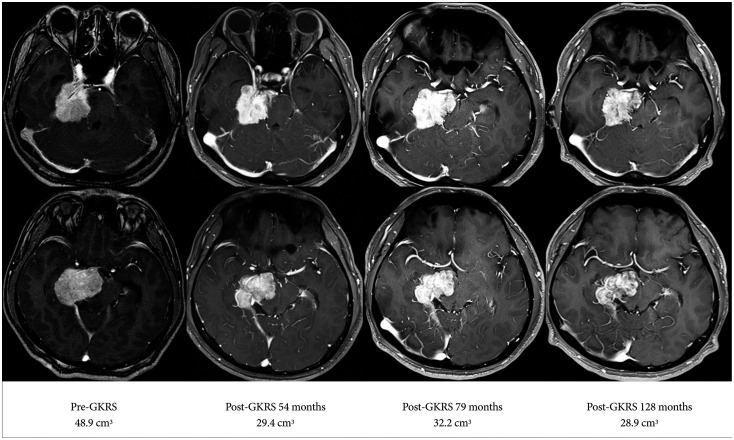
Representative case 1
A 39-year-old man visited our hospital with diplopia as a chief complaint. The patient also complained of gait disturbance and 48.9 cm3 of PCM was diagnosed on the MRI. Although the tumor had a perilesional edema and an indistinct margin with the brainstem, surgical resection was recommended. The patient and his family were concerned about the possibility of postoperative complications and decided to undergo alternative GKRS. The radiosurgery was performed with three fractionations of 6 Gy and 50% isodose (total 12.7 Gy). Fifty-four months after treatment, the follow-up MRI showed a size reduction of 29.4 cm3 and a clinically stable state without discomfort. The last follow-up MRI performed at 128 months showed a well-controlled mass with a shrunken volume of 28.9 cm3. Diplopia and the gait disturbance were completely improved and there were no other complications (Fig. 3).
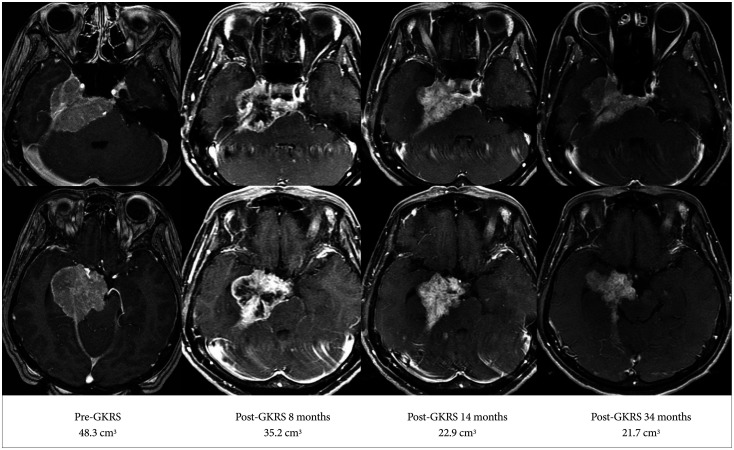
Representative case 2
A 58-year-old woman visited the medical center complaining of a visual field defect on the right temporal side. Mild 6th nerve palsy was also observed. MRI showed a large sized PCM invading cavernous sinus on the right side. The patient and his family wanted the alternative GKRS mainly due to mild clinical symptoms. Radiosurgery was conducted as usual, with a single session of 12 Gy and 50% isodose. The mass gradually decreased in volume on serial follow-up MRIs after the detection of internal necrosis. There were no specific complications other than mild 6th nerve palsy that appeared to be initial (Fig. 4).
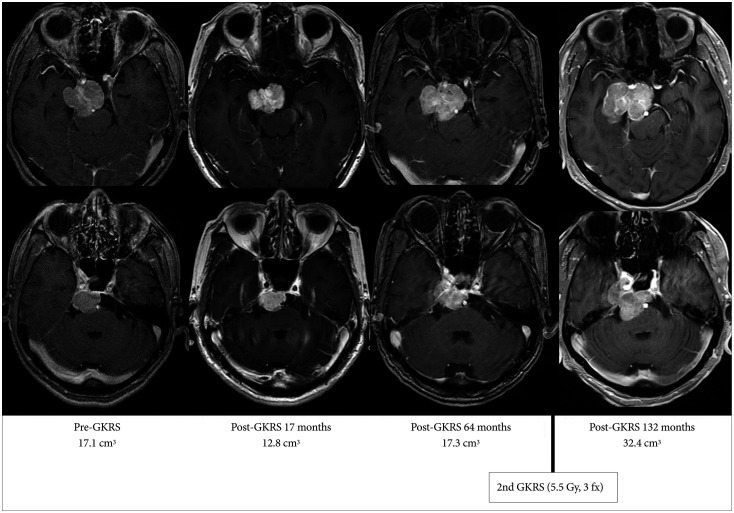
Representative case 3
An 82-year-old woman visited our hospital for further evaluation of an incidentally detected mass. There were no neurological symptoms or signs. The patient wanted to undergo alternative GKRS. Fractionated GKRS was performed uneventfully (5.5 Gy/fraction, 3 fractions, and 50% isodose). Even though the TV was reduced on the early follow-up MRI, the mass gradually increased and another fractionated GKRS was performed at 5.5 Gy. There were no symptoms or patient complaints, but the follow-up MRI performed 11 years after the 1st GKRS showed progression of the mass with a volume of 32.4 cm3 (Fig. 5).
Go to :
DISCUSSION
Although PCM has benign tumor characteristics, it is more likely to cause post-operative complication as it spans the clivus and petrous portions where vascular structures and cranial nerves are located. Therefore, other alternative methods may be considered when a high possibility of complications and morbidity is anticipated after surgical resection [10].
A recent study summarized the treatment outcomes of patients with PCM for 30 years in a single institution. The authors analyzed several types of multimodal treatments to establish an optimal management strategy for PCM. Interestingly, their study showed no progression for five years in both the group with GTR and the group with additional radiotherapy or radiosurgery, even without GTR. The GTR rate had been decreased since 2000 with the frequent use of GKRS as an adjuvant treatment, and the complication rate tended to decrease. The authors concluded that, considering local tumor control and postoperative quality of life, adjuvant radiosurgery after planned incomplete resection would be a good option [3]. Bernard et al. [11] conducted a retrospective study of 154 patients who underwent treatment for PCMs larger than 2.5 cm from 1984 to 2017. The 5-, 10-, and 15-year PFS were not significantly different between the GTR group and the non-GTR group with adjuvant radiation treatment (100, 90, and 75%, respectively). In the group that did not receive adjuvant radiation treatment after subtotal removal, 5-, 10-, and 15-year PFSs were clearly reduced to 71, 51 and 31%, respectively. Based on these results, it can be argued that planned subtotal resection without injury to the cranial nerves, brain stem or vascular structures, followed by radiation therapy or GKRS, especially for a difficult case anticipated to have high possibility of postsurgical complications should be performed [1213].
Recently, it has been suggested that GKRS is effective as an alternative treatment for PCMs, as it is for other intracranial meningiomas [14151617181920]. In fact, the reason neurosurgeons were reluctant to choose GKRS as the primary treatment for PCM was because of concerns regarding the injury of the cranial nerve and brain stem caused by radiation-induced toxicity. In addition, when the tumor presented with a large volume and wide extension into the multi-cranial fossa, they were concerned about a higher failure rate of GKRS. Furthermore, there are not many studies on the outcomes of GKRS for PCMs [3456782122] (Table 4).
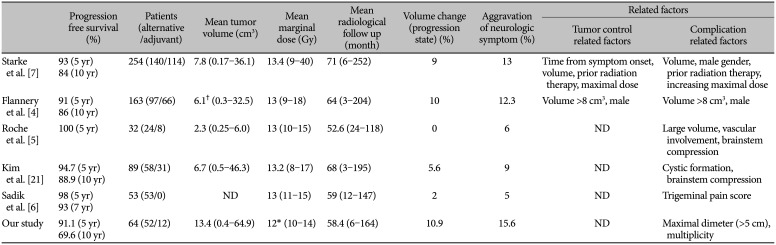
Table 4
Comparison of Gamma Knife radiosurgery outcomes and tumor control and complications related factors in selected studies
| Progression free survival (%) | Patients (alternative/adjuvant) | Mean tumor volume (cm3) | Mean marginal dose (Gy) | Mean radiological follow up (month) | Volume change (progression state) (%) | Aggravation of neurologic symptom (%) | Related factors | ||
|---|---|---|---|---|---|---|---|---|---|
| Tumor control related factors | Complication related factors | ||||||||
| Starke et al. [7] | 93 (5 yr) | 254 (140/114) | 7.8 (0.17–36.1) | 13.4 (9–40) | 71 (6–252) | 9 | 13 | Time from symptom onset, volume, prior radiation therapy, maximal dose | Volume, male gender, prior radiation therapy, increasing maximal dose |
| 84 (10 yr) | |||||||||
| Flannery et al. [4] | 91 (5 yr) | 163 (97/66) | 6.1† (0.3–32.5) | 13 (9–18) | 64 (3–204) | 10 | 12.3 | Volume >8 cm3, male | Volume >8 cm3, male |
| 86 (10 yr) | |||||||||
| Roche et al. [5] | 100 (5 yr) | 32 (24/8) | 2.3 (0.25–6.0) | 13 (10–15) | 52.6 (24–118) | 0 | 6 | ND | Large volume, vascular involvement, brainstem compression |
| Kim et al. [21] | 94.7 (5 yr) | 89 (58/31) | 6.7 (0.5–46.3) | 13.2 (8–17) | 68 (3–195) | 5.6 | 9 | ND | Cystic formation, brainstem compression |
| 88.9 (10 yr) | |||||||||
| Sadik et al. [6] | 98 (5 yr) | 53 (53/0) | ND | 13 (11–15) | 59 (12–147) | 2 | 5 | ND | Trigeminal pain score |
| 93 (7 yr) | |||||||||
| Our study | 91.1 (5 yr) | 64 (52/12) | 13.4 (0.4–64.9) | 12* (10–14) | 58.4 (6–164) | 10.9 | 15.6 | ND | Maximal dimeter (>5 cm), multiplicity |
| 69.6 (10 yr) | |||||||||
![]()
Subach et al. [8] reported 62 patients with PCM treated by GKRS. During the median follow-up period of 37 months, only five patients (8%) developed new complications, such as cranial nerve deficits, and none had evidence of tumor progression. Flannery et al. [4] reported on 163 patients who underwent GKRS for PCMs during a 21-year interval. The median TV was 6.1 cm3 and the mean radiating dose to the tumor margin was 13 Gy. The overall 5-year PFS rate was 91% and the 10-year PFS was 86%. Among the patients who underwent primary GKRS in the study, 12 patients out of 97 showed aggravation of neurologic symptom (12.3%). Patients with tumor progression complained of facial pain, hydrocephalus, deteriorating balance, vocal cord paresis, and headache. They concluded that the tumor progression and symptom deterioration related factors were tumors over 8 cm3 and male sex. Starke et al. [7] studied 254 patients diagnosed with PCM from multiple centers. In their study, the mean volume was 7.8 cm3 (rang, 0.17–36.1 cm3), the 5-year PFS was 93%, and the 10-year PFS was 84%. Neurologically stable states after GKRS were found in 93.6% of the patients. They concluded that the predictors for tumor included increasing-interval time from diagnosis to radiosurgery, large initial TV, previous radiotherapy history, and decreasing maximal dose. The predictors for unfavorable clinical outcome included the large initial TV, male sex, previous radiotherapy history, and increasing maximal dose. Kim et al. [21] reported 94.7% and 88.9% 5-year and 10-year PFSs, respectively, with a mean TV of 6.7 cm3. Eighty-one of 89 patients (91%) showed neurologically stable states after GKRS.
In our study, the overall 5-year PFS was 91.1% and the 10 year PFS was 69.6%. Compared to other studies, the results worse, and this is because the mean TV of the study subjects was larger in our study. The mean maximum diameter was 2.9 cm (range, 1–6 cm) in our study, and the mean TV was 13.4 cm3 (range, 0.4–64.9 cm3). Complications were found in 10 out of 64 patients and 84.4% were neurologically stable, which was relatively lower than the results of other studies. Increased diameter and multiplicity were independently related with complication after GKRS. Although the clinical outcome and growth rate in multiple meningiomas has been reported to be similar to a solitary case [2324], unknown biological behaviors including inconsistent pathological features [25] in multiple meningiomas may lead to unexpected clinical outcome after GKRS. Based on our results, we concluded that GKRS was shown to be an effective and safe treatment strategy for large-sized PCMs, as an alternative or adjuvant treatment. Research on how GKRS can overcome limited situations such as large-volume tumors and the complications of surrounding structures, is ongoing. Fractionated GKRS can be considered an answer to that question [92627].
Some limitations exist in this retrospective study. It was conducted on a small number of patients in a single institution with a wide range of follow-up periods. Prospective studies with a large scale and long-term follow-up period are needed to clarify the effectiveness and safety of GKRS for PCM.
In conclusion, considering the surgical morbidity of PCM, GKRS could be considered an effective alternative or adjuvant treatment in selective patients. Although there was no predictive factor for PFS for PCM, multiplicity and large size were independent predictive factors for post-GKRS complications in our study.
Go to :
 XML Download
XML Download