

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lymphopenia, defined as a reduction in total lymphocyte count (TLC), frequently occurs after concomitant chemoradiation (CCRT) for glioblastoma (GBM), and it was recently suggested as a novel biomarker associated with overall survival (OS) in newly diagnosed GBM [123456]. As lymphocytes play a major role in the immune response to eliminate malignant cells, an insufficient number of circulating lymphocytes could weaken the immune system's control of GBM progression [78910].
Several clinical factors have been suggested as contributors to lymphopenia including sex, age, irradiated brain volume, chemotherapy, and the use of dexamethasone [1112131415161718]. Radiotherapy (RT) was found to be significantly associated with lymphopenia in GBM patients [10111415161819]. Dexamethasone, which is a commonly prescribed drug for controlling brain edema and improving performance of GBM patients, is also known for its potent immunosuppressive effects [202122]. However, its effect on inducing lymphopenia in GBM patients remains controversial [11141517]. Three previous studies did not find an association between the use of dexamethasone and acute lymphopenia [111415], but another study showed that increased use of dexamethasone during CCRT was an independent risk factor for acute lymphopenia after CCRT [17]. As numerous immunotherapeutic agents are being developed for GBM, it is critical to minimize iatrogenic lymphopenia to maintain sufficient immunity to fight against cancer cells [1023].
In this context, we attempted to elucidate the clinical factors associated with lymphopenia following CCRT in patients with newly diagnosed GBM focusing specifically on the use of dexamethasone. We examined the overall cumulative dose of dexamethasone from initiation of CCRT to 4 weeks after completion of CCRT to facilitate a more accurate evaluation of this association.
MATERIALS AND METHODS
Patient selection
Our study was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC19RESI0168). The need for informed consent was waived due to the retrospective nature of our study. The electronic medical records (EMR) of 186 patients with newly diagnosed GBM who were treated at our institution between August 2009 and December 2017 were retrospectively examined. The eligibility criteria were as follows: 1) newly diagnosed GBM confirmed by craniotomy or stereotactic biopsy, 2) completion of CCRT at our institution, 3) accessible baseline and follow-up complete blood count (CBC). The exclusion criteria were as follows: 1) prior history of diagnosed malignancies, chemotherapy, or radiation due to other medical illnesses, 2) evidence of acute infection or autoimmune disease at the time of blood sampling.
Clinical variables and treatment protocols
Patient characteristics included sex, age, performance status, extent of resection (EOR), pathologic findings, radiation dosage and fraction, radiation volume, radiation modalities, dose of dexamethasone used, and CBC. Performance status at baseline was measured using the Eastern Cooperative Oncology Group (ECOG) performance score. EOR was measured by comparing radiologic findings on MRI at baseline and within 48 hours after surgery. Resection of 90% or more of the tumor volume was considered gross total resection (GTR) and <90% was considered non-GTR [24]. Isocitrate dehydrogenase 1 (IDH1) mutation was evaluated by immunohistochemistry or direct sequencing.
O6-methylguanine-DNA methyltransferase (MGMT) gene methylation status was evaluated by polymerase chain reaction.
We used navigation and intraoperative monitoring in all surgeries and we also performed awake surgery or 5-aminolevulinic acid fluorescence-guided surgery, for achieving maximal safe resection, when indicated. CCRT was started within 28 days of surgical resection if possible, considering wound healing, the patient's condition, and RT schedules [25]. Radiation was administered at a dosage of either 5,940 cGy for 33 fractions or 6,000 cGy for 30 fractions, regardless of age. RT was conducted with either three-dimensional conformal RT (3DRT) or intensity-modulated RT (IMRT). Temozolomide (TMZ) dosages were 75 mg/m2 during CCRT and 150–200 mg/m2 for adjuvant therapy. We used dexamethasone, considering the patient's neurologic status, general condition, and radiologic findings after surgery to control brain edema and improve patient performance. Other steroids including prednisolone were not prescribed.
TLC and dexamethasone
We collected results of blood tests, including white blood cell count and the composition of neutrophils and lymphocytes, at baseline and 4 weeks after completion of CCRT. TLC were calculated from these data for the analysis.
We also reviewed prescribed dexamethasone doses using EMR from initiation of CCRT until 4 weeks after the completion of CCRT, which was the same day blood samples were collected for calculating TLC. We estimated the cumulative dexamethasone dose from the EMR. Median dexamethasone dose prescribed during this period was calculated by dividing the cumulative dexamethasone dose (mg) by the days from initiation of CCRT to 4 weeks after the completion of CCRT. For example, if a patient took a cumulative dexamethasone dose of 200 mg over 80 days from initiation of CCRT to 4 weeks after completion of, the median daily dexamethasone dose was 2.5 mg. In our study, the median period from initiation of CCRT until 4 weeks after completion of CCRT was 78.3 (range 65–98) days.
Statistical analysis
Lymphopenia was defined as TLC <1,000 cells/µL at 4 weeks after completion of CCRT, based on previous reports. The primary endpoint in our study was OS. OS was calculated using the time interval from date of initial surgery to death. Dates of death were obtained from the Korea Central Cancer Registry database. Patients who were confirmed alive on July 30, 2019 were censored. The median follow-up period was 26.1 (range 4–117) months.
All clinical variables were characterized with descriptive statistics. Differences between groups in which dexamethasone was and was not used were compared with Fisher's exact test or the chi-squared test. A test of normality was performed for continuous variables. Univariate and multivariate analyses were conducted using the Cox proportional regression model. The hazard ratio (HR) and 95% confidence intervals (CIs) were calculated. Multivariate analysis was performed using the variables with p-values <0.2, and p-values <0.05 were considered statistically significant. Statistical analysis was performed using R Statistical Software (Version 3.4.4; R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Patient characteristics
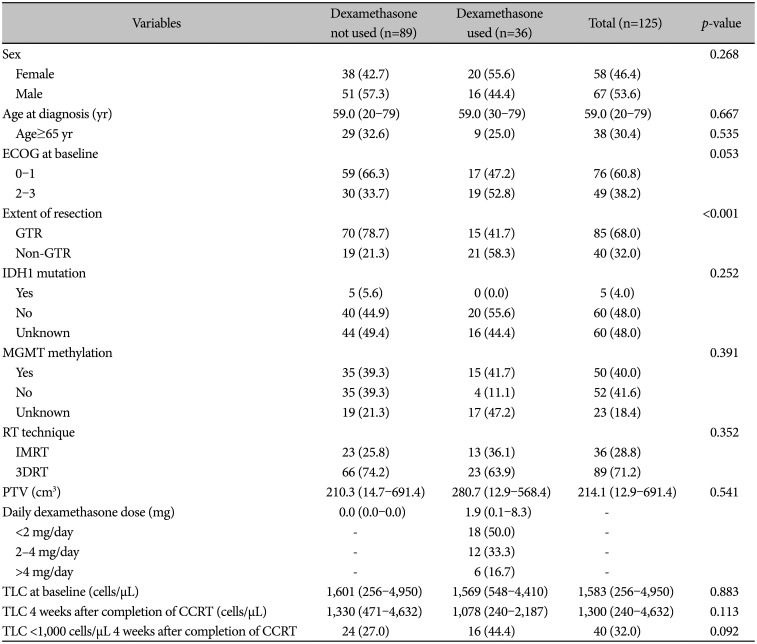
We included 125 patients who met our eligibility criteria. Of them, 89 patients who did not take any dexamethasone were assigned to the “not used group” and 36 patients who took dexamethasone were assigned to the “used group.” Baseline patient characteristics are shown in Table 1. The “used group” had poor ECOG performance score at baseline and had more patients who underwent non-GTR, while other clinical variables including sex, age, IDH1 mutation status, presence of MGMT promoter methylation, median planning treatment volume (PTV), median TLC at baseline and at 4 weeks after completion of CCRT, and proportion of lymphopenia were not significantly different. The median daily dexamethasone dose (mg) in the “used group” was 1.9 (range 0.1–8.3) mg/day. Eighteen of 36 patients (50%) took a median dexamethasone dose less than 2.0 mg/day, 12 patients (33.3%) from 2.0 to 4.0 mg/day, and 6 patients (16.6%) more than 4 mg/day.
Lymphopenia and overall survival
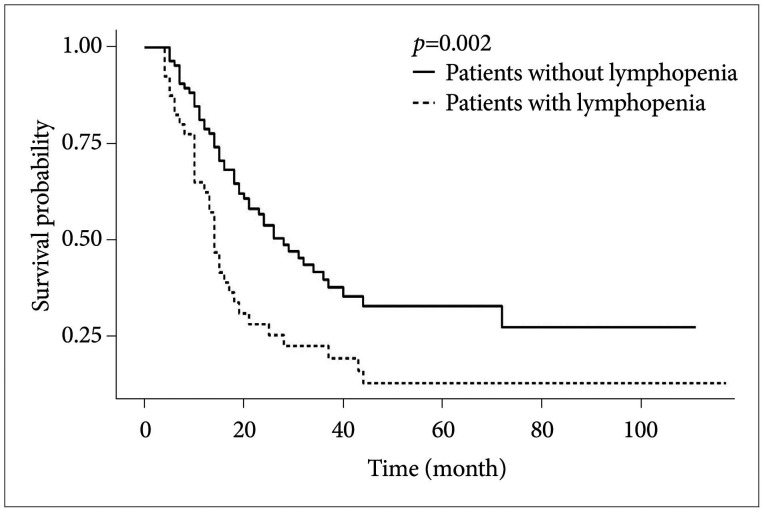
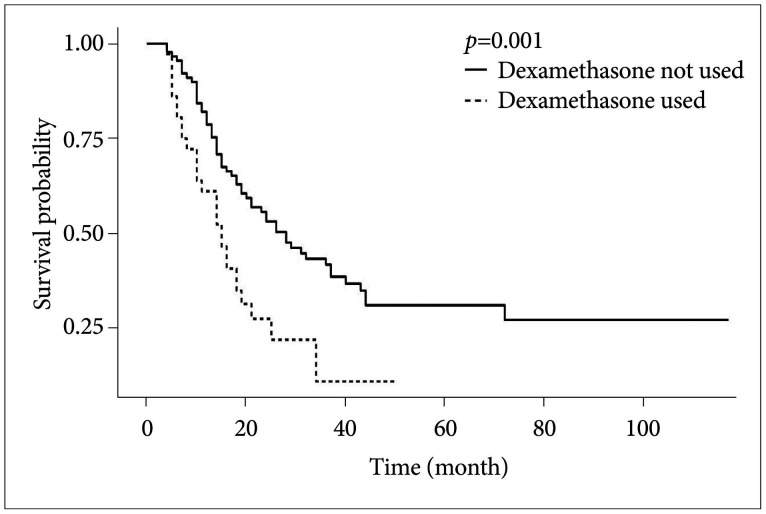
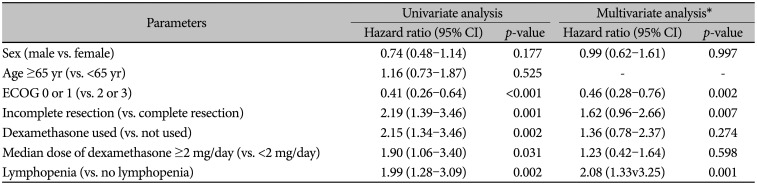
Kaplan-Meier analysis and multivariate Cox regression analysis with previously identified prognostic factors were performed to evaluate the effect of lymphopenia and higher use of dexamethasone on OS (Table 2). The Kaplan-Meier curves showed that the median OS of patients with lymphopenia was shorter than that of patients without lymphopenia (14.0 months vs. 28.0 months, p=0.002) (Fig. 1) and the median OS of patients who took dexamethasone was shorter than that of patients who did not take dexamethasone (15.0 months vs. 28.0 months, p=0.001) (Fig. 2). On multivariate analysis, lymphopenia (<1,000 cells/µL) was independently associated with shorter survival (HR 2.08, p<0.001), while dexamethasone use alone and dexamethasone dose greater than 2 mg/day were not. Well-known prognostic factors, including non-GTR and an ECOG score of 2 or more, were significantly associated with shorter survival (HR: 1.62, p=0.007, and HR: 0.46, p=0.002).
Lymphopenia and risk factors
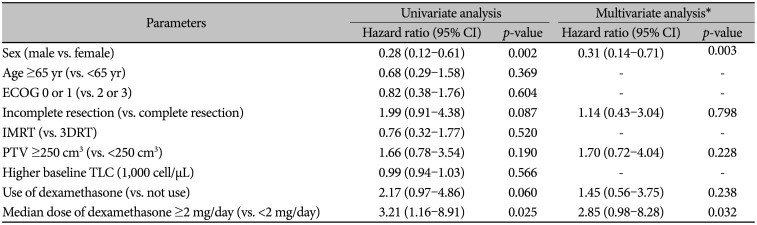
Multivariate logistic regression was performed to identify independent clinical factors associated with lymphopenia (Table 3). Female sex and dexamethasone dose greater than 2 mg per day were independently associated with lymphopenia (male vs. female, HR: 0.31, p=0.003, and HR: 2.85, p= 0.032, respectively), while use of dexamethasone regardless of dose was not associated with lymphopenia (HR 1.45, p=0.238). Older age, non-GTR, PTV, RT modality, and baseline TLC count were not associated with lymphopenia.
DISCUSSION
In our study, we showed that lymphopenia was an independent prognostic factor in terms of OS as were already well-known parameters including EOR and performance status. We also found that female sex and median daily dexamethasone dose greater than 2 mg from initiation of CCRT to 4 weeks after completion of CCRT were independently associated with lymphopenia in patients with newly diagnosed GBM. However, dexamethasone dose less than 2 mg/day, EOR, baseline TLC, RT modality (IMRT vs. 3DRT), and PTV were not significantly associated with lymphopenia. In addition, the use of dexamethasone, regardless of dose, was not independently associated with OS.
Dexamethasone, as a synthetic glucocorticoids, bind to the glucocorticoid receptor, which is expressed in almost all immune cells [26]. Recent preclinical experiments using conditional glucocorticoid receptor-knockout mice as well as transgenic mice showed effects of glucocorticoid on immune and inflammatory responses [272829]. In the thymus, glucocorticoid induced apoptosis of naïve T cell and resulted in regulation of T cell number and function during development [2728]. In the periphery, glucocorticoid also promoted apoptosis of T cells in lymphoid organs and limited the migration activity of T cells to the site of inflammation [29].
Huang et al. [11] showed that acute severe lymphopenia was associated with higher brain volume receiving 25 Gy (V25Gy) [odds ratio (OR): 1.03, CI: 1.003–1.05], female sex (OR: 5.30, CI: 2.46–11.41), older age (OR: 1.05, CI: 1.02–1.09), and lower baseline TLC (OR: 0.92, CI: 0.87–0.98) in patients with high grade glioma who were treated with RT and TMZ chemotherapy. Rudra et al. [14] also found that higher brain volume receiving 25 Gy (OR: 1.048, CI: 1.022–1.074), older age (OR: 1.091 CI: 1.047–1.137), and female sex (OR: 2.901, CI: 1.391–6.047) were independently associated with acute severe lymphopenia in patients with GBM treated with CCRT. In addition, Lin et al. [15] found that older age (OR: 1.06, CI: 1.02–1.10), female sex (OR: 10.08, CI: 3.79–30.5), and TMZ use (OR: 72.3, CI: 7.8–679) were independently associated with lymphopenia after RT and/or TMZ in patients with high grade glioma. However, these three studies did not find that dexamethasone use was associated with lymphopenia. A recent study published by Hui et al. [17] calculated the cumulative exposure of dexamethasone during CCRT and showed that increased use of dexamethasone was independently associated with acute severe lymphopenia and OS. Chitadze et al. [13] showed that dexamethasone affects various immune cell parameters not including TLC in GBM patients. Based on our findings and previous reports, female sex seemed to be strongly associated with lymphopenia. Further investigation is needed to determine why females showed more frequent lymphopenia than males.
In this study, we calculated the overall cumulative dose of dexamethasone from initiation of CCRT to 4 weeks after completion of CCRT (the day before starting the first round of adjuvant TMZ chemotherapy), which was also the same date blood samples were collected for calculating TLC. Most of the studies mentioned above included only baseline dose of dexamethasone and did not include overall cumulative dose from initiation of CCRT until blood sampling. We found that a median daily dexamethasone dose greater than 2 mg from initiation of CCRT until the start of the first round of adjuvant TMZ chemotherapy was independently associated with lymphopenia, while a dexamethasone dose less than 2 mg per day was not.
Our findings provide evidence that higher cumulative dexamethasone dose during CCRT in patients with newly diagnosed GBM could be a significant risk factor for developing lymphopenia. A large body of evidence from preclinical and clinical studies in other cancers supports the adverse effect of dexamethasone on patient immunity [203031]. However, the use of dexamethasone itself was not independently associated with OS in our study. This may be due to other confounding factors and a larger prospective analysis considering various confounding factors is needed to further evaluate the potential relationship between dexamethasone use and lymphopenia.
Our study had several limitations. There is a possibility of selection bias due to its retrospective and non-randomized design. Molecular parameters, such as MGMT gene methylation, IDH1, and 1p19q co-deletion were not fully identified. More patients in the dexamethasone group underwent non-GTR surgery. Remaining microscopic and/or macroscopic tumor cells could also have induced immunosuppression. Further investigation of the immunosuppressive effect of remnant tumor cells is needed, although a higher dose of dexamethasone was independently associated with acute lymphopenia in our study.
In conclusion, use of dexamethasone itself after initiation of CCRT until 4 weeks after completion of CCRT was not associated with developing lymphopenia at 4 weeks after completion of CCRT. However, the median daily dexamethasone dose ≥2 mg was independently associated with lymphopenia. These results should be validated by further prospective studies.
 XML Download
XML Download