

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Guideline Working Group of Korean Society for Neuro-Oncology (KSNO) conducted a nationwide questionnaire survey on the clinical practice about several topics of brain tumor. The intent of this survey study is described in the previous article of the series in this issue. As part III of the survey, this study deals with practical decisions in the management of brain metastasis and primary central nervous system lymphoma (PCNSL).
Brain metastases are the most common CNS tumors, with up to 30–40% of cancer patients developing brain metastases [1]. The management of brain metastases varies according to accessibility for surgical management, number of lesions, patients' clinical status, and physicians' preferences. According to National Comprehensive Cancer Network (NCCN) guidelines, surgery is recommended for a limited number of metastases with lower level evidence (category 2A) [2], but no solid management guideline exists for extensive metastases or recurrent disease. A paucity of evidence and different clinical situations formed varied practice patterns across centers [3], and key questions for management strategies for brain metastases include following: single metastasis with or without surgical accessibility, disease status with or without systemic involvement, and local or multiple recurrence after initial therapy.
PCNSL is a rare brain tumor and represents 3–4% of all brain tumors [4]. PCNSL is a highly aggressive non-Hodgkin lymphoma that is typically restricted to the brain, spine, cerebrospinal fluid (CSF), and eyes without evidence of systemic spread [5]. High-dose methotrexate (HD-MTX) plus consolidation chemotherapy and/or whole brain radiotherapy (WBRT) is the mainstay of standard of care for newly diagnosed PCNSL [6]. However, the optimal treatment regimen has yet to be defined. In addition, no consensus exists for refractory and relapsed PCNSL. Questions in this study deal with current controversies including the optimal chemotherapy regimen, the role of radiation, the salvage management, and treatment of the CSF space [5].
The aim of this study is to evaluate the current status of clinical practice for patients with brain metastasis and PCNSL from the nationwide survey in Korea.
MATERIALS AND METHODS
The details of the study design, outline, and implementation are described in the previous article of the series in this issue. Here, the questionnaires about brain metastases (7 questions) and PCNSL (5 questions) were structured around existing controversies regarding real clinical management in patients (Appendix).
Regarding to the brain metastasis, the survey questions dealt with the following specific situations related with the management plan of brain metastasis patient: 1) Single brain metastasis (initial management) depending on size; 2) Multiple brain metastases (initial management) depending on symptom, location, and number of lesions; 3) Progressive single brain metastasis with a failure of initial management; and 4) Progressive multiple brain metastases.
As for the PCNSL, the questionnaires were structured general questions focused on the diagnostic work-ups and treatment options. All responses were analyzed descriptively as well as quantitatively wherever appropriate.
RESULTS
Brain metastasis
The results of a survey on single brain metastasis management options are shown in Fig. 1. For patients with a surgically accessible single brain metastatic lesion with size less than 3 cm in diameter, 32 of 49 (65.3%) respondents preferred the surgical resection without (n=4) or with postoperative managements such as, chemotherapy (n=2), WBRT (n=5), and radiation boost to the surgical cavity (n=21). Seventeen (34.7%) respondents have chosen radiosurgery (n=16) and localized radiotherapy (n=1) without surgery as an initial treatment for the same lesion. However, if the patient has a surgically inaccessible single brain metastatic lesion less than 3 cm in diameter without any other evidence of systemic disease, most respondents (n=44, 89.8%) preferred the radiosurgery (including fractionated method) than localized radiotherapy (n=4, 8.2%) or WBRT (n=1, 2.0%).
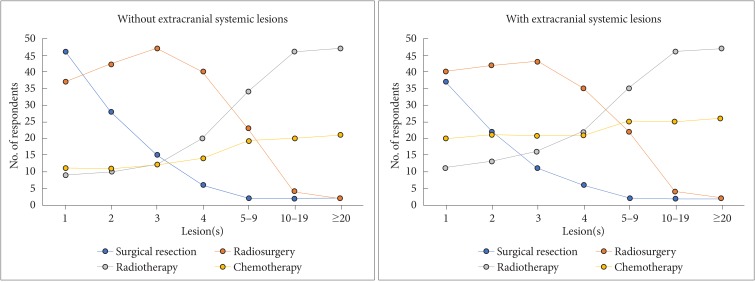
For those patients with multiple brain metastases but if one of the lesions is showing mass effect and surgically accessible, most respondents (n=42, 85.7%) choose the surgical resection of the mass of interest followed by adjuvant treatment for the other lesions with radiosurgery in 8.2% (n=4), or radiotherapy in 6.1% (n=3). There was similar tendency for choosing treatment modalities according to the number of lesions between conditions having extracranial metastases or not (Fig. 2). Respondents considered the radiotherapy as the number of brain lesions increased, and the radiosurgery was mainly chosen at the brain metastases of less than or equal to 4. The consideration of chemotherapy combination increased when there were extracranial systemic lesions.
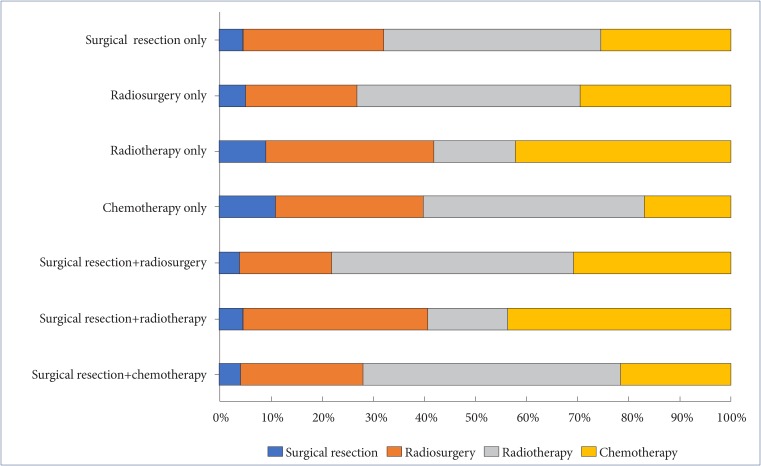
For enlarging single brain metastasis, which had been treated with radiosurgery or radiotherapy 3 months ago, respondents considered the following options: short-term follow-up MRI within 1 or 2 months (n=31, 63.3%); decision-making after further work-up such as positron emission tomography (PET) and MR perfusion (n=7, 14.3%); surgical resection followed by adjuvant treatment such as radiotherapy, radiosurgery, and chemotherapy (n=4, 8.2%); surgical resection only (n=4, 8.2%). Fig. 3 shows preference of respondents for the treatment strategies for patients with developing multiple brain metastases after treatment of single brain metastasis according to previously treated modality. Localized radiotherapy or WBRT was the mainstay of the multiple metastases (n=36–38, 78.3–84.4%), regardless the patients were treated with surgery, radiosurgery, or chemotherapy. When the patients had a history of radiotherapy, radiosurgery (n=22, 48.9%) was considered. Chemotherapy was preferred as combined therapy for radiosurgery, radiotherapy, and surgery.
PCNSL
Respondents were answered to consider following diagnostic work-ups to identify the extent of PCNSL; brain MRI scan (including enhance, diffusion and perfusion images) (n=46, 100%), ophthalmologic evaluation (n=38, 82.6%), whole-body PET scan (n=36, 78.3%), chest and/or abdominopelvic CT scan (n=32, 69.6%), spine MRI scan (if symptomatic) (n=31, 67.4%), CSF analysis (n=31, 67.4%), brain CT scan (n=25, 54.3%), bone marrow biopsy (n=17, 37.0%), testicular ultrasound for men >60 years (n=11, 23.9%), and serum LDH (n=1, 2.2%).
It was surprising to see that there is still a weak consensus on the initial management protocol for PCNSL. As a first-line induction therapy for PCNSL, 22 of 44 (50.0%) respondents considered HD-MTX-based polychemotherapy with (n=5) or without rituximab (n=17). Sixteen (36.4%) respondents used single-agent HD-MTX and six (13.6%) choose WBRT with or without chemotherapy. As the consolidation therapy for those patients showing complete response after induction therapy, 18 of 40 (42.5%) respondents choose high-dose WBRT at 45 Gy (n=3) or low-dose WBRT at 23–24 Gy (n=15). One respondent stated that the low-dose WBRT was given only to young patients. However, 19 of 40 (47.5%) respondents considered chemotherapy as the consolidation therapy. The regimens were as followings: continuing HD-MTX based chemotherapy (n=12); high-dose chemotherapy with autologous stem cell transplantation (ASCT) (n=6); conventional chemotherapy using cytarabine, etoposide plus cytarabine, or others (n=1). Three respondents (7.5%) choose the close observation without consolidation therapy.
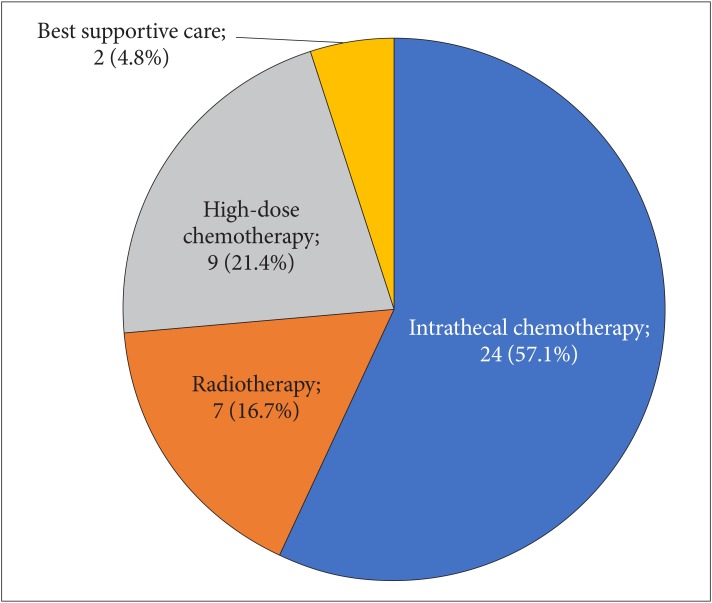
As the salvage therapy for patients showing partial response (PR), progressive disease (PD), and recurrence after induction therapy, 14 of 42 (33.3%) respondents choose the WBRT with (n=3) or without local boost (n=11). Sixteen (38.1%) respondents choose the HD-MTX based chemotherapy and WBRT rechallenge and four (9.5%) respondents choose the single or combined chemotherapy using temozolomide, pemetrexed, topotecan, or rituximab. Four (9.5%) respondents considered ASCT and three (7.1%) considered the clinical trial. In free text response, one respondent stated that chemotherapy was performed for patients with PR or PD, and WBRT was performed for recurred patients. Fig. 4 shows the preferred management of respondents for PCNSL patients with CSF dissemination.
DISCUSSION
The majority of practice patterns for single brain metastasis in Korea was consistent with the NCCN guideline. The mainstay of management for accessible single metastasis was surgery (65.3%) with or without adjuvant radiation at the surgical cavity, followed by radiosurgery (32.7%). This is in line with current evidence that the local control rate of brain metastases was comparable between radiosurgery and surgical resection group [7]. The preference options for the management for single brain metastasis was similar to those from international survey by radiation oncologists [3] who had chosen surgery and WBRT (40%), radiosurgery and WBRT (17%), and radiosurgery alone (14%).
Interestingly, surgery was preferred (85.7%) for the symptomatic lesion among the multiple metastases when it is surgically accessible. This result is different from an international survey by radiation oncologists that 53% would not offer surgery but give WBRT for multiple brain metastases [3]. The reason for that is the main respondents of our survey was neurosurgeons (66.7%), followed by radiation oncologists (24.1%).
Imaging findings after radiotherapy and radiosurgery can be confounded by treatment effects [8]. Physicians preferred to repeat scan with short-term interval of 1–2 month rather than additional advanced MRI or PET for enlarging single metastasis after radiosurgery or radiotherapy. When diagnosed with multiple recurrences, localized radiotherapy or WBRT was the most preferred treatment option, combination with chemotherapy.
PCNSL is usually present as a single brain lesion, but sometimes involves eyes, CSF, and rarely the spinal cord [9]. Thorough clinical evaluation of PCNSL is mandatory to assess the extent of the disease and to treat patients. Practical guidelines from the NCCN and European Association for Neuro-Oncology (EANO) commonly recommend ophthalmologic exam, CSF exam, spine MRI (if symptomatic), chest/abdominopelvic CT or whole-body PET/CT scan, bone marrow biopsy (lower level evidence), and testicular sonography (lower level evidence) [10]. The result of the survey in terms of clinical evaluation is generally in accordance with NCCN and EANO guidelines while both bone marrow biopsy and testicular sonography are performed less frequently.
In this survey, HD-MTX based chemotherapy with or without other chemotherapeutic agents is revealed as a main strategy for the induction therapy. In prospective studies, HD-MTX chemotherapy yielded a 52–100% response rate, while HD-MTX-based polychemotherapy resulted in 65–100% response rate [6,11,12,13]. NCCN and EANO guidelines recommend that chemotherapy should include HD-MTX at doses of at least 3g/m2 [10]. Interestingly, a minority of respondents use polychemotherapy including rituximab, a monoclonal antibody directed against CD20 of the B-cell for CD20 positive PCNSL. The result of the IELSG32 phase 2 trial suggests that the combination of HD-MTX, cytarabine, thiotepa, and rituximab (MATRix regimen) as the first-line treatment improves overall response rates [14]. To date, the level of evidence supporting the use of rituximab as part of protocol remains low, but several trials are ongoing to verify that addition of rituximab to induction therapy is beneficial [10].
Nearly half of clinicians choose the WBRT, especially low-dose WBRT, as a main strategy for consolidation in this survey. In the largest and only phase 3 trial (G-PCNSL-SG 1) comparing consolidation WBRT to observation alone, the overall survival was similar in patients underwent WBRT and those who did not [15]. In addition, high-dose WBRT negatively impacts on quality of life without the survival benefit in patients with PCNSL [16]. In accordance with the survey result, practical guidelines recommend reduced-dose consolidation radiotherapy. Consolidation therapies based on continued HD-MTX chemotherapy, high-dose chemotherapy combined with ASCT, or other chemotherapeutic regimens are also revealed as preferred treatment options in practice.
Despite advances in first-line treatment, half of respondent relapse and a third of PCNSL patients have primary refractory disease [6]. The salvage regimen is poorly defined and varied widely including HD-MTX rechallenge, temozolomide, topotecan, WBRT, rituximab, ASCT, and so on [17]. As the survey result for the salvage treatment, HD-MTX rechallenge or WBRT for those who have not received previously seems to be effective in retrospective studies [18,19]. For the CSF disseminated disease, more than half of respondents choose intrathecal chemotherapy although no consensus exists regarding the role of intrathecal chemotherapy until now. Overall decision of salvage treatments should have been made based on patients' situation and clinicians' experiences.
As with any online survey, the major limitation of this study is response bias that respondents might be influenced by the pressure to follow the published guidelines, especially in the survey of PCNSL because of relatively few medical oncologists of the KSNO members. Additionally, the relatively low response rate may give rise to sampling bias interfering with the valuable interpretation of several questions.
In conclusion, the survey demonstrates the variation and similarity of clinical practice for patients with brain metastasis and PCNSL among members of the KSNO. We could draw important issues to be studied for the establishment of guidelines based on the best available evidence.

 XML Download
XML Download